
Figure 2.
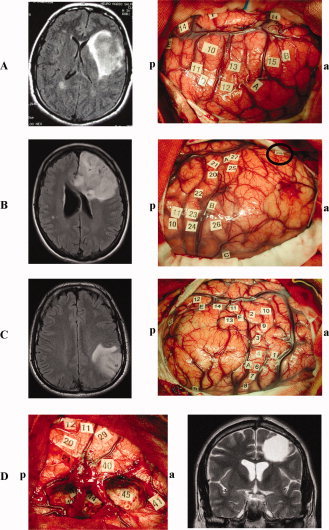
A: Patient 3, Left: Preoperative axial fluid attenuation inversion recovery (FLAIR)‐weighted MRI showing a left insular glioma. Right: Intraoperative view before resection and location of specific disturbances following electrical stimulation. The letter tags demarcate the tumor boundaries identified using intrasurgical ultrasonography. Complete speech arrest was produced with stimulation in the ventral premotor cortex (i.e., the lateral part of the precentral gyrus) (10), anomia but no gender errors with stimulation in the pars opercularis of the inferior frontal gyrus (13), and syntactic gender error but no naming disturbances with stimulation in the pars opercularis of the inferior frontal gyrus (12). The other letter tags correspond to sensory‐motor sites or areas generating transient hesitation when stimulated during naming task without speech arrest, anomia or syntactic gender disorders. a = anterior; p = posterior. B: Patient 6, Left: Preoperative axial FLAIR‐weighted MRI showing a left frontal glioma. Right: Intraoperative view before resection and location of specific disturbances following electrical stimulation. The letter tags demarcate the tumor boundaries identified using intrasurgical ultrasonography. Complete speech arrest was produced with stimulation in the ventral premotor cortex (20/21), anomia but no gender errors with stimulation in the pars opercularis of the inferior frontal gyrus (27/25) as well as in the dorsolateral prefrontal cortex (i.e. posterior part of the middle frontal gyrus) (26), and syntactic gender error but no naming disturbances with stimulation in the pars orbitaris of the inferior frontal gyrus (28). The other letter tags correspond to sensory‐motor sites or areas generating transient hesitation when stimulated during naming task without speech arrest, anomia or syntactic gender disorders. a = anterior; p = posterior. C: Patient 9, Left: Preoperative axial FLAIR‐weighted MRI showing a left parietal glioma. Right: Intraoperative view before resection and location of specific disturbances following electrical stimulation. The letter tags demarcate the tumor boundaries identified using intrasurgical ultrasonography. Complete speech arrest was produced with stimulation in the ventral premotor cortex (1), anomia but no gender errors with stimulation in the posterior part of the superior temporal gyrus (14), and syntactic gender errors but no naming disturbances with stimulation in the posterior part of the middle temporal gyrus (12). The other letter tags correspond to sensory‐motor sites or areas generating transient hesitation when stimulated during naming task without speech arrest, anomia or syntactic gender disorders. a = anterior; p = posterior. D: Patient 4, Left: Intraoperative view after resection of a left frontal glioma and location of specific disturbances following electrical stimulation at both cortical and subcortical levels. Complete speech arrest was produced with stimulation in the ventral premotor cortex (11/12), anomia but no gender errors with stimulation in the pars opercularis of the inferior frontal gyrus (29), and syntactic gender error but no naming disturbances with stimulation in the pars triangularis of the inferior frontal gyrus (40). Interestingly, subcortical stimulation of the white matter around the head of the caudate nucleus, below the cortical site 40, also elicited reproducible syntactic gender error without naming disorders (anomia was specifically generated in 45). The other letter tags correspond to sensory‐motor sites or areas generating transient hesitation when stimulated during naming task without speech arrest, anomia or syntactic gender disorders. a = anterior; p = posterior. Right: Postoperative coronal T2‐weighted MRI confirming that the surgical cavity was into the contact of white matter around the head of the caudate nucleus, in particular with pathways coming for the inferior frontal gyrus. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]