

Abstract
Adequate calcium intake during pregnancy is important in the prevention of pre‐eclampsia. A substantial proportion of pregnant women do not meet the recommended daily calcium intake, even in developed countries. Nonetheless, calcium supplementation is not routinely advised to pregnant women in most countries. We aimed to predict the impact of advising pregnant women to use calcium supplements (1,000 mg/day) on the number of cases of pre‐eclampsia prevented and related health care costs. By use of a decision‐analytic model, we assessed the expected impact of advising calcium supplementation to either (1) all pregnant women, (2) women at high risk of developing pre‐eclampsia, or (3) women with a low dietary calcium intake compared with current care. Calculations were performed for a hypothetical cohort of 100,000 pregnant women living in a high‐income country, although input parameters of the model can be adjusted so as to fit other settings. The incidence of pre‐eclampsia could be reduced by 25%, 8%, or 13% when advising calcium supplementation to all pregnant women, women at high risk of pre‐eclampsia, or women with a low dietary calcium intake, respectively. Expected net financial benefits of the three scenarios were of €4,621,465, €2,059,165, or €2,822,115 per 100,000 pregnant women, respectively. Advising pregnant women to use calcium supplements can be expected to cause substantial reductions in the incidence of pre‐eclampsia as well as related health care costs. It appears most efficient to advise calcium supplementation to all pregnant women, not subgroups only.
Keywords: calcium supplementation, decision analysis, impact, pre‐eclampsia
1. INTRODUCTION
Calcium supplementation is a promising intervention for the prevention of pre‐eclampsia (PE). A meta‐analysis of 13 randomized controlled trials comprising 15,730 pregnant women, showed an overall reduction of 55% in the risk of PE among women receiving calcium supplements (>1,000 mg/day) from the second half of pregnancy to delivery as compared to women receiving placebo supplements (risk ratio (RR), 0.45; 95% confidence interval (95% CI), 0.31–0.65) (Hofmeyr, Lawrie, Atallah, Duley, & Torloni, 2014). The risk reduction was more pronounced among women with an increased risk of hypertensive disorders (RR 0.22, 95% CI 0.12–0.42, five trials) and among women with a low dietary calcium intake (mean intake <900 mg/day) (RR 0.36, 95% CI 0.20–0.65, eight trials).
Calcium supplementation of 1,000 mg/day (elemental) costs about €50 per pregnancy (British National Formulary, 2016; Zorginstituut Nederland, 2016). Side effects are uncommon and usually mild (Heaney et al., 2012; Hofmeyr et al., 2014). Despite its documented protective effect, relative cheapness, and safety, calcium supplementation is still not part of standard antenatal care in most countries. The World Health Organization recommends calcium supplementation as part of antenatal care in populations where calcium intake is low (WHO, 2013).
Recommended calcium intake for pregnant women varies between 900 and 1,200 mg/day, depending on the country (EFSA NDA PANEL, 2015; IOM, 2011). Actual intake among pregnant women often does not meet the recommendation, even in countries with sufficient availability and affordability of calcium‐rich foods (Merialdi et al., 2005). For instance, in a recent Dutch pregnancy cohort study, mean maternal dietary calcium intake was 1,108 mg/day with a standard deviation of 311 mg, indicating that more than one‐third of the women had an intake below 1,000 mg/day (Heppe et al., 2013). The contribution of calcium‐containing supplement use to total daily calcium intake is low (Bailey et al., 2010; Van Rossum, Fransen, Verkaik‐Kloosterman, Buurma‐Rethans, & Ocké, 2011).
Although adequate calcium intake through calcium‐rich foods should be encouraged, available experimental evidence implies that calcium supplementation, either among all pregnant women or selected subgroups, could yield important health gains. Other factors, however, also contribute to the eventual success of implementing calcium supplementation in antenatal care. These include the size of the target population, the incidence of PE, the percentage of women already taking calcium supplements, and the uptake of the intervention. As to financial impact, costs of calcium supplements and savings due to prevented cases of PE should be taken into account.
The aim of this study was to predict the impact of advising pregnant women to use calcium supplements (1,000 mg/day) on the number of cases of PE prevented and related health care costs.
Key messages.
Adequate calcium intake during pregnancy is important in the prevention of pre‐eclampsia.
A substantial proportion of pregnant women have a daily calcium intake below the recommended value, even in developed countries.
Our findings, based on the best available evidence, provide support for advising calcium supplementation during pregnancy as it can cause substantial reductions in the incidence of pre‐eclampsia and related health care costs.
It appears most efficient to advise calcium supplementation to all pregnant women, not subgroups only.
2. MATERIALS AND METHODS
2.1. Analytical model
We assessed the expected impact of advising calcium supplementation (1000 mg/day), from 20 weeks of pregnancy to delivery, to (1) all pregnant women, (2) women at high risk of developing PE, or (3) women with a low dietary calcium intake (<900 mg/day). We designed a simple decision‐analytic model for the comparison of these three scenarios with current care (Figure 1) (Petrou & Gray, 2011). The patient population was a hypothetical cohort of 100,000 pregnant women living in a high‐income country such as the Netherlands. Variables used in the model were the following: size of the target population, incidence of PE, efficacy of calcium supplementation during pregnancy, estimated number of women currently using calcium supplements, expected compliance with the advice, cost of one case of PE (in‐hospital costs for both mother and baby from diagnosis of PE until discharge from hospital after delivery), and cost of calcium supplements per pregnancy.
Figure 1.
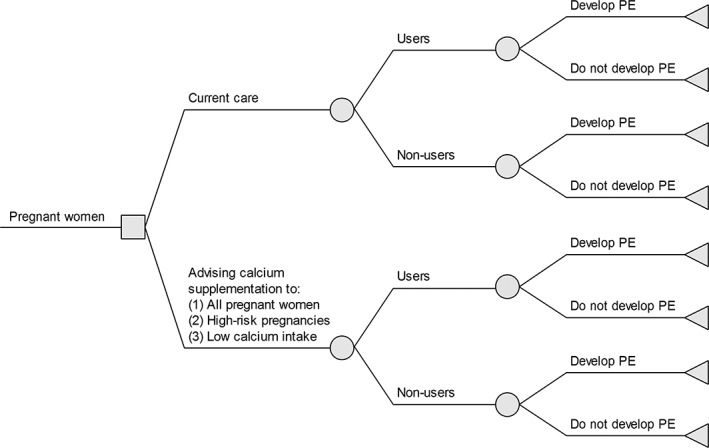
Decision tree comparing current care with advising calcium supplementation (1,000 mg/day) to different scenarios in the prevention of pre‐eclampsia. PE = pre‐eclampsia. Legend: The decision tree illustrates the comparison of current care with advising calcium supplementation (1,000 mg/day) to (1) all pregnant women, (2) women at high risk of developing pre‐eclampsia, or (3) women with a low dietary intake (<900 mg/day) in the prevention of pre‐eclampsia
The model was developed in Microsoft Excel and is available as supplementary material.
2.2. Data sources
We obtained base‐case values and reported ranges of the relevant input parameters from published literature and government reports. Where no specific evidence was available, we employed conservative estimates based on related information from the literature or input from clinical experts.
The eligible population modeled reflects the Dutch pregnant population. No data source was available for the number of women at high risk of developing PE, as this is also dependent on the definition of high risk. We made a conservative estimate based on interviews with Dutch obstetricians. The number of pregnant women with a low dietary calcium intake was estimated on data from a Dutch birth cohort study and data from the Dutch National Food Consumption Survey among women of reproductive age (Heppe et al., 2013; Van Rossum et al., 2011). The incidence of PE was obtained from a nationwide Dutch cohort study, as the Dutch perinatal registry (Perined) has no reliable data about the exact incidence of PE (Von Schmidt auf Altenstadt, Hukkelhoven, van Roosmalen, & Bloemenkamp, 2013). PE incidence data among women at high risk of developing PE and women with low dietary calcium intake were acquired from international literature studies (Duley, Henderson‐Smart, Meher, & King, 2007; Hofmeyr et al., 2014; Meads et al., 2008). The effect sizes of calcium supplementation in the prevention of PE in the different target populations were obtained from the most recently published systematic review (Hofmeyr et al., 2014). The number of pregnant women currently using calcium supplements during pregnancy was estimated on the basis of data from the Dutch National Food Consumption Survey among women of reproductive age, survey among pregnant women in Australia, and interviews with Dutch obstetricians (Forster, Wills, Denning, & Bolger, 2009; Van Rossum et al., 2011). No data source was available on the uptake of the advice to use calcium supplements during pregnancy as this is no recommendation yet in Dutch obstetric care. We made a conservative estimate based on Dutch data about the use of folic acid supplementation during pregnancy (Sikkens, van Eijsden, Bonsel, & Cornel, 2011; Woude, Walle, & Berg, 2012).
For calculating the financial impact outcomes, in‐hospital cost of one case of PE was derived from a review containing an economic evaluation of tests and treatments on PE (Meads et al., 2008). Cost of calcium supplements per pregnancy was obtained from Care Institute Netherlands which calculates drug costs based on the actual Pharmacy Purchase Price (Zorginstituut Nederland, 2016).
The values and sources of all clinical and financial input parameters are summarized in Table 1.
Table 1.
Overview of input parameters
| Model parameter | Base‐case value | Plausible range for sensitivity analysis | Source | |
|---|---|---|---|---|
| Low | High | |||
| • Cohort size (i.e., number of pregnant women) (n) | 100,000 | — | — | — |
| • Incidence of pre‐eclampsia (%) | 3 | 2 | 5 | Von Schmidt auf Altenstadt et al., 2013. |
| • Risk ratio of pre‐eclampsia for calcium supplementation versus no calcium supplementation among all pregnant women | 0.45 | 0.31 | 0.65 | Hofmeyr et al., 2014. |
| • Current use of calcium supplements among all pregnant women (%) | 5 | 2.5 | 10 | Assumption based on expert interviews, Forster et al., 2009, and Van Rossum et al., 2011. |
| • Users of calcium supplements after implementing the advice among all pregnant women (%) | 50 | 25 | 75 | Assumption based on Sikkens et al., 2011 and Woude et al., 2012. |
| Subgroup pregnant women at high risk of developing pre‐eclampsia | ||||
| • Pregnant women at high risk of developing pre‐eclampsia (% of total pregnant women) | 10 | 5 | 15 | Assumption based on expert interviews. |
| • Incidence pre‐eclampsia among pregnant women at high risk of developing pre‐eclampsia (%) | 7.5 | 5 | 10 | Duley et al., 2007 and Meads et al., 2008. |
| • Risk ratio of pre‐eclampsia for calcium supplementation versus no calcium supplementation among pregnant women at high risk of developing pre‐eclampsia | 0.22 | 0.12 | 0.42 | Hofmeyr et al., 2014. |
| • Current use of calcium supplements among pregnant women at high risk of developing pre‐eclampsia (%) | 10 | 5 | 20 | Assumption based on expert interviews, Forster et al., 2009 and Van Rossum et al., 2011. |
| • Users of calcium supplements after implementing the advice among pregnant women at high risk of developing pre‐eclampsia (%) | 50 | 25 | 75 | Assumption based on Sikkens et al., 2011 and Woude et al., 2012. |
| Subgroup pregnant women with a low dietary calcium intake | ||||
| • Pregnant women with a low dietary calcium intake (<900 mg/day) (% of total pregnant women) | 25 | 15 | 40 | Van Rossum et al., 2011 and Heppe et al., 2013. |
| • Incidence pre‐eclampsia among pregnant women with a low dietary calcium intake (%) | 5.5 | 4 | 7 | Hofmeyr et al., 2014. |
| • Risk ratio of pre‐eclampsia for calcium supplementation versus no calcium supplementation among pregnant women with a low dietary calcium intake | 0.36 | 0.20 | 0.65 | Hofmeyr et al., 2014. |
| • Current use calcium supplements among pregnant women with a low dietary calcium intake (%) | 10 | 5 | 20 | Assumption based on expert interviews, Forster et al., 2009 and Van Rossum et al., 2011. |
| • Users of calcium supplements after implementing the advice among pregnant women with a low dietary calcium intake (%) | 50 | 25 | 75 | Assumption based on Sikkens et al., 2011 and Woude et al., 2012. |
| Costs | ||||
| • In‐hospital cost of one case of pre‐eclampsia | €9,000 | €6,000 | €12,000 | Meads et al., 2008. |
| • Cost of calcium supplements per pregnancy | €50 | €35 | €65 | Zorginstituut Nederland, 2016. |
2.3. Outcome measures
With the model, we calculated the changes in health outcomes between the new scenarios and current care in terms of absolute reduction, relative reduction, and number needed to advise. The absolute reduction was defined as the difference in the number of cases of PE between the new scenario and current care, and relative reduction as the percentage difference in incidence of PE between the new scenario and current care. The number needed to advise was calculated as the average number of pregnant women that need to be advised to use calcium supplements in the new scenario to prevent one case of PE compared with current care.
The financial impact of prevented cases of PE in the new scenario compared to current care was calculated by multiplying the absolute reduction by unit cost of one case of PE. The extra cost of calcium supplements was defined as the additional cost of calcium supplements in the new scenario compared to current care. The net financial impact was calculated from a public payer's perspective by subtracting extra cost of calcium supplements from the financial impact of prevented cases of PE. Financial quantities were expressed in euros (€). No discounting was applied to either costs or clinical outcomes. Time horizon, in line with the timing used in the meta‐analysis, spanned the 20th weeks of pregnancy until discharge of mother or child from hospital after delivery (Hofmeyr et al., 2014).
2.4. Sensitivity analysis
One‐way sensitivity analyses were performed for each scenario to evaluate the impact of variations of values of model input parameters on the absolute reduction and net financial impact. Input parameters were varied one at a time within a plausible range around the base‐case value based on literature review or realistic assumptions. Ranges used for the sensitivity analyses are presented in Table 1. The results of the sensitivity analyses were plotted in tornado diagrams using R version 3.2.3.
3. RESULTS
3.1. Base‐case
Table 2 presents the expected number of PE prevented and related health care costs for the three scenarios compared to current care in a hypothetical cohort of 100,000 pregnant women.
Table 2.
The expected impact on prevented cases of pre‐eclampsia and related health care costs of advising calcium supplementation during pregnancy—a comparison of three scenarios with current care
| Current care | Scenarios—advising calcium supplementation to: | |||
|---|---|---|---|---|
| (1) all pregnant women (n = 100,000) | (2) pregnant women at high risk of pre‐eclampsia (n = 10,000) | (3) pregnant women with a low dietary calcium intake (n = 25,000) | ||
| Cohort | ||||
| Number of pregnant women (n) | 100,000 | 100,000 | 100,000 | 100,000 |
| Users of calcium supplements (n) | 5,000 | 50,000 | 9,500 | 16,250 |
| Cases of pre‐eclampsia (n) | 3,000 | 2,237 | 2,746 | 2,624 |
| Clinical impact cases of pre‐eclampsia | ||||
| Absolute reduction (n) | 763 | 254 | 376 | |
| Relative reduction (%) | 25 | 8 | 13 | |
| Number needed to advise (n) | 131 | 39 | 66 | |
| Financial impact | ||||
| Cost savings from prevented cases of pre‐eclampsia | €6,871,465 | €2,284,165 | €3,384,615 | |
| Extra cost of calcium supplements | €2,250,000 | €225,000 | €562,500 | |
| Net financial impact | +€4,621,465 | +€2,059,165 | +€2,822,115 | |
In current care, PE complicates 3% of all pregnancies (3,000/100,000). The base‐case analysis indicated that if calcium supplementation is advised to all pregnant women (n = 100,000) (scenario 1), 763 cases of PE will be prevented (i.e., relative reduction of 25%). The estimated net financial benefit (savings minus costs of calcium supplements) was €4,621,465 per 100,000 pregnant women.
If calcium supplementation is advised to subpopulations of pregnant women at high risk of PE (scenario 2) or pregnant women with a low dietary calcium intake (scenario 3), an estimated 254 and 376 cases of PE will be prevented, respectively, and estimated net benefits amount to €2,059,165 and €2,822,115. The numbers needed to advise is lowest in scenario 2 and highest in scenario 1.
3.2. Sensitivity analysis
One‐way sensitivity analyses performed for the different scenarios are illustrated in Figure 2. The results indicated that calcium supplementation during pregnancy is both clinically and financially beneficial within all plausible ranges. The strongest influence was found for the number of users of calcium supplements in the new scenarios and the efficacy of the use of calcium supplements. In scenarios 2 and 3, results were additionally influenced by the size of the subpopulation, with larger impacts in case of larger target populations.
Figure 2.
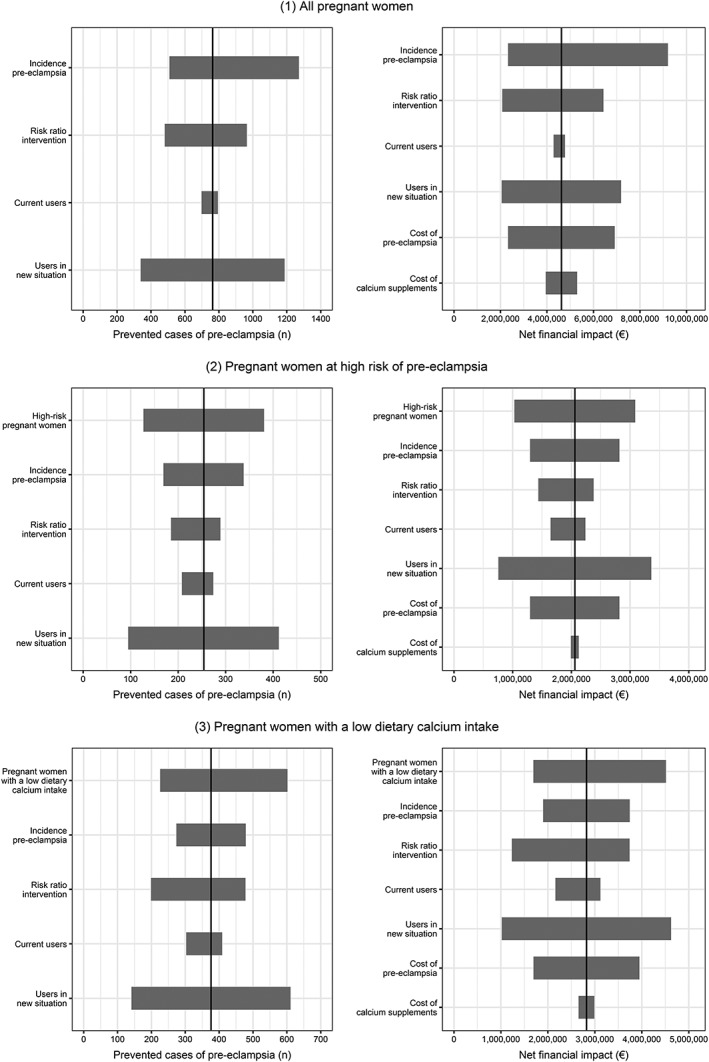
Tornado diagrams of one‐way sensitivity analyses results for prevented cases of pre‐eclampsia and net financial impact, per 100,000 pregnant women. Legend: The vertical line in the center of the chart represents the prevented cases of pre‐eclampsia or net financial impact for the base‐case values. The bars show the variation of input parameters within plausible ranges
4. DISCUSSION
4.1. Main findings
The results of our decision analysis indicate that advising calcium supplementation to all pregnant women, pregnant women at high risk of PE, or pregnant women with a low dietary calcium intake can be expected to reduce the incidence of PE by 25%, 8%, or 13%, respectively. Expected net financial benefits are €4,621,465, €2,059,165, or €2,822,115 per 100,000 pregnant women. Although clinical and financial benefits may vary with varying parameter estimates, it is implausible that effects will be reversed.
4.2. Strengths and limitations
Translation of efficacious preventive interventions to clinical practice remains a challenge (Glasgow, Lichtenstein, & Marcus, 2003). Randomized controlled trials may not represent real‐world conditions and do not by themselves yield sufficient information for inference on the population impact of implementing an intervention. Decision analysis, combining evidence from efficacy studies with that of various other sources, is necessary in order to provide insight to caregivers, budget holders, policy makers, and health insurance companies as to whether an efficacious intervention is attractive for implementation.
Other researchers have estimated the clinical and financial impact of diagnostic or preventive interventions to reduce pregnancy complications (Bajaj & Veenstra, 2013; Darmstadt et al., 2005; Hadker, Garg, Costanzo, van der Helm, & Creeden, 2013; Hadker et al., 2010; Meads et al., 2008; Zechmeister‐Koss & Piso, 2014). Meads et al. (2008) also considered the cost‐effectiveness of calcium supplementation in the prevention of PE but under less realistic assumptions, namely that in current care no pregnant women use calcium supplements and that the uptake of the intervention would be 100%.
We recognize that although we have used the best evidence for obtaining accurate input values, our analysis is limited by the availability and quality of existing evidence. We derived the effect estimate of calcium supplementation from a high GRADE systematic review (Hofmeyr et al., 2014). As the authors of that review noted, overall effects may be overestimated due to stronger effects found in smaller studies (which predominantly included high‐risk women), or publication bias. Also, different effects of calcium supplementation may be expected across populations with different baseline levels of calcium intake. However, as evidenced by our sensitivity analysis, even more modest effects can be expected to yield considerably favorable effects on population health as well as economic outcomes.
For the few parameters for which no evidence was available, we attempted to take account for the uncertainty by staying conservative when determining the base‐case values, so as not to obtain overoptimistic results. We also performed sensitivity analyses, the results of which did not reveal a dependency of the conclusions on variation of the input values within all plausible ranges.
We did not take into account investments for implementation of the intervention. Therefore, the expenditure is expected to be higher depending on the extent of the efforts, particularly in the first years of implementation. On the other hand, we also did not consider long‐term costs for mother and child due to PE (e.g., costs related to neurodevelopmental impairment of children born preterm or to cardiovascular disease in the mother), as these are problematic to quantify (Mol et al., 2015; Petrou, Eddama, & Mangham, 2011; Platt, 2014). Including these costs would have made the economic benefits of the intervention more favorable.
Our cost calculations were made from a public payer's perspective, implying that we assumed that women prepared to use calcium supplements would receive a prescription from their health care provider. Assuming that pregnant women would have to pay for calcium supplements themselves would, with equal uptake, lead to higher benefits from the perspective of the public payer. For the estimation of the expected uptake of the calcium advice, we made use of the rate of folic acid use in the periconceptional period in the Netherlands, which intervention is currently not financially reimbursed by health insurance companies. As prescription and reimbursement is expected to improve uptake rates, and higher uptake will lead to higher economic and health benefits (see Figure 2), our results probably give a conservative picture of expected effects.
4.3. Interpretation
Our results provide support for the idea that advising the use of calcium supplements to pregnant women can bring about important health effects on population level. Besides, it can reduce health care costs.
We calculated the expected impact from a high‐income perspective, using values specific for the Dutch situation. Comparable results can be expected for other high‐income countries. In low‐income countries, particularly those in which inadequate dietary calcium intake is more prevalent or baseline risk of PE is higher, health and economic effects may be more favorable (Khan, Wojdyla, Say, Gulmezoglu, & Van Look, 2006; Merialdi et al., 2005; Saleem et al., 2014). Our model can be used for the calculation of country‐specific effects by making use of local point estimates and plausible ranges.
Reaching an adequate calcium intake through calcium‐rich foods should be primarily encouraged. However, women may not be prepared to consume the daily amount of foods necessary to reach an adequate intake. For example, to take in 1,000 mg of elementary calcium by milk only, at least four glasses (200 mL each) have to be consumed. Trials of behavioral interventions to increase maternal dietary calcium intake have shown mixed results (Jung, Stork, Stapleton, Bourne, & Martin Ginis, 2014).
In view of our results, it seems efficient to advise using calcium supplements to all pregnant women. Women who are not part of defined subgroups then can also profit from the intervention, and no individual dietary calcium intake or risk of PE has to be estimated. Although the number needed to advise is higher in the overall pregnant population as compared to subgroups, this seems acceptable as calcium supplementation is a non‐invasive, well tolerated, and—provided that it is used prudently—safe intervention. Recent studies among the elderly have raised concerns that high‐dose calcium supplementation might increase the risk of cardiovascular disease (Bolland, Grey, Avenell, Gamble, & Reid, 2011; Bolland et al., 2010; Lewis et al., 2015). Available evidence remains, however, inconclusive. Moreover, most pregnant women will stop using the supplements after delivery and therefore use it for only a short period of time.
The specific dose of supplemental calcium needed to reduce the risk of PE is unknown and probably dependent on the dietary intake of calcium. Low‐dose calcium supplementation (<1 g/day) has shown a reduction in the risk of PE in some studies, but evidence is limited and more high‐quality trials are needed (Hofmeyr et al., 2014). Until more evidence is available, supplementation of 1000 mg/day is recommendable, keeping an eye on the upper level of 2,500 mg/day (EFSA NDA PANEL, 2015; Hofmeyr et al., 2014; IOM, 2011; WHO, 2013). Effects of calcium supplementation could be further enhanced if combined with vitamin D, as calcium absorption occurs principally via an active transcellular vitamin D‐dependent process (Fleet & Schoch, 2010; Heaney, 2008).
Although our results indicate that favorable economic and health effects can be obtained even with suboptimal uptake of the intervention, a challenge remains to effectively implement the intervention in health care practice (Martin, Seim, Wawire, Chapleau, & Young, 2017; Omotayo et al., 2016). Implementation efforts require that attention be paid to accessibility, affordability, acceptability, and adherence to the intervention from a patient's, care providers', and organizational point of view. Implementation strategies for low‐income countries have major challenges compared to high‐income countries, such as limited accessibility to antenatal care and economic issues (Firoz, Sanghvi, Merialdi, & von Dadelszen, 2011; Von Dadelszen et al., 2012).
Facilitators for the implementation of calcium supplementation are good tolerance, absence of adverse effects, and the expectation that it can be implemented by different health care providers with moderate levels of training and expertise (Heaney et al., 2012; Hofmeyr et al., 2014). Uncertain but important factors are the extent to which antenatal care providers are effective in changing pregnant women's behavior, and whether or not calcium supplements are covered by health insurers. Research is needed on facilitators and barriers in the implementation of calcium supplementation among pregnant women.
5. CONCLUSION
In conclusion, our results indicate that advising calcium supplements to pregnant women can be expected to cause substantial reductions in the incidence of PE as well as related health care costs. The largest impact is expected from calcium supplementation advice to all pregnant women, not subgroups only.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
LJEM, HCJS, and LJMS contributed to the conception and design of the study. LJEM and LJMS developed the computing framework. LJEM acquired existing evidence and expert opinions. All authors were involved in interpretation of outcomes. LJEM drafted the manuscript in collaboration with LJMS and HCJS. All authors contributed intellectual content, critically reviewed draft versions and approved the final manuscript.
Supporting information
Data S1. Supporting info item
Computing framework of the decision‐analytic model.
ACKNOWLEDGMENTS
We thank Huub Hoofs, Department of Epidemiology, Maastricht University, for his contribution to the creation of the tornado diagrams. Dutch Foundation “Gezond Geboren” is an independent research support fund focusing on improvement of obstetric outcomes.
Meertens LJE, Scheepers HCJ, Willemse JPMM, Spaanderman MEA, Smits LJM. Should women be advised to use calcium supplements during pregnancy? A decision analysis. Matern Child Nutr. 2018;14:e12479 10.1111/mcn.12479
REFERENCES
- Bailey, R. L. , Dodd, K. W. , Goldman, J. A. , Gahche, J. J. , Dwyer, J. T. , Moshfegh, A. J. , … Picciano, M. F. (2010). Estimation of total usual calcium and vitamin D intakes in the United States. The Journal of Nutrition, 140, 817–822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bajaj, P. S. , & Veenstra, D. L. (2013). A risk‐benefit analysis of factor V Leiden testing to improve pregnancy outcomes: A case study of the capabilities of decision modeling in genomics. Genetics in Medicine, 15, 374–381. [DOI] [PubMed] [Google Scholar]
- Bolland, M. J. , Avenell, A. , Baron, J. A. , Grey, A. , MacLennan, G. S. , Gamble, G. D. , & Reid, I. R. (2010). Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: Meta‐analysis. BMJ, 341, c3691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bolland, M. J. , Grey, A. , Avenell, A. , Gamble, G. D. , & Reid, I. R. (2011). Calcium supplements with or without vitamin D and risk of cardiovascular events: Reanalysis of the Women's Health Initiative limited access dataset and meta‐analysis. BMJ, 342, d2040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- British National Formulary . (2016). Calcium carbonate. BMJ Group and the Royal Pharmaceutical Society of Great Britain. Available at: https://www.medicinescomplete.com/mc/bnf/current/PHP93602-calcium-carbonate.htm?q=calcichew&t=search&ss=text&p=7%20-%20_hit. Accessed February 19, 2016.
- Darmstadt, G. L. , Bhutta, Z. A. , Cousens, S. , Adam, T. , Walker, N. , & de Bernis, L. (2005). Evidence‐based, cost‐effective interventions: How many newborn babies can we save? Lancet, 365, 977–988. [DOI] [PubMed] [Google Scholar]
- Duley, L. , Henderson‐Smart, D. J. , Meher, S. , & King, J. F. (2007). Antiplatelet agents for preventing pre‐eclampsia and its complications. Cochrane Database of Systematic Reviews, 18, 1–146. Cd004659. [DOI] [PubMed] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products and Allergies) . (2015). Scientific opinion on dietary reference values for calcium. EFSA Journal, 13(4101), 4182. [Google Scholar]
- Firoz, T. , Sanghvi, H. , Merialdi, M. , & von Dadelszen, P. (2011). Pre‐eclampsia in low and middle income countries. Best Practice & Research. Clinical Obstetrics & Gynaecology, 25, 537–548. [DOI] [PubMed] [Google Scholar]
- Fleet, J. C. , & Schoch, R. D. (2010). Molecular mechanisms for regulation of intestinal calcium absorption by vitamin D and other factors. Critical Reviews in Clinical Laboratory Sciences, 47, 181–195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forster, D. A. , Wills, G. , Denning, A. , & Bolger, M. (2009). The use of folic acid and other vitamins before and during pregnancy in a group of women in Melbourne, Australia. Midwifery, 25, 134–146. [DOI] [PubMed] [Google Scholar]
- Glasgow, R. E. , Lichtenstein, E. , & Marcus, A. C. (2003). Why don't we see more translation of health promotion research to practice? Rethinking the efficacy‐to‐effectiveness transition. American Journal of Public Health, 93, 1261–1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hadker, N. , Garg, S. , Costanzo, C. , Miller, J. D. , Foster, T. , van der Helm, W. , & Creeden, J. (2010). Financial impact of a novel pre‐eclampsia diagnostic test versus standard practice: a decision‐analytic modeling analysis from a UK healthcare payer perspective. Journal of Medical Economics, 13, 728–737. [DOI] [PubMed] [Google Scholar]
- Hadker, N. , Garg, S. , Costanzo, C. , van der Helm, W. , & Creeden, J. (2013). Are there financial savings associated with supplementing current diagnostic practice for preeclampsia with a novel test? Learnings from a modeling analysis from a German payer perspective. Hypertension in Pregnancy, 32, 105–119. [DOI] [PubMed] [Google Scholar]
- Heaney, R. P. (2008). Vitamin D and calcium interactions: Functional outcomes. The American Journal of Clinical Nutrition, 88, 541s–544s. [DOI] [PubMed] [Google Scholar]
- Heaney, R. P. , Kopecky, S. , Maki, K. C. , Hathcock, J. , Mackay, D. , & Wallace, T. C. (2012). A review of calcium supplements and cardiovascular disease risk. Advances in Nutrition, 3, 763–771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heppe, D. H. , Medina‐Gomez, C. , Hofman, A. , Franco, O. H. , Rivadeneira, F. , & Jaddoe, V. W. (2013). Maternal first‐trimester diet and childhood bone mass: The Generation R Study. The American Journal of Clinical Nutrition, 98, 224–232. [DOI] [PubMed] [Google Scholar]
- Hofmeyr, G. J. , Lawrie, T. A. , Atallah, A. N. , Duley, L. , & Torloni, M. R. (2014). Calcium supplementation during pregnancy for preventing hypertensive disorders and related problems. Cochrane Database of Systematic Reviews, 6, CD001059. [DOI] [PubMed] [Google Scholar]
- IOM (Institute of Medicine) . (2011). Dietary reference intakes for calcium and vitamin D. Washington, DC: The National Academies Press. [PubMed] [Google Scholar]
- Jung, M. E. , Stork, M. J. , Stapleton, J. , Bourne, J. E. , & Martin Ginis, K. A. (2014). A systematic review of behavioural interventions to increase maternal calcium intake. Maternal & Child Nutrition. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan, K. S. , Wojdyla, D. , Say, L. , Gulmezoglu, A. M. , & Van Look, P. F. (2006). WHO analysis of causes of maternal death: A systematic review. Lancet, 367, 1066–1074. [DOI] [PubMed] [Google Scholar]
- Lewis, J. R. , Radavelli‐Bagatini, S. , Rejnmark, L. , Chen, J. S. , Simpson, J. M. , Lappe, J. M. , … Prince, R. L. (2015). The effects of calcium supplementation on verified coronary heart disease hospitalization and death in postmenopausal women: A collaborative meta‐analysis of randomized controlled trials. Journal of Bone and Mineral Research, 30, 165–175. [DOI] [PubMed] [Google Scholar]
- Martin, S. L. , Seim, G. L. , Wawire, S. , Chapleau, G. M. , & Young, S. L. (2017). Translating formative research findings into a behaviour change strategy to promote antenatal calcium and iron and folic acid supplementation in western Kenya. 13. [DOI] [PMC free article] [PubMed]
- Meads, C. A. , Cnossen, J. S. , Meher, S. , Juarez‐Garcia, A. , ter Riet, G. , Duley, L. , … Khan, K. S. (2008). Methods of prediction and prevention of pre‐eclampsia: Systematic reviews of accuracy and effectiveness literature with economic modelling. Health Technology Assessment, 12, iii‐iv, 1–270. [DOI] [PubMed] [Google Scholar]
- Merialdi, M. , Mathai, M. , Ngoc, N. , Purwar, M. , Campodonico, L. , Abdel‐Aleem, H. , … Villar, J. (2005). World Health Organization systematic review of the literature and multinational nutritional survey of calcium intake during pregnancy. Fetal and Maternal Medicine Review, 16, 97–121. [Google Scholar]
- Mol, B. W. , Roberts, C. T. , Thangaratinam, S. , Magee, L. A. , de Groot, C. J. , & Hofmeyr, G. J. (2015). Pre‐eclampsia. Lancet, 387, 999–1011. [DOI] [PubMed] [Google Scholar]
- Omotayo, M. O. , Dickin, K. L. , O'Brien, K. O. , Neufeld, L. M. , De Regil, L. M. , & Stoltzfus, R. J. (2016). Calcium supplementation to prevent preeclampsia: Translating guidelines into practice in low‐income countries. Advances in Nutrition, 7, 275–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petrou, S. , & Gray, A. (2011). Economic evaluation using decision analytical modelling: Design, conduct, analysis, and reporting. BMJ, 342, d1766. [DOI] [PubMed] [Google Scholar]
- Petrou, S. , Eddama, O. , & Mangham, L. (2011). A structured review of the recent literature on the economic consequences of preterm birth. Archives of Disease in Childhood. Fetal and Neonatal Edition, 96, F225–F232. [DOI] [PubMed] [Google Scholar]
- Platt, M. J. (2014). Outcomes in preterm infants. Public Health, 128, 399–403. [DOI] [PubMed] [Google Scholar]
- Saleem, S. , McClure, E. M. , Goudar, S. S. , Patel, A. , Esamai, F. , Garces, A. , … Goldenberg, R. L. (2014). A prospective study of maternal, fetal and neonatal deaths in low‐ and middle‐income countries. Bulletin of the World Health Organization, 92, 605–612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sikkens, J. J. , van Eijsden, M. , Bonsel, G. J. , & Cornel, M. C. (2011). Validation of self‐reported folic acid use in a multiethnic population: Results of the Amsterdam born children and their development study. Public Health Nutrition, 14, 2022–2028. [DOI] [PubMed] [Google Scholar]
- Van Rossum, C. , Fransen H., Verkaik‐Kloosterman, J. , Buurma‐Rethans, E. , & Ocké, M. (2011). Dutch National Food Consumption Survey 2007–2010: Diet of children and adults aged 7 to 69 years. RIVM rapport 350050006 (Dutch).
- Von Dadelszen, P. , Firoz, T. , Donnay, F. , Gordon, R. , Hofmeyr, G. J. , Lalani, S. , … Magee, L. A. (2012). Preeclampsia in low and middle income countries‐health services lessons learned from the PRE‐EMPT (PRE‐Eclampsia‐Eclampsia Monitoring, Prevention and Treatment) project. Journal of Obstetrics and Gynaecology Canada, 34, 917–926. [DOI] [PubMed] [Google Scholar]
- Von Schmidt auf Altenstadt, J. F. , Hukkelhoven, C. W. , van Roosmalen, J. , & Bloemenkamp, K. W. (2013). Pre‐eclampsia increases the risk of postpartum haemorrhage: A nationwide cohort study in the Netherlands. PloS One, 8, e81959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO . (2013). Guideline: Calcium supplementation in pregnant women. Geneva: World Health Organization. [PubMed] [Google Scholar]
- Woude, P. A. , Walle, H. E. , & Berg, L. T. (2012). Periconceptional folic acid use: Still room to improve. Birth Defects Research. Part A, Clinical and Molecular Teratology, 94, 96–101. [DOI] [PubMed] [Google Scholar]
- Zechmeister‐Koss, I. , & Piso, B. (2014). Affordability of programmes to prevent spontaneous preterm birth in Austria: A budget impact analysis. European Journal of Public Health, 24, 145–150. [DOI] [PubMed] [Google Scholar]
- Zorginstituut Nederland . (2016). Medicijnkosten. Calciumcarbonaat. Available at: http://www.medicijnkosten.nl/. Accessed February 19, 2016.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Supporting info item
Computing framework of the decision‐analytic model.