
Fig. 2. Histopathological analysis of human breast cancer samples correlates IL-8 enrichment with the presence of mammographic calcifications and proliferative ductal epithelia.
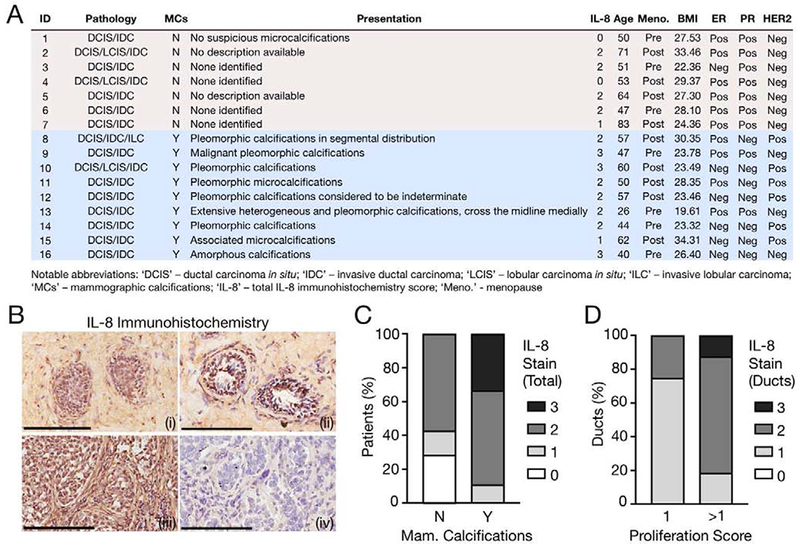
(A) Patient information for assessed specimens, sorted by presence of mammographic calcifications. ‘IL-8’ indicates the corresponding degree of total IL-8 stain via immunohistochemistry (IHC). This chart represents an expanded version of a previously published dataset [5]. (B) Representative IL-8 IHC with hematoxylin counterstain. Image labels: (i) - Weak ductal; (ii) - Strong ductal; (iii) - Strong ductal and stromal; (iv) – No IgG. Scale bars, 200 μm. (C) Histopathological scoring for the degree of total IL-8 stain as a function of mammographic calcifications. Rubric for total IL-8 staining intensity: 0-to-3, with 0 representing negligible intensity and 3 representing maximum staining. N vs. Y: p<0.05. (D) Histopathological scoring for the degree of ductal IL-8 stain as a function of the ductal proliferation score. Rubric for ductal IL-8 staining intensity: 0-to-3, with 0 representing negligible intensity and 3 representing maximum staining. Rubric for ductal proliferation: 0-to-3, with 0 representing negligible proliferation and 3 representing excessive proliferation and total deterioration of acinar architecture. 1 vs. >1: p<0.05.