

Abstract
Children who have difficulty using reparative behaviors following transgressions display a wide range of poorer social and emotional outcomes. Despite the importance of reparative skills, no study has charted the developmental trajectory of these behaviors or pinpointed predictors of poorer reparative abilities. To address these gaps in the literature, this study applied growth mixture modeling to parent-reports of children’s reparative behaviors (N = 230) in a 9-year longitudinal dataset spanning from preschool to early adolescence. Three distinct trajectories of reparative behaviors were found: a low-stable, moderate-stable, and high-stable latent class. Poorer emotion understanding, social withdrawal, social rejection, and maladaptive guilt in the preschool period predicted membership in a low-stable reparative trajectory. Externalizing diagnoses, particularly Conduct Disorder and Oppositional Defiant Disorder, also predicted membership in a low-stable reparative trajectory. Preschool-onset depression (PO-MDD) predicted membership in a low-stable reparative trajectory through high levels of maladaptive guilt. The findings from this study suggest that socioemotional deficits in the preschool period set children on longstanding trajectories of impaired reparative responding. Thus, emotion understanding, social functioning, maladaptive guilt, and early psychiatric symptoms should be targeted in early preventive interventions.
Keywords: Reparative behaviors, growth mixture modeling, emotion understanding, social functioning, preschool depression
Learning to amend transgressions using prosocial behaviors is an important developmental skill for young children to master. Reparative behaviors—or prosocial behaviors that transgressors direct toward victims of their wrongdoings (Tangney, Stuewig, & Mashek, 2007)— have been positively associated with social acceptance and positive affect and negatively associated with externalizing and internalizing problems across children, adolescents, and adults (Bafunno & Camodeca, 2013; Caprara, Barbaranelli, Pastorelli, Cermak, & Rosza, 2001; Cohen, Wolf, Panter, & Insko, 2011; Howell, Dopko, Turowski, & Buro, 2011; Kochanska, Koenig, Barry, Kim, & Yoon, 2010; Luyten, Fontaine, & Corveleyn, 2002). Despite the importance of reparative behaviors to children’s social and emotional outcomes, no study has charted their developmental course, and very few studies have identified predictors of reparative abilities. Preschoolers’ emotion understanding, social functioning, and psychiatric diagnoses have been previously associated with their general prosocial skills and may similarly predict reparative behaviors (Eggum et al., 2011; Luby, Belden, Sullivan, et al., 2009; O’Toole, Monks, & Tsermentseli, 2017). The purpose of this study was to examine developmental trajectories of reparative behaviors from preschool through early adolescence and identify predictors of these longitudinal trajectories.
Reparative Behaviors
Prosocial behaviors are voluntary actions that are helpful, affiliative, supportive and aimed at benefitting another person (Eisenberg & Fabes, 1998). Theorists have recently argued that prosocial actions can be categorized into three distinct subtypes—helping, (i.e., assisting another in achieving an instrumental goal), sharing (i.e., giving up a limited resource), and comforting behaviors (i.e., offering physical or verbal support; Dunfield, 2014; Svetlova, Nichols, & Brownell, 2010). Research is increasingly highlighting the complex and multidimensional nature of prosocial behaviors; for example, empirical studies have found that these three subtypes emerge at different points in development (Svetlova et al., 2010), and are fostered through different parental socialization practices (Pettygrove, Hammond, Karahuta, Waugh, & Brownell, 2013).
Prosocial behaviors can also be classified based on the context in which they occur. Children use prosocial behaviors in response to both distress that they have witnessed as bystanders as well as to distress they have caused as transgressors. Prosocial responses to distress witnessed as a bystander (hereafter referred to as general prosocial behaviors) function to promote or sustain relationships, whereas responses to distress caused as a transgressor are termed reparative behaviors, as they function to repair or restore relationships (Estrada-Hollenbeck & Heatherton, 1998). Thus, reparative behaviors are a specific type of prosocial behavior that include helping, sharing, and comforting behaviors as well as attempts to make amends (e.g., fix a broken item), apologize, and confess to a transgression (Tangney et al., 2007).
Reparative behaviors are related to, yet distinct from, general prosocial behaviors. Whereas empathy underlies general prosocial behaviors, reparative behaviors are motivated by guilt, in which a child experiences empathy for a victim and an awareness of personal responsibility for causing the victim’s distress (Tilghman-Osborne, Cole, & Felton, 2010). Several studies have demonstrated that toddlers and preschoolers are less prosocial as transgressors than bystanders (Dunn & Brown, 1994; Dunn, Brown, Slomkowski, Tesla, & Youngblade, 1991; Zahn-Waxler, Radkerrow, Wagner, & Chapman, 1992; Zahn-Waxler, Radke-Yarrow, & King, 1979), suggesting that it may be more difficult for young children to engage in reparative than general prosocial behaviors. Studies have also documented that children are less empathic and more likely to display avoidance, self-distress, aggression, and positive affect as transgressors than bystanders, further highlighting the distinctiveness and more emotionally challenging nature of the transgressor context to young children (Barrett, Zahn-Waxler, & Cole, 1993; Demetriou & Hay, 2004; Zahn-Waxler et al., 1992).
Reparative behaviors serve an important function in helping transgressors alleviate potentially excessive and harmful guilty feelings. Guilt often motivates reparative behaviors to make amends for the transgression (e.g., Colasante, Zuffianò, Bae, & Malti, 2014). In turn, the use of reparative behaviors following a transgression effectively alleviates guilt (de Hooge, 2012). Theorists posit that the inability to engage in reparative behaviors plays an important role in the development and maintenance of psychopathology, particularly depression (Quiles & Bybee, 1997). When individuals cannot or do not use reparative behaviors to alleviate guilty feelings, maladaptive guilt, a destructive type of guilt that is intense, extreme, or inaccurate (Tilghman-Osborne, Cole, & Felton, 2012) is theorized to develop. In a vicious cycle, maladaptive guilt further inhibits reparative behaviors, leading to chronically unalleviated guilt, and, over time, depression (Quiles & Bybee, 1997). Indeed, maladaptive guilt has been linked to higher levels of depression in children and adults (Jones & Kugler, 1993; Luby, Belden, Sullivan, et al., 2009).
Despite evidence documenting the importance of learning to engage in reparative behaviors for children’s positive social and emotional outcomes (e.g., Luby et al., 2009) there is a dearth of literature documenting the developmental course and predictors of reparative functioning. As early as the first year of life, children begin to engage in reparative behaviors after transgressions (e.g., Kochanska, Gross, Lin, & Nichols, 2002). For example, in a naturalistic study by Zahn-Waxler et. al (1979), children as young as 15 months engaged in reparative behaviors after transgressing. Throughout early childhood, children’s capacity for reparative behaviors continues to develop alongside associated cognitive skills such as self-awareness, understanding of social norms, and theory of mind (Lewis, 2008; Muris & Meesters, 2014). As no study has charted trajectories of reparative behaviors, very little is known about how children’s reparative abilities change over the course of development. In toddlerhood, reparative behaviors have been found to include verbalizations (e.g., “all better now?”), simple apologies (“sorry”), making amends (e.g., offering food, a bandaid, or toys), and giving physical affection (e.g., hugging the victim; Kochanska et al., 2002; Zahn-Waxler et al., 1979). In older children, reparative behaviors also include more sophisticated verbalizations (e.g., apologies that include elaborations of remorse or responsibility; Ely & Gleason, 2006) and actions (e.g., attempts to fix or replace broken items; Kochanska, DeVet, Murray, & Putnam, 1994). One study found that reparative behaviors were more frequent with older age across 4-to 8-year-olds (Colasante et al., 2014); however, the association between age and reparative behaviors may be more complex, as children’s prosocial behaviors tend to become more selective over development as they learn more about situations in which they are needed (Hay & Cook, 2007).
The few existing studies of concurrent predictors of reparative responding have found that parenting styles that deemphasize power assertion and include inductive reasoning were associated with greater levels of reparative behaviors (Kochanska, 1991; Zahn-Waxler et al., 1979). To date, no study has examined child socioemotional factors that may influence reparative abilities, such as children’s emotion understanding abilities, social functioning, and psychiatric diagnoses.
Developmental trajectories of general prosocial behaviors
Several studies have examined general prosocial behaviors in childhood and adolescence using a developmental trajectory approach. The majority of these studies have found evidence for three latent classes that reflect low, moderate, and high levels of general prosocial behavior across development (Cote, Tremblay, Nagin, Zoccolillo, & Vitaro, 2002; Flynn, Ehrenreich, Beron, & Underwood, 2015; Nantel-Vivier, Pihl, Côté, & Tremblay, 2014), although a smaller number of studies have found evidence of four or five classes (Nantel-Vivier et al., 2009; Padilla-Walker, Dyer, Yorgason, Fraser, & Coyne, 2015). Interestingly, despite a meta-analytic finding of increased prosociality across development (Eisenberg & Fabes, 1998), the majority of studies have identified trajectories that are either stable or declining over time. For example, in one study of 472 Italian youth aged 10-to 14-years old, only 7% of the sample was classified into a latent class characterized by increasing, rather than stable or declining, prosocial behaviors (Nantel-Vivier et al., 2014). A decline in prosociality appears to occur around pre-adolescence (Cote et al., 2002; Nantel-Vivier et al., 2014) with some evidence of a slight rebound once children reach 12th grade (Carlo, Crockett, Randall, & Roesch, 2007). Whether reparative prosocial behaviors can also be classified into at least three, stable or declining trajectories from preschool through early adolescence remains unexplored. Charting reparative behavior trajectories may further illuminate the similarities and differences of these behaviors to general prosocial skills.
Several predictors of membership in general prosocial trajectories have been identified. Gender has emerged as a robust predictor, with several studies finding that boys are significantly more likely to be members of low-stable than moderate-stable or high-stable prosocial trajectories (Cote et al., 2002; Flynn et al., 2015; Nantel-Vivier et al., 2009, 2014). Other research has identified family and/or environmental predictors of general prosocial trajectories, with studies generally finding links between negative parenting practices and membership in low-stable prosocial trajectories. For example, one study found that children who reported lower maternal warmth were more likely to be members of a low-stable than moderate-stable or high-increasing trajectories of prosocial behaviors toward family (Padilla-Walker et al., 2015). Similarly, children from families characterized by less positive parenting were less likely to be members of a high-stable than a moderate-stable or low-stable prosocial trajectory (Nantel-Vivier et al., 2014). Nantel-Vivier and colleagues (2014) found that maternal depression and lower socioeconomic status (SES) increased children’s likelihood of membership in a high-stable prosocial trajectory. This finding may seem counter-intuitive and conflicts with other literature demonstrating lower levels of prosocial behavior among lower SES children (Lichter, Shanahan, & Gardner, 2002) and children of depressed mothers (Hay & Pawlby, 2003). One explanation may be that these children are under more social pressure to display precocious prosocial behavior given the absence of parental and social support. Alternatively, there may also be more complex, quadratic relationship between stressful family environments and prosocial behavior such that children from these family environments exhibit both very low and very high levels of prosocial behavior. Tendencies toward high prosocial behaviors in children of low SES or children of depressed mothers may be a reaction to periods of harsh parenting related to these factors (e.g., Rakow et al., 2009).
Very few studies have examined child factors that influence general prosocial trajectories. One study found that adolescents’ low sympathy and low self-regulation predicted greater odds of membership in a low-stable than a high-stable trajectory of general prosocial behaviors toward family (Padilla-Walker et al., 2015). Studies have also demonstrated that children’s externalizing and internalizing problems are related to membership in low-stable general prosocial trajectories (Flynn et al., 2015; Nantel-Vivier et al., 2014). For example, in the study by Nantel-Vivier and colleagues (2014), a large proportion of highly aggressive 2-to 11-year-old children were members of the low-stable prosocial trajectory, and membership in the low-stable prosocial trajectory was also associated with both high and low depression. Although this finding suggests associations between early childhood externalizing and depressive symptoms and membership in low prosocial trajectories, it was limited by the use of parent report rating scales that assessed externalizing and depressive symptoms broadly rather than structured diagnostic interviews that utilize clinician interviewers to determine age-appropriate symptoms of psychiatric disorders.
Several aspects of deficits in children’s social and emotional competence are theoretically and empirically related to children’s concurrent prosocial and reparative difficulty and may thus predict low trajectories of reparative behaviors. First, children’s abilities to behave prosocially theoretically depend on both their capabilities to identify a victim’s emotional distress as well as social opportunity and exposure that provide children an important context in which to learn and practice prosocial skills (Denham, 2006; Rubin & Coplan, 2004). As follows, children’s emotion understanding deficits, social withdrawal, and social rejection may likely predict low reparative trajectories. Second, both externalizing and internalizing psychopathology are associated with reparative difficulty (e.g., Cohen et al., 2011; Luyten et al., 2002), which can theoretically be explained through very low and high levels of guilt, respectively. Indeed, as moderate levels of guilt motivate reparative behavior (e.g., Cryder, Springer, & Morewedge, 2012), the very low levels of guilt characteristic of externalizing disorders (Muris et al., 2016) are likely insufficient to motivate reparative behaviors, whereas the excessively high levels of guilt characteristic of depression (i.e., maladaptive guilt) theoretically inhibit reparative behaviors (Quiles & Bybee, 1997). Thus, maladaptive guilt and preschool-onset psychopathology may also predict reparative trajectories. We now review empirical evidence of associations between levels of general prosocial or reparative behaviors and these aspects of children’s social and emotional competence that have implications for examining trajectories of reparative behaviors.
Influence of emotion understanding on prosocial behaviors
A wealth of literature demonstrates that children’s empathy predicts their general prosocial behaviors (for review see: Eisenberg, Eggum, & Di Giunta, 2010). An important building block of both affective empathy, or experiencing the same emotion that another is feeling, as well as cognitive empathy, or the capacity to take another’s perspective, is the ability to identify and understand emotions, or emotion understanding. Emotion understanding is a term that encompasses children’s developing abilities to recognize facial expressions, label and understand causes of emotions (Saarni, Campos, Camras, & Witherington, 2006). Basic emotion understanding skills emerge by age three, when children are able to verbally identify positive and negative emotions (Widen & Russell, 2003), and can receptively point to the correct facial expression when verbally presented with an emotion term (Albanese et al., 2006). Although emotion understanding improves with age across childhood (Pons, Harris, & de Rosnay, 2004), marked individual differences in children’s emotion understanding skills are present as early as the preschool period (Dunn et al., 1991).
Individual differences in preschoolers’ emotion understanding are predictive of their levels of general prosocial behaviors. Across correlational studies, 2-to 6-year-old children’s poorer emotion understanding has been associated with their poorer prosocial skills (Belacchi & Farina, 2010; Denham, 1986; Denham & Couchoud, 1991; Diesendruck & Ben-Eliyahu, 2006; Ensor & Hughes, 2005; Ornaghi, Pepe, & Grazzani, 2016). To assess emotion understanding in preschoolers, studies typically use tasks in which children listen to vignettes read from storybooks or enacted by puppets and are asked to point to the pictoral facial expression that describes how the protagonist or puppet would feel (Denham, 1986). Studies have also demonstrated that preschool emotion understanding longitudinally impacts children’s later prosocial abilities. Children’s emotion understanding difficulties at age three have been found to predict their poorer prosocial skills at age four (Eggum et al., 2011; Ensor, Spencer, & Hughes, 2011). Moreover, poorer emotion understanding at age 3-to 4 has been found to predict lower teacher-rated prosocial behaviors at age 5-to 6 (Denham et al., 2003).
In sum, several studies support that children’s poorer emotion understanding skills are associated with decreased concurrent and future general prosocial behavior. Although children’s successful use of reparative behaviors likely depends, in part, on their abilities to first identify that someone they have harmed is in distress (Denham, 2006), studies have not yet investigated emotion understanding as a predictor of reparative behaviors or trajectories.
Influence of social rejection and withdrawal
Peer rejection and social withdrawal in the preschool period may also predict children’s membership in a low reparative behavior trajectory, as socially rejected or withdrawn children likely have limited opportunities to learn and practice reparative skills through peer interactions. Studies across middle childhood and adolescence have found that children’s greater peer rejection is associated with their lesser general prosocial responding (Di Giunta et al., 2018; LaFontana & Cillessen, 2002; Peters, Cillessen, Riksen-Walraven, & Haselager, 2010). One study found that greater teacher-reported peer rejection was related to lower levels of general prosocial behavior in children as young as 3-to 6-years-old (O’Toole et al., 2017). There are likely bidirectional effects between peer rejection and prosocial deficits; indeed, whereas studies have found that peer rejection increases the probability of subsequent decreases in general prosocial behavior (Obsuth, Eisner, Malti, & Ribeaud, 2015), another study found that children’s lesser general prosocial behavior at age 8 predicted their greater peer rejection at age 13–14 (Caprara, Barbaranelli, Pastorelli, Bandura, & Zimbardo, 2000).
Social withdrawal is a term describing children who prefer to play alone when in the company of peers; this withdrawal may reflect a low social approach motivation (“social disinterest”) or a high social avoidance motivation (“anxious solitude”; Rubin & Coplan, 2004). Although fewer studies have examined relations between social withdrawal and general prosocial behavior, existing studies have demonstrated that social withdrawal is associated lower levels of general prosocial behaviors in early childhood (Ladd & Profilet, 1996) and early adolescence (Findley & Ojanen, 2013).
Influence of preschool-onset psychiatric diagnoses
Children’s psychiatric diagnoses have been previously associated with children’s concurrent levels of reparative behaviors and may thus predict trajectories of reparative behaviors. A previous report from the sample examined in the current study found that children with both PO-MDD and preschool-onset externalizing diagnoses—Attention-Deficit/Hyperactivity Disorder (ADHD), Oppositional Defiant Disorder (ODD), or Conduct Disorder (CD)—displayed significantly lower levels of concurrent reparative behaviors than their peers with anxiety diagnoses or no psychiatric diagnosis (Luby, Belden, Sullivan, et al., 2009). Moreover, children with PO-MDD had significantly higher levels of guilt than other children, suggesting that PO-MDD may be associated with reparative deficits through excessive (i.e., maladaptive) guilt. Indeed, maladaptive guilt has been associated with low levels of reparative behaviors in adults, likely due to overwhelmingly intense affect that impedes reparation and/or thoughts that transgressions are not reparable (e.g., Nencini & Meneghini, 2013). Whether preschool-onset psychiatric diagnoses predict trajectories of reparative behaviors or whether reparative difficulties in these children represent developmentally transient phenomenon remains unexplored. Further, no study has directly tested whether PO-MDD is related to reparative deficits through maladaptive guilt.
Overview of the Proposed Study and Hypotheses
In summary, reparative behaviors have been associated with a wide range of social and emotional outcomes (e.g., Luby, Belden, Sullivan, et al., 2009) and theoretically alleviate guilt, preventing maladaptive guilt and psychopathology, particularly depression (Quiles & Bybee, 1997). Despite the critical importance of these behaviors for young children’s development, no study to date has charted their developmental course, and very few examinations have identified predictors of reparative difficulty. Identifying modifiable social and emotional markers of risk for reparative deficits in early childhood, when these abilities are developing, may inform interventions to increase reparative responding and protect children from poorer outcomes.
The aims of the current study were threefold. First, we aimed to address gaps in the literature by charting the developmental trajectory of reparative behaviors endorsed by caregivers in a 9-year longitudinal dataset spanning from preschool into adolescence. Second, after creating these trajectories, we sought to examine the predictive power of child factors measured early in development during the preschool period, specifically emotion understanding, social functioning, maladaptive guilt, and psychiatric disorders, on trajectory class membership. Finally, we also aimed to directly test the hypothesis that PO-MDD would be related to membership in a low reparative trajectory through high levels of maladaptive guilt.
We hypothesized the following:
As reparative behaviors are related yet distinct from general prosocial behaviors, we did not predict a specific number of trajectories.
We anticipated that boys would be more likely to be members of lower, rather than higher, trajectories.
We also expected that children with poorer emotion understanding, greater social withdrawal, greater peer rejection, and greater maladaptive guilt would be more likely to be members of lower than higher trajectories.
We expected that groups of children with a preschool-onset externalizing diagnosis (ADHD, ODD, or CD) and PO-MDD would both be more likely to be members of lower trajectories.
Finally, we also hypothesized that the association between PO-MDD and membership in a low reparative trajectory would be explained by high levels of maladaptive guilt.
Methods
Participants
Participants were 306 children from the Preschool Depression Study (PDS), a prospective longitudinal investigation of preschoolers conducted at [name of university redacted for peer review] (Luby, Si, Belden, Tandon, & Spitznagel, 2009). Child assent and parental written consent were obtained prior to study participation and the Institutional Review Board at [university] approved all procedures. Recruitment details have been previously described (Luby, Si, et al., 2009). In sum, at the baseline assessment, 3-to 6-year-olds were recruited from preschools, daycares and primary care practices throughout a medium sized Midwestern metropolitan area using a validated screening questionnaire (Preschool Feelings Checklist; Luby, Heffelfinger, Koenig-McNaught, Brown, & Spitznagel, 2004) to oversample preschoolers with depressive symptoms as well as healthy controls. The current investigation examines data at four timepoints: when children were 3-to 6-years-old (T1), 4-to 7-years-old (T2), 5-to 8-years-old (T3), and 8-to 13.5-years-old (T4). To be included in the quadratic growth mixture models (see data analytic plan), participants needed to have completed at least three of four annual assessments. Seventy-six participants completed fewer than three assessments and were thus excluded from analyses, yielding a final sample of N = 230 participants. Parents reported children’s race as follows: 59.1% White, 27.0% Black, 12.6% Biracial, 0.9% Asian, and 0.4% American Indian. Parents reported children’s ethnicity as 99.1% Non-Hispanic/Latinx and 0.9% Hispanic/Latinx.
Maladaptive guilt and reparative behaviors.
Both maladaptive guilt and reparative behaviors were assessed using the My-Child-2 (Kochanska et al., 1994), a 100-item parent-report questionnaire that measures children’s emotions and behaviors after transgressions or wrongdoing. This scale is composed of two main factors—guilt feelings and guilt reparations (hereafter referred to as maladaptive guilt and reparative behaviors; Kochanska et al., 1994). The maladaptive guilt scale assesses guilt in preschoolers that is ongoing or excessive and has been found to function maladaptively (Luby, Belden, Sullivan, et al., 2009). Subscales include: 1) Guilt after wrongdoing; 2) Symbolic reproduction of wrongdoing; 3) Concern over good feelings with parent after wrongdoing; and 4) Sensitivity to flawed or damaged objects and themes of wrongdoing. Examples of items include, “may have problems sleeping or a poor appetite after having done something wrong” and “after a wrongdoing, child replays that situation with toys.” The reparative behaviors scale assesses children’s use of reparative behaviors after transgressing. Subscales include: 1) Amends; 2) Internalized conduct; 3) Confession; 4) Prosocial response; 5) Concern occasioned by others’ transgressions; and 6) Apology. Examples of items are: “likely to spontaneously say ‘sorry’ after having done something wrong” and “tries to make up for a wrongdoing.” Parents rated each item on a 1–7 Likert-type scale; thus, higher scores indicate greater reparative behaviors.
The current study examines reparative behaviors assessed at T1-T4 and maladaptive guilt assessed at T1. At T3 and T4, a slightly modified version of the My-Child-2 questionnaire was administered in which minor wording alterations were made to 17% of items to better address developmental issues as the population aged. For example, the item “eager to make amends for doing something naughty” read “eager to make amends for doing something disobedient” at T3 and T4. Internal consistency reliability of the My-Child-2 ranged from α=.86 at T1 to α=.95 at T10 (Mα=.88). Finally, as affective and behavioral responses to transgressions are often correlated, creating residual scores is often recommended to obtain purer measures of affect versus behavior (e.g., (Luyten et al., 2002). Thus, we regressed the maladaptive guilt scale on the reparative behaviors scale to obtain maladaptive guilt residual scores. We also regressed the reparative behaviors scale on the maladaptive guilt scale to obtain reparative behavior residual scores. Residual, rather than raw scores, were used in analyses of study hypotheses.
Emotion identification.
Emotion identification was assessed at T1 using the Penn Emotion Differentiation Task (EMODIFF; Gur et al., 2010) is a 24-item, validated measure of children’s abilities to recognize emotional facial expressions that participants completed using a standardized computer program. Children are shown 24 pairs of adult faces, presented one pair at a time, and are required to select the more intense facial expression of the pair. The number of correct responses were summed to yield a total score; thus, higher scores indicate greater emotion identification skills. Internal consistency reliability was α=.73.
Social functioning.
Two variables reflecting children’s social functioning were assessed at T1 using the MacArthur Health and Behavior Questionnaire, Parent Form, Version 2.1 (Armstrong & Goldstein, 2003), a parent-report measure of children’s social, emotional, and physical functioning. The social withdrawal subscale includes 9-items assessing children’s asociality, or the extent to which children prefer to spend time alone compared to with peers, and social inhibition. Example items include, “prefers to play alone,” and “shy with other children.” Higher scores indicate greater social withdrawal. The peer acceptance/rejection subscale includes 8-items that assess the extent to which children are accepted or rejected by peers. An example item is, “is often left out by other children.” Lower scores indicate lesser peer acceptance and greater peer rejection. Internal consistency reliability was α=.80 for social withdrawal and α=.85 for peer rejection.
Preschool-onset psychiatric diagnoses.
Parents were interviewed using the Preschool Age Psychiatric Assessment (PAPA; Egger, Ascher, & Angold, 2003), which consists of a series of developmentally appropriate questions to assess DSM criteria for psychiatric disorders. Diagnoses of PO-MDD, ADHD, ODD, CD, Separation Anxiety Disorder (SAD), Generalized Anxiety Disorder (GAD), and Post-Traumatic Stress Disorder (PTSD) were assessed at T1 and covered the preceding 6 months. The existence of MDD in the preschool period has been extensively validated (e.g., Luby et al., 2002). The current study examines the presence or absence of PO-MDD, any externalizing disorder, and any anxiety disorder. Children were considered to have an externalizing disorder if they met criteria for ADHD, ODD, or CD. Children were considered to have an anxiety disorder if they met criteria for SAD, GAD, or PTSD. Children were given a dichotomous score for each disorder (e.g., ‘1’ externalizing disorder present; ‘0’ externalizing disorder not present). Inter-rater reliability of the PAPA in our sample has been previously reported (e.g., Whalen, Belden, Tillman, Barch, & Luby, 2016)
Income-to-needs ratio
Families’ income-to-needs ratios at T1, or the total family income divided by the federal poverty level based on family size, were calculated (McLoyd, 1998). An income-to-needs ratio of 1 indicates that the family was living at the poverty threshold. This measure of families’ early financial advantage/disadvantage was used as a covariate in analyses of study hypotheses.
Data analytic plan
The current study used a developmental trajectory approach to examine the longitudinal course of reparative behaviors. Developmental trajectory approaches such as latent class growth analysis (LCGA; Nagin, 1999) or growth mixture modeling (GMM; Muthén & Muthén, 2000) enable the creation of unique trajectories of reparative behaviors for groups of children whose behavioral patterns are similar across time. These approaches also enable the identification of risk and resilience factors that increase the likelihood of children’s membership in a low or high developmental trajectory of reparative behaviors.
Beginning at T1, participants were classified into subgroups based on reparative behavior scores across the longitudinal study using GMM in Mplus version 8.1 (Muthén & Muthén, 2000). Mplus utilizes full information maximum likelihood (FIML) estimation under the assumption of data missing at random (MAR) with robust standard errors (called the MLR estimator in Mplus). Specifically, reparative behavior scores were calculated at each of the four annual assessment waves. The majority of participants had data from all four timepoints (n = 156); a minority had data from three timepoints (n = 74). Quadratic growth mixture models with these scores as the dependent variables were used to determine categorical latent class variables for grouping participants with similar reparative behavior trajectories. In each of these models, participants’ probability of belonging to each of the latent classes was evaluated, and participants were assigned to the latent class with the greatest probability. Several growth mixture models with varying numbers of classes (1–5 classes) for reparative behaviors were compared. The model with the best fit according to a combination of the Bayesian Information Criterion (BIC), the Lo-Mendell-Rubin adjusted likelihood ratio test (LRT), and sample size of the resulting classes was selected (Jung & Wickrama, 2008; Nylund, Asparouhov, & Muthén, 2007).
We then used multinomial logistic regressions to determine whether emotion identification skills, social functioning, maladaptive guilt feelings, and preschool-onset psychiatric diagnoses predicted latent class membership. These analyses compare latent classes (i.e., low vs. moderate, moderate vs. high, low vs. high) on the predictors of interest. Children’s sex, and T1 income-to-needs ratio were included as covariates in each analysis. Importantly, children’s age at T1 was also included as a covariate in each analysis to account for the fact that participants ranged in age at each timepoint. Given that the current sample was enriched for depression, whether or not children met criteria for PO-MDD at T1 was also included as a covariate in each analysis.
In order to test our specific hypothesis about the role of guilt and reparation in depression and to determine whether maladaptive guilt partially explained relations between PO-MDD and latent class membership, mediation analyses were conducted using the PROCESS macro for SAS (Hayes, 2012; Hayes & Preacher, 2014). Whether or not children met criteria for an externalizing diagnosis at T1 was included as an additional covariate in this analysis. When warranted, the Monte Carlo simulator was used to test the statistical significance of the indirect, or mediating, effect. The Monte Carlo method is a form of bootstrapping, which simulates random draws from the distributions of each path in the model to estimate a 95% confidence interval around the indirect effect. Bootstrapping is generally preferred over more traditional methods of calculating mediation.
Results
Preliminary Analyses
Descriptive statistics for participants are presented in Table 1. Relevant demographic characteristics (sex, age at T1, T1 income-to-needs ratio) were not significantly different between the latent classes.
Table 1.
Descriptive Statistics of Study Participants
| Observed Range | Mean (SD) or Frequency | ||||
|---|---|---|---|---|---|
| Variable | Overall Sample | Low Reparative Behaviors | Moderate Reparative Behaviors | High Reparative Behaviors | |
| N=230 | n=47 | n=133 | n=50 | ||
| 1. T1 Age (months) | 36–71 | 53.10 (9.51) | 55.00 (9.57) | 51.90 (9.47) | 54.50 (9.26) |
| 2. Sex (% female) | 47.4% | 48.9% | 43.6% | 56.0% | |
| 3. T1 Income to needs | 0–3.93 | 2.19 (1.14) | 2.11 (1.20) | 2.17 (1.14) | 2.33 (1.11) |
| 4. T1 EMODIFF scores1 | 0–23 | 1.47 (4.50) | 10.03 (4.07) | 12.02 (4.36) | 11.30 (5.05) |
| 5. T1 Maladaptive guilt2 | −8.08–6.86 | −.12 (2.38) | .94 (1.99) | −.14 (2.36) | −1.09 (2.40) |
| 6. T1 MDD (% present) | 24.5% | 42.6% | 22.6% | 12.2% | |
| 7. T1 Anxiety (% present) | 21.0% | 25.5% | 18.8% | 22.4% | |
| 8. T1 Externalizing (% present) | 32.3% | 57.4% | 32.3% | 8.2% | |
Note.
EMODIFF = Penn Emotion Differentiation Task
Maladaptive guilt residual scores were used.
We have previously replicated Kochanska’s original two-factor structure of the My-Child-2 questionnaire in our sample at T1 (Luby, Belden, Sullivan, et al., 2009). As a small number of items were slightly modified for T3 and T4, we used the procedure outlined by Kochanska et. al (1994) to conduct separate principal components analyses (PCA) at T2, T3, and T4 to ensure that the questionnaire had a similar factor structure across all timepoints. For these analyses, raw scores rather than residuals were used. Strong evidence of a two-factor solution (rotated using the varimax rotation) was found at each timepoint. No factor other than reparation behaviors and maladaptive guilt had an eigenvalue above one at any timepoint. The same subscales loaded onto the reparative behaviors and maladaptive guilt factors, respectively, across all timepoints. Table 1 presents factor loadings for each subscale as well as variance and eigenvalues for each factor at each of the four timepoints.
Growth Mixture Model
Fit statistics for the growth mixture models with latent class variables with 1, 2, 3, 4, and 5 classes were compared (Table 3). The 3-class model had the lowest BIC and fit significantly better than the 2-class model according to the Lo-Mendell-Rubin adjusted LRT, so the 3-class model was chosen for analyses. Because the slope and quadratic terms in the 3-class model were non-significant, they were removed from the model. The probabilities of being included in each latent class were: low 0.87 (0.17), moderate 0.89 (0.14), and high 0.93 (0.11).
Table 3.
Fit statistics of growth mixture models of reparation behaviors
| N Latent Classes | AIC | BIC | Log- Likelihood | Entropy | L-M-R ALRT p | Latent Class N’s |
|---|---|---|---|---|---|---|
| 1 | 4760.732 | 4784.799 | −2373.366 | 1.000 | -- | 230 |
| 2 | 4552.490 | 4590.309 | −2265.245 | 0.722 | 0.0038 | 134, 96 |
| 3 | 4476.051 | 4527.622 | −2223.026 | 0.779 | 0.0058 | 43, 135, 52 |
| 4 | 4467.800 | 4533.124 | −2214.900 | 0.690 | 0.4149 | 27, 88, 80, 35 |
| 5 | 4465.164 | 4544.240 | −2209.582 | 0.710 | 0.2323 | 25, 59, 89, 48, 9 |
| 3* | 4467.644 | 4498.587 | −2224.822 | 0.774 | 0.0070 | 47, 133, 50 |
AIC = Akaike Information Criterion; BIC = Bayesian Information Criterion; L-M-R ALRT p = Lo-Mendell-Rubin Adjusted Likelihood Ratio Test p-value
Final 3-class model after removing slope and quadratic terms
The trajectories of the latent classes from the final 3-class model are graphed in Figure 1. All three latent classes in the growth mixture model had intercepts that significantly differed from zero, indicating differences in reparative behaviors at the first assessment, but did not have significant linear or quadratic slope components. Thus, no reparative behavior latent classes exhibited increasing (or decreasing) behaviors; instead, behaviors remained stable across time.
Figure 1.
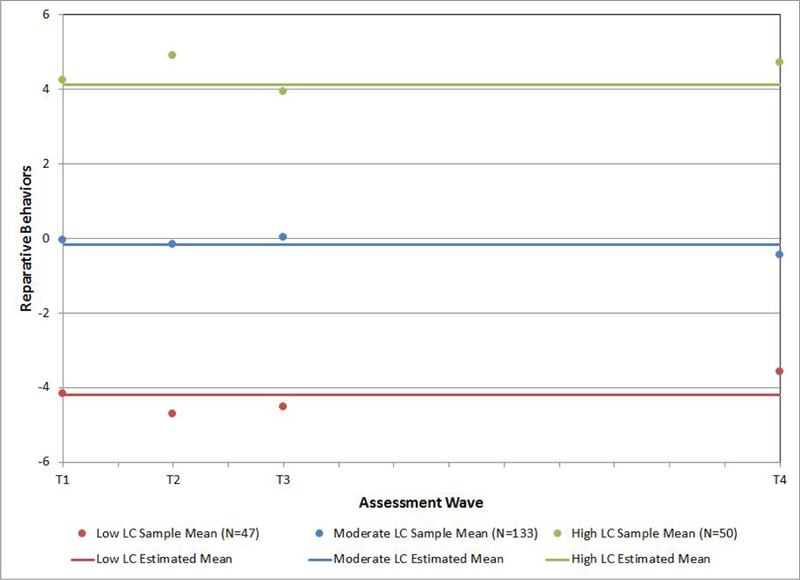
Latent class trajectories of reparative behaviors in participants (N = 230).
Predictors of latent class membership
Sex.
Results from the multinomial logistic regression indicated that child sex did not significantly predict latent class membership, χ2(2) = 1.40, p = .50.
Emotion understanding skills.
Emotion understanding skills as measured by the EmoDiff task were significantly associated with latent class membership. A 1-point decrease in emotion identification scores was associated with 1.12 times higher odds (95% CI 1.02 – 1.23) of being a member in the low rather than moderate latent class, χ2(1) = 6.18, p = .01. EmoDiff scores did not significantly differentiate the moderate and high classes, χ2(1) = .70, p = .40 or low and high classes, χ2(1) = 2.31, p = .13.
Social functioning.
The degree to which children were socially withdrawn was significantly associated with latent class. A 1-point increase in social withdrawal was associated with 3.73 times higher odds (95% CI 1.19 – 11.72) of being a member of the low rather than high latent class, χ2(1) = 5.08, p = .02. Social withdrawal did not significantly differentiate the low and moderate classes, χ2(1) = 2.11, p = .15 or the moderate and high classes, χ2(1) = 1.67, p = .20. Children’s peer rejection was also associated with latent class membership. A 1-point decrease in peer rejection (more rejection) was associated with 4.08 times higher odds (95% CI 1.48 – 11.24) of being a member of the low rather than high latent class, χ2(1) = 7.39, p = .01. Peer rejection did not significantly differentiate the low and moderate classes, χ2(1) = 3.57, p = .06, or moderate and high classes, χ2(1) = 2.40, p = .12.
Maladaptive guilt.
Children’s maladaptive guilt predicted children’s latent class membership. A 1-point increase in maladaptive guilt was associated with 1.22 times higher odds (95% CI 1.01 – 1.46) of being a member in the low rather than moderate latent class, χ2(1) = 4.47, p = .04, 1.21 times higher odds (95% CI 1.03 −1.41) of being a member in the moderate than high class, χ2(1) = 5.67, p = .02, and 1.47 times higher odds (95% CI 1.19 – 1.82) of being a member of the low than high class, χ2(1) = 12.38, p < .001.
Preschool-onset psychiatric diagnoses.
We tested for whether diagnostic status at baseline directly predicted latent class membership. Baseline MDD, externalizing disorder, and anxiety disorder were independent variables in the same multinomial logistic regression model.
Preschool-onset externalizing disorders.
Children with an externalizing diagnosis had 3.21 times higher odds (95% CI 1.47 – 6.99) of being in the low compared to moderate latent class, χ2(1) = 8.58, p = .003, 4.53 times higher odds (95% CI 1.45 – 14.13) of being in the moderate than high class χ2(1) = 6.78, p = .01, and 14.53 times higher odds (95% CI 4.16 – 50.69) of being in the low than high class, χ2(1) = 17.61, p < .001. We then examined ODD/CD and ADHD diagnoses separately by entering these two variables into the model in place of baseline externalizing disorder. Children with ODD or CD had 3.11 times higher odds (95% CI 1.39 – 6.97) of being in the low rather than moderate latent class, χ2(1) = 7.63, p = .01, 6.67 times higher odds (95% CI 1.45 – 30.61) of being in the moderate rather than high latent class, χ2(1) = 5.95, p = .02, and 20.77 times higher odds (95% CI 4.15 – 103.86) of being in the low rather than high latent class, χ2(1) = 13.64, p < .001. In contrast, an ADHD diagnosis did not predict odds of membership in the low compared to moderate, χ2(1) = 2.47, p = .12, moderate than high, χ2(1) = .13, p = .72, or low than high latent class, χ2(1) = 1.77, p = .18, indicating that results are primarily driven by children with ODD and CD.
Preschool-onset anxiety disorders.
Preschool-onset anxiety diagnoses did not predict odds of membership in the low compared to moderate, χ2(1) = .07, p = .80, moderate than high, χ2(1) = 1.13, p = .29, or low than high latent class, χ2(1) = 1.09, p = .30.
Preschool-onset MDD.
Children with a PO-MDD diagnosis had 3.37 times higher odds (95% CI 1.03 – 11.02) of being in the low rather than high latent class, χ2(1) = 4.02, p = .045. PO-MDD did not predict odds of being in the low than moderate class, χ2(1) = 2.27, p = .13 or moderate than high class, χ2(1) = 1.15, p = .28.
Maladaptive guilt as a mediator of PO-MDD and latent class membership.
Finally, we tested whether maladaptive guilt mediated the relationship between baseline PO-MDD and latent class membership. Methodological experts in mediation analysis recommend that researchers testing mediation move away from the Baron and Kenny (1986) causal steps logic; instead, they argue that a single inference about the indirect effect as quantified by (a*b) is alone sufficient to test mediation (Hayes & Rockwood, 2017). As shown in Figure 2, maladaptive guilt was a significant mediator of the relationship between PO-MDD and greater likelihood of membership in the low compared to moderate latent class of reparative behaviors. There was not a direct effect of PO-MDD on latent class membership (95% CI: −0.41 to 1.32), a common result when there is a mediation effect (Hayes & Rockwood, 2017). However, the indirect effect (a*b) was significant (95% CI: 0.05 to 0.74). This indicates that PO-MDD was related to membership in the low rather than moderate latent class of reparative behaviors through high levels of maladaptive guilt. Maladaptive guilt also significantly mediated the relationship between PO-MDD and greater likelihood of membership in the moderate compared to high class. Although there was not a direct effect of PO-MDD on latent class membership, (95% CI: −0.95 to 1.24), the indirect effect (a*b) was significant, (95% CI: .00 to .55), indicative of mediation. Finally, maladaptive guilt mediated the relationship between PO-MDD and greater likelihood of membership in the low than high class. There was not a direct effect of PO-MDD on latent class membership, (95% CI: −1.29 to 1.49), yet, the indirect effect (a*b) was significant, (95% CI: .00 to 1.70), indicative of mediation. Across these analyses, high levels of maladaptive guilt explained relations between PO-MDD and greater likelihood of membership in latent classes characterized by lower rather than higher levels of reparative behaviors.
Figure 2.
Indirect effects of maladaptive guilt in the relation between preschool-onset depression and lesser odds of membership in the A) moderate compared to low, B) high compared to moderate, and C) high compared to low latent class of reparative behaviors PO-MDD = preschool-onset depression

LC = latent class
*p<.05, **p<.001
Discussion
Despite the importance of reparative behaviors to children’s social and emotional functioning (e.g., Bafunno & Camodeca, 2013; Luby et al., 2009), very little is known about either the developmental course of these behaviors or factors that predict children’s reparative deficits. To address these gaps in the literature, this study applied GMM to reparative behaviors reported by children’s caregivers in a 9-year longitudinal dataset spanning from preschool through adolescence. We found evidence for three distinct trajectories of reparative behaviors—low, moderate, and high—that remained stable across development. The fact that all three trajectories were stable was of interest and suggests that such traits develop early and remain constant independent of other developmental changes. Contrary to hypotheses, child sex was not a significant predictor of latent class membership. However, consistent with hypotheses, emotion understanding abilities, social withdrawal and rejection, maladaptive guilt, and psychiatric diagnoses during the preschool period all differentiated latent class membership, some quite powerfully. Moreover, high levels of maladaptive guilt explained why preschoolers with depression were likely to be members of low-stable reparative behavior trajectories.
Similar to most studies of general prosocial behaviors (e.g., Cote et al., 2002), we found evidence of three trajectories in our sample reflecting low-stable, moderate-stable, and high-stable levels of reparative behaviors. However, our findings also differ from studies of general prosocial trajectories in two important ways. First, studies have documented decreases in general prosocial behaviors in pre-adolescence (Cote et al., 2002; Nantel-Vivier et al., 2014), which may reflect that prosocial behaviors become more targeted and selective with children’s increasing age as they learn more about when these behaviors are needed (for review, see: Hay & Cook, 2007). In contrast to these studies, we found no evidence of declining reparative tendencies during pre-adolescence; in fact, each of the three reparative trajectories were stable from preschool through adolescence. Second, several studies have found that boys are more likely to be members of low-stable general prosocial trajectories (Cote et al., 2002; Flynn et al., 2015; Nantel-Vivier et al., 2009, 2014), which may reflect socialization pressures for girls to disproportionately show caring behaviors (Brody, 2000). Contrary to this robust finding, child sex did not differentiate membership in latent classes of reparative behaviors. Unlike general prosocial behaviors, which involve a bystander’s choice of whether or not to help, reparative behaviors involve transgressor contexts in which a child has caused harm, and is thus responsible for mending the transgression (Tilghman-Osborne et al., 2010). It is possible that this awareness of responsibility leads to a steady motivation to act prosocially that persists regardless of typical age or gender-related influences. In sum, our findings further support that reparative behaviors are related to, yet distinct from, general prosocial tendencies and should thus be examined independently. Future studies that model joint trajectories of general prosocial and reparative behaviors would be informative to further distinguish their trajectories and identify common and distinct predictors.
Poorer socioemotional competence predicted children’s membership in trajectories characterized by lower reparative skills. Our findings suggest that socioemotional deficits during the preschool period, when skills for emotion understanding and successful peer interactions are developing, may have longstanding implications for children’s reparative functioning across a period of development spanning through adolescence. First, preschoolers with poorer emotion understanding abilities were more likely to be members in a latent class characterized by low-stable reparative behaviors. In contrast to previous studies which have assessed emotion understanding using puppets or pictoral faces, the current study assessed children’s abilities to discern actual facial expressions, which is likely a more ecologically valid context for elucidating how children’s poorer emotion understanding skills may impact their reparative abilities. Children who struggle to recognize and discern others’ emotional expressions are likely less able to both understand the consequences of their transgressions on others and also identify when a victim is in distress and could benefit from reparative skills. Children’s emotion understanding difficulties may be exacerbated over time, as children who fail to use reparative behaviors following transgressions miss opportunities for social interaction in which they would likely gain more experience with others’ emotions and the situations that elicit them. Thus, reparative difficulties may also predict future emotion understanding deficits; indeed, in one study, children’s lesser prosocial tendencies at age four predicted their poorer emotion understanding skills at age six (Eggum et al., 2011).
Second, children who were more socially withdrawn or rejected were likely to be members of latent classes characterized by lesser reparative behaviors. Children who have fewer social interactions likely have fewer opportunities to learn prosocial skills, as children learn these skills partially through social exposure and social learning experiences (Williamson, Donohue, & Tully, 2013). Further, there are likely bidirectional effects between social withdrawal and rejection and reparative difficulties; for example, rejected children are likely to respond with aggression and reduced prosocial behavior, which in turn may increase the extent to which these children are disliked and rejected (Sandstrom & Coie, 1999). Failing to use reparative skills may be particularly harmful to maintaining peer relationships, as children have a greater responsibility to help the victim of a transgression they have caused. Future studies that directly examine these potential bidirectional effects may help elucidate mechanisms through which peer difficulties and reparative deficits influence one another. In sum, our results support previous findings of associations between prosocial deficits and poorer emotion understanding (e.g., Ensor et al., 2011), social withdrawal (Findley & Ojanen, 2013) and rejection (Obsuth et al., 2015) and is the first to demonstrate that these socioemotional deficits are also associated with children’s greater difficulties using specifically reparative behaviors.
Children in this study with preschool-onset externalizing disorders and major depression were likely to be members of a low-stable reparative trajectory, supporting previous findings of associations between depression and externalizing diagnoses and prosocial deficits (Nantel-Vivier et al., 2014) and extending them to specifically reparative behaviors. The effect of an externalizing diagnosis on latent class membership was largely driven by children with ODD and CD, consistent with well-established deficits in empathy-based emotions and behaviors in these disorders (e.g., (Muris et al., 2016) We previously found that preschoolers in our sample with depression and externalizing diagnoses had concurrent reparative difficulties (Luby, Belden, Sullivan, et al., 2009); the current study extends this finding by demonstrating that, far from being a transient developmental phenomenon, preschool-onset psychiatric diagnoses predict children’s reparative deficits into adolescence. Moreover, high levels of maladaptive guilt explained why children with PO-MDD were more likely to be members of lower prosocial trajectories. This finding underscores the importance and specificity of maladaptive guilt experiences in preschool depression (Belden et al., 2015; Luby, Belden, Pautsch, Si, & Spitznagel, 2009; Luby, Belden, Sullivan, et al., 2009). Moreover, consistent with studies demonstrating that maladaptive guilt is associated with low levels of reparative behaviors in adults (e.g., Nencini & Meneghini, 2013), our finding provides the first evidence that maladaptive guilt also predicts reparative difficulty in children. Importantly, our finding suggests that maladaptive guilt is a mechanism through which PO-MDD is associated with long-standing reparative impairments that have broad implications for later social and emotional outcomes. Reparative deficits may be part of processes that maintain depression for children with PO-MDD, for example through leading to impaired peer relationships. Moreover, as reparative behaviors successfully alleviate guilt following transgressions (de Hooge, 2012), reparative difficulty may exacerbate depression through repeated experiences in which children’s guilt following transgressions remains unalleviated.
Clinical Implications
Our findings have implications for early interventions that target enhancement of the development of reparative behaviors. Such interventions might then serve to ameliorate psychopathology, particularly during early childhood when reparative behaviors are developing. As socioemotional deficits were found to detrimentally impact children’s reparative skills, interventions designed to enhance reparative behaviors should contain components to explicitly target children’s emotion understanding and social skills in order to have the greatest benefit. Studies have demonstrated that emotion understanding interventions in which children engage in conversations about the nature, causes, and regulation of emotions effectively increase general prosocial responding in toddlers and preschoolers (Grazzani, Ornaghi, Agliati, & Brazzelli, 2016; Ornaghi, Brazzelli, Grazzani, Agliati, & Lucarelli, 2017; Ornaghi, Grazzani, Cherubin, Conte, & Piralli, 2015). Moreover, social skills interventions have successfully targeted children’s social withdrawal and rejection (Barstead et al., 2018; Lochman, Coie, Underwood, & Terry, 1993). Our findings indicate that emotion understanding and social skills interventions may also be effective in increasing reparative behaviors. The only existing intervention that contains a component to increase children’s reparative skills is Parent-Child Interaction Therapy that added a novel emotion development module to target early childhood depression (PCIT-ED (Luby, Barch, Whalen, Tillman, & Freedland, 2018); in this treatment, parents were scaffolded in directly teaching children reparative skills, assuaging children’s maladaptive guilt, and helping children challenge cognitions that transgressions are irreparable. Compared to children in a wait-list control group, children in the PCIT-ED group evinced both significant declines in depressive severity and significant increases in reparative behaviors at the end of treatment, suggesting that reparative interventions are likely to have substantial benefit. Our findings suggest that these interventions should explicitly teach emotion identification (e.g., recognizing and labeling facial expressions) and promote social approach to both prevent social withdrawal as well as to provide opportunities for children to learn and practice social skills that may help prevent social rejection. Importantly, the fact that reparative trajectories were stable across development in our sample as early as 3 years of age suggests that reparative interventions may need to be implemented in toddlerhood in order to have the greatest benefit.
Limitations
Several study limitations should be mentioned. Although the measure of reparative behaviors used in the current study demonstrated good internal consistency and the same factor structure across study timepoints, it was originally designed for use with children 6-years-old and younger, and was thus slightly modified with developmentally appropriate wording for use with the older children in this study. Similarly, although the reparative behavior questionnaire utilized in this study is the most widely used measure of reparative behaviors in children, future studies of reparative trajectories might include additional measures of reparative behavior, such as observational measures. Although this study aimed to examine aspects of children’s social and emotional development that had not previously been examined as predictors of prosocial trajectories, future studies might examine the impact of aspects of the child’s environment, such as social and parenting factors, on children’s reparative behavior trajectories. For example, warm, supportive parenting has been consistently associated with promoting prosocial development, and harsh parenting strategies associated with decreasing children’s prosocial tendencies (Grusec, Hastings, & Almas, 2014). Whether reparative behaviors are influenced by the same or distinct parent socialization factors as general prosocial behaviors remains unexplored.
Conclusion
This study found that children’s reparative behaviors from preschool through adolescence followed three stable trajectories characterized by low, moderate, and high levels of reparative skills. Further, we identified child factors in the preschool period that predicted longitudinal reparative difficulty including poorer emotion understanding skills, greater social withdrawal, greater peer rejection, greater maladaptive guilt, and preschool-onset MDD and externalizing diagnoses. High maladaptive guilt was a process through which preschoolers with MDD were likely to be members of a low-stable reparative trajectory. Overall, this study contributes new knowledge about the developmental trajectories of specifically reparative behaviors and elucidates predictors of reparative difficulties that are modifiable and should be targeted in early reparative interventions.
Table 2.
Results of Principal Components Analyses of My-Child at T1, T2, T3 and T4
| Subscale | Factor Loadings |
|||||||
|---|---|---|---|---|---|---|---|---|
| Reparation Behaviors | Maladaptive Guil | |||||||
| T1 | T2 | T3 | T4 | T1 | T2 | T3 | T4 | |
| 1. Amends | .81 | .80 | .83 | .84 | .30 | .33 | .17 | .28 |
| 2. Internalized Conduct | .78 | .79 | .81 | .79 | −.03 | −.10 | −.06 | −.05 |
| 3. Confession | .75 | .73 | .81 | .80 | .13 | .21 | .16 | .21 |
| 4. Prosocial Response | .71 | .62 | .64 | .65 | .26 | .34 | .31 | .40 |
| 5. Concern Over Others’ Transgressions | .63 | .57 | .71 | .70 | .26 | .35 | .19 | .09 |
| 6. Apology | .58 | .73 | .70 | .81 | .07 | .11 | .18 | .18 |
| 7. Symbolic Representation | −.31 | −.38 | −.24 | −.40 | .73 | .68 | .81 | .73 |
| 8. Guilt | .33 | .26 | .49 | .33 | .71 | .77 | .67 | .70 |
| 9. Concern Over Parent Feelings After Transgression | .25 | .35 | .25 | .48 | .66 | .66 | .76 | .57 |
| 10. Sensitivity to Themes of Wrongdoing | .33 | .32 | .31 | .23 | .60 | .66 | .65 | .73 |
| Variance | 35% | 35% | 38% | 41% | 21% | 23% | 23% | 22% |
| Eigenvalue | 4.02 | 4.24 | 4.50 | 4.69 | 1.48 | 1.57 | 1.66 | 1.60 |
Acknowledgements
All phases of this study were supported by an NIH grant (R01 MH064769–06A1). Dr. Donohue’s work was supported by NIH grant T32 MH100019 (PIs: Barch and Luby).
Footnotes
The authors report no conflicts of interest.
References
- Albanese O, Grazzani I, Molina P, Antoniotti C, Aratti L, Farina E, & Pons F (2006). Children’s emotion understanding: Preliminary data of the italian validation project of Test of Emotion Comprehension (T.E.C). In Toward Emotional Competences (pp. 39–53). Aalborg, Denmark: Aalborg University Press. [Google Scholar]
- Armstrong J, & Goldstein L (2003). Manual for the MacArthur health and behavior questionnaire (HBQ 1.0). MacArthur Foundation Research Network on Psychopathology and Development, University of Pittsburgh. [Google Scholar]
- Bafunno D, & Camodeca M (2013). Shame and guilt development in preschoolers: The role of context, audience and individual characteristics. European Journal of Developmental Psychology, 10(2), 128–143. 10.1080/17405629.2013.765796 [DOI] [Google Scholar]
- Barrett KC, Zahn-Waxler C, & Cole PM (1993). Avoiders vs amenders: Implications for the investigation of guilt and shame during toddlerhood? Cognition and Emotion, 7(6), 481–505. 10.1080/02699939308409201 [DOI] [Google Scholar]
- Barstead MG, Danko CM, Chronis-Tuscano A, O’Brien KA, Coplan RJ, & Rubin KH (2018). Generalization of an Early Intervention for Inhibited Preschoolers to the Classroom Setting. Journal of Child and Family Studies, 27(9), 2943–2953. 10.1007/s10826-018-1142-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belacchi C, & Farina E (2010). Prosocial/hostile roles and emotion comprehension in preschoolers. Aggressive Behavior, 36(6), 371–389. 10.1002/ab.20361 [DOI] [PubMed] [Google Scholar]
- Belden AC, Barch DM, Oakberg TJ, April LM, Harms MP, Botteron KN, & Luby JL (2015). Anterior Insula Volume and Guilt: Neurobehavioral Markers of Recurrence After Early Childhood Major Depressive Disorder. JAMA Psychiatry, 72(1), 40 10.1001/jamapsychiatry.2014.1604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody LR (2000). The socialization of gender differences in emotional expression: Display rules, infant temperament, and differentiation. Gender and Emotion: Social Psychological Perspectives, 2. [Google Scholar]
- Caprara GV, Barbaranelli C, Pastorelli C, Bandura A, & Zimbardo PG (2000). Prosocial Foundations of Children’s Academic Achievement. Psychological Science, 11(4), 302–306. 10.1111/1467-9280.00260 [DOI] [PubMed] [Google Scholar]
- Caprara GV, Barbaranelli C, Pastorelli C, Cermak I, & Rosza S (2001). Facing guilt: Role of negative affectivity, need for reparation, and fear of punishment in leading to prosocial behaviour and aggression. European Journal of Personality, 15(3), 219–237. 10.1002/per.402 [DOI] [Google Scholar]
- Carlo G, Crockett LJ, Randall BA, & Roesch SC (2007). A Latent Growth Curve Analysis of Prosocial Behavior Among Rural Adolescents. Journal of Research on Adolescence, 17(2), 301–324. 10.1111/j.1532-7795.2007.00524.x [DOI] [Google Scholar]
- Cohen TR, Wolf ST, Panter AT, & Insko CA (2011). Introducing the GASP scale: A new measure of guilt and shame proneness. Journal of Personality and Social Psychology, 100(5), 947–966. 10.1037/a0022641 [DOI] [PubMed] [Google Scholar]
- Colasante T, Zuffianò A, Bae NY, & Malti T (2014). Inhibitory Control and Moral Emotions: Relations to Reparation in Early and Middle Childhood. The Journal of Genetic Psychology, 175(6), 511–527. 10.1080/00221325.2014.976535 [DOI] [PubMed] [Google Scholar]
- Cote S, Tremblay RE, Nagin D, Zoccolillo M, & Vitaro F (2002). The development of impulsivity, fearfulness, and helpfulness during childhood: patterns of consistency and change in the trajectories of boys and girls. Journal of Child Psychology and Psychiatry, 43(5), 609–618. 10.1111/1469-7610.00050 [DOI] [PubMed] [Google Scholar]
- Cryder CE, Springer S, & Morewedge CK (2012). Guilty Feelings, Targeted Actions. Personality and Social Psychology Bulletin, 38(5), 607–618. 10.1177/0146167211435796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Hooge IE (2012). The exemplary social emotion guilt: Not so relationship-oriented when another person repairs for you. Cognition & Emotion, 26(7), 1189–1207. 10.1080/02699931.2011.640663 [DOI] [PubMed] [Google Scholar]
- Demetriou H, & Hay DF (2004). Toddlers’ Reactions to the Distress of Familiar Peers: The Importance of Context. Infancy, 6(2), 299–318. 10.1207/s15327078in0602_9 [DOI] [PubMed] [Google Scholar]
- Denham SA (1986). Social Cognition, Prosocial Behavior, and Emotion in Preschoolers: Contextual Validation. Child Development, 57, 194–201. [Google Scholar]
- Denham SA (2006). Emotional Competence: Implications for Social Functioning. In Luby JL (Ed.), Handbook of preschool mental health: Development, disorders, and treatment (pp. 23–44). New York, NY: Guilford Press; Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2006-10334-002&site=ehost-live [Google Scholar]
- Denham SA, Blair KA, DeMulder E, Levitas J, Sawyer K, Auerbach-Major S, & Queenan P (2003). Preschool Emotional Competence: Pathway to Social Competence? Child Development, 74(1), 238–256. 10.1111/1467-8624.00533 [DOI] [PubMed] [Google Scholar]
- Denham SA, & Couchoud EA (1991). Social-Emotional Predictors of Preschoolers’ Responses to Adult Negative Emotion. Journal of Child Psychology and Psychiatry, 32(4), 595–608. 10.1111/j.1469-7610.1991.tb00337.x [DOI] [PubMed] [Google Scholar]
- Di Giunta L, Pastorelli C, Thartori E, Bombi AS, Baumgartner E, Fabes RA, … Enders CK (2018). Trajectories of Italian Children’s Peer Rejection: Associations with Aggression, Prosocial Behavior, Physical Attractiveness, and Adolescent Adjustment. Journal of Abnormal Child Psychology, 46(5), 1021–1035. 10.1007/s10802-017-0373-7 [DOI] [PubMed] [Google Scholar]
- Diesendruck G, & Ben-Eliyahu A (2006). The relationships among social cognition, peer acceptance, and social behavior in Israeli kindergarteners. International Journal of Behavioral Development, 30(2), 137–147. 10.1177/0165025406063628 [DOI] [Google Scholar]
- Dunfield KA (2014). A construct divided: prosocial behavior as helping, sharing, and comforting subtypes. Frontiers in Psychology, 5 10.3389/fpsyg.2014.00958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn J, & Brown J (1994). Affect Expression in the Family, Children’s Understanding of Emotions, and Their Interactions With Others. Merrill-Palmer Quarterly, 40(1), 120–137. [Google Scholar]
- Dunn J, Brown J, Slomkowski C, Tesla C, & Youngblade L (1991). Young Children’s Understanding of Other People’s Feelings and Beliefs: Individual Differences and Their Antecedents. Child Development, 62, 1352–1366. [PubMed] [Google Scholar]
- Egger HL, Ascher B, & Angold A (2003). The preschool age psychiatric assessment: version 1.4. Center for Developmental Epidemiology, Department of Psychiatry and Behavioral Sciences Duke University Medical Center. [Google Scholar]
- Eggum ND, Eisenberg N, Kao K, Spinrad TL, Bolnick R, Hofer C, … Fabricius WV (2011). Emotion understanding, theory of mind, and prosocial orientation: Relations over time in early childhood. The Journal of Positive Psychology, 6(1), 4–16. 10.1080/17439760.2010.536776 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Eggum ND, & Di Giunta L (2010). Empathy-Related Responding: Associations with Prosocial Behavior, Aggression, and Intergroup Relations: Empathy-Related Responding. Social Issues and Policy Review, 4(1), 143–180. 10.1111/j.1751-2409.2010.01020.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, & Fabes RA (1998). Prosocial development. In Eisenberg N (Ed.), Handbook of child psychology: Social, emotional, and personality development, Vol. 3, 5th ed. (pp. 701–778). Hoboken, NJ: John Wiley & Sons Inc; Retrieved from http://libproxy.wustl.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2005-03132-011&site=ehost-live&scope=site [Google Scholar]
- Ely R, & Gleason JB (2006). I’m sorry I said that: apologies in young children’s discourse. Journal of Child Language, 33(03), 599 10.1017/S0305000906007446 [DOI] [PubMed] [Google Scholar]
- Ensor R, & Hughes C (2005). More than talk: Relations between emotion understanding and positive behaviour in toddlers. British Journal of Developmental Psychology, 23(3), 343–363. 10.1348/026151005X26291 [DOI] [Google Scholar]
- Ensor R, Spencer D, & Hughes C (2011). ‘You Feel Sad?’ Emotion Understanding Mediates Effects of Verbal Ability and Mother-Child Mutuality on Prosocial Behaviors: Findings from 2 Years to 4 Years: Prosocial Behavior, Emotion Understanding. Social Development, 20(1), 93–110. 10.1111/j.1467-9507.2009.00572.x [DOI] [Google Scholar]
- Estrada-Hollenbeck M, & Heatherton TF (1998). Avoiding and alleviating guilt through prosocial behavior. In Guilt and children (pp. 215–231). Elsevier. [Google Scholar]
- Findley D, & Ojanen T (2013). Adolescent resource control: Associations with physical and relational aggression, prosocial and withdrawn behaviors, and peer regard. International Journal of Behavioral Development, 37(6), 518–529. 10.1177/0165025413503420 [DOI] [Google Scholar]
- Flynn E, Ehrenreich SE, Beron KJ, & Underwood MK (2015). Prosocial Behavior: Long-term Trajectories and Psychosocial Outcomes: Prosocial Trajectories. Social Development, 24(3), 462–482. 10.1111/sode.12100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grazzani I, Ornaghi V, Agliati A, & Brazzelli E (2016). How to Foster Toddlers’ Mental-State Talk, Emotion Understanding, and Prosocial Behavior: A Conversation-Based Intervention at Nursery School. Infancy, 21(2), 199–227. 10.1111/infa.12107 [DOI] [Google Scholar]
- Grusec JE, Hastings P, & Almas A (2014). Prosocial behavior. In Smith PK & Hart CH (Eds.), The Wiley Blackwell handbook of childhood social development, 2nd ed. (pp. 549–566). Wiley-Blackwell; Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2014-08957-029&site=ehost-live [Google Scholar]
- Gur RC, Richard J, Hughett P, Calkins ME, Macy L, Bilker WB, … Gur RE (2010). A cognitive neuroscience-based computerized battery for efficient measurement of individual differences: Standardization and initial construct validation. Journal of Neuroscience Methods, 187(2), 254–262. 10.1016/j.jneumeth.2009.11.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hay DF, & Cook KV (2007). The transformation of prosocial behavior from infancy to childhood. In Brownell CA & Kopp CB (Eds.), Socioemotional development in the toddler years: Transitions and transformations (pp. 100–131). New York, NY: Guilford Press; Retrieved from http://libproxy.wustl.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2007-15136-004&site=ehost-live&scope=site [Google Scholar]
- Hay DF, & Pawlby S (2003). Prosocial Development in Relation to Children’s and Mothers’ Psychological Problems. Child Development, 74(5), 1314–1327. 10.1111/1467-8624.00609 [DOI] [PubMed] [Google Scholar]
- Hayes AF (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling. White Paper
- Hayes AF, & Preacher KJ (2014). Statistical mediation analysis with a multicategorical independent variable. British Journal of Mathematical and Statistical Psychology, 67(3), 451–470. 10.1111/bmsp.12028 [DOI] [PubMed] [Google Scholar]
- Hayes AF, & Rockwood NJ (2017). Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behaviour Research and Therapy, 98, 39–57. 10.1016/j.brat.2016.11.001 [DOI] [PubMed] [Google Scholar]
- Howell AJ, Dopko RL, Turowski JB, & Buro K (2011). The disposition to apologize. Personality and Individual Differences, 51(4), 509–514. 10.1016/j.paid.2011.05.009 [DOI] [Google Scholar]
- Jones WH, & Kugler K (1993). Interpersonal Correlates of the Guilt Inventory. Journal of Personality Assessment, 61(2), 246–258. 10.1207/s15327752jpa6102_6 [DOI] [PubMed] [Google Scholar]
- Jung T, & Wickrama KAS (2008). An Introduction to Latent Class Growth Analysis and Growth Mixture Modeling. Social and Personality Psychology Compass, 2(1), 302–317. 10.1111/j.1751-9004.2007.00054.x [DOI] [Google Scholar]
- Kochanska G (1991). Socialization and temperament in the development of guilt and conscience. Child Development, 62(62). [PubMed] [Google Scholar]
- Kochanska G, DeVet K, Murray K, & Putnam SP (1994). Maternal Reports of Conscience Development and Temperament in Young Children. Child Development, 65(3), 852–868. [PubMed] [Google Scholar]
- Kochanska G, Gross JN, Lin M-H, & Nichols KE (2002). Guilt in young children: Development, determinants, and relations with a broader system of standards. Child Development, 73(2), 461–482. 10.1111/1467-8624.00418 [DOI] [PubMed] [Google Scholar]
- Kochanska G, Koenig JL, Barry RA, Kim S, & Yoon JE (2010). Children’s conscience during toddler and preschool years, moral self, and a competent, adaptive developmental trajectory. Developmental Psychology, 46(5), 1320–1332. 10.1037/a0020381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ladd GW, & Profilet SM (1996). The Child Behavior Scale: A teacher report measure of young children’s aggressive, withdrawn, and prosocial behaviors. Developmental Psychology, 32(6), 1008–1024. [Google Scholar]
- LaFontana KM, & Cillessen AHN (2002). Children’s perceptions of popular and unpopular peers: A multimethod assessment. Developmental Psychology, 38(5), 635–647. 10.1037//0012-1649.38.5.635 [DOI] [PubMed] [Google Scholar]
- Lewis M (2008). Self-conscious emotions: Embarrassment, pride, shame, and guilt. In Lewis M, Haviland-Jones JM, & Barrett LF (Eds.), Handbook of emotions, 3rd ed. (pp. 742–756). New York, NY: Guilford Press; Retrieved from http://libproxy.wustl.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2008-07784-046&site=ehost-live&scope=site [Google Scholar]
- Lichter DT, Shanahan MJ, & Gardner EL (2002). Helping Others?: The Effects of Childhood Poverty and Family Instability on Prosocial Behavior. Youth & Society, 34(1), 89–119. 10.1177/0044118X02034001004 [DOI] [Google Scholar]
- Lochman JE, Coie JD, Underwood MK, & Terry R (1993). Effectiveness of a Social Relations Intervention Program for Aggressive and Nonaggressive, Rejected Children. Journal of Consulting and Clinical Psychology, 61(6), 1053–1058. [DOI] [PubMed] [Google Scholar]
- Luby JL, Barch DM, Whalen D, Tillman R, & Freedland KE (2018). A Randomized Controlled Trial of Parent-Child Psychotherapy Targeting Emotion Development for Early Childhood Depression. American Journal of Psychiatry, appi.ajp.2018.1. 10.1176/appi.ajp.2018.18030321 [DOI] [PMC free article] [PubMed]
- Luby JL, Belden AC, Pautsch J, Si X, & Spitznagel E (2009). The clinical significance of preschool depression: Impairment in functioning and clinical markers of the disorder. Journal of Affective Disorders, 112(1–3), 111–119. 10.1016/j.jad.2008.03.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luby JL, Belden A, Sullivan J, Hayen R, McCadney A, & Spitznagel E (2009). Shame and guilt in preschool depression: evidence for elevations in self-conscious emotions in depression as early as age 3. Journal of Child Psychology and Psychiatry, 50(9), 1156–1166. 10.1111/j.1469-7610.2009.02077.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luby JL, Heffelfinger AK, Mrakotsky C, Hessler MJ, Brown KM, & Hildebrand T (2002). Preschool Major Depressive Disorder: Preliminary Validation for Developmentally Modified DSM-IV Criteria. Journal of the American Academy of Child & Adolescent Psychiatry, 41(8), 928–937. 10.1097/00004583-200208000-00011 [DOI] [PubMed] [Google Scholar]
- Luby JL, Heffelfinger A, Koenig-McNaught AL, Brown K, & Spitznagel E (2004). The Preschool Feelings Checklist: A Brief and Sensitive Screening Measure for Depression in Young Children. Journal of the American Academy of Child & Adolescent Psychiatry, 43(6), 708–717. 10.1097/01.chi.0000121066.29744.08 [DOI] [PubMed] [Google Scholar]
- Luby JL, Si X, Belden AC, Tandon M, & Spitznagel E (2009). Preschool Depression: Homotypic Continuity and Course Over 24 Months. Archives of General Psychiatry, 66(8), 897 10.1001/archgenpsychiatry.2009.97 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luyten P, Fontaine JR ., & Corveleyn J (2002). Does the Test of Self-Conscious Affect (TOSCA) measure maladaptive aspects of guilt and adaptive aspects of shame? An empirical investigation. Personality and Individual Differences, 33(8), 1373–1387. 10.1016/S0191-8869(02)00197-6 [DOI] [Google Scholar]
- McLoyd VC (1998). Socioeconomic Disadvantage and Child Development. American Psychologist, 20. [DOI] [PubMed] [Google Scholar]
- Muris P, & Meesters C (2014). Small or Big in the Eyes of the Other: On the Developmental Psychopathology of Self-Conscious Emotions as Shame, Guilt, and Pride. Clinical Child and Family Psychology Review, 17(1), 19–40. 10.1007/s10567-013-0137-z [DOI] [PubMed] [Google Scholar]
- Muris P, Meesters C, Heijmans J, van Hulten S, Kaanen L, Oerlemans B, … Tielemans T (2016). Lack of guilt, guilt, and shame: a multi-informant study on the relations between self-conscious emotions and psychopathology in clinically referred children and adolescents. European Child & Adolescent Psychiatry, 25(4), 383–396. 10.1007/s00787-015-0749-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén B, & Muthén LK (2000). Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcoholism: Clinical and Experimental Research, 24(6), 882–891. [PubMed] [Google Scholar]
- Nagin DS (1999). Analyzing developmental trajectories: A semiparametric, group-based approach. Psychology of Methods, 4(2), 139–157. [Google Scholar]
- Nantel-Vivier A, Kokko K, Caprara GV, Pastorelli C, Gerbino MG, Paciello M, … Tremblay RE (2009). Prosocial development from childhood to adolescence: a multi-informant perspective with Canadian and Italian longitudinal studies. Journal of Child Psychology and Psychiatry, 50(5), 590–598. 10.1111/j.1469-7610.2008.02039.x [DOI] [PubMed] [Google Scholar]
- Nantel-Vivier A, Pihl RO, Côté S, & Tremblay RE (2014). Developmental association of prosocial behaviour with aggression, anxiety and depression from infancy to preadolescence. Journal of Child Psychology and Psychiatry, 55(10), 1135–1144. 10.1111/jcpp.12235 [DOI] [PubMed] [Google Scholar]
- Nencini A, & Meneghini AM (2013). How relational bonds influence strategies for coping with guilt. Journal of Relationships Research, 4 Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2014-15784-001&site=ehost-live [Google Scholar]
- Nylund KL, Asparouhov T, & Muthén BO (2007). Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569. 10.1080/10705510701575396 [DOI] [Google Scholar]
- Obsuth I, Eisner MP, Malti T, & Ribeaud D (2015). The developmental relation between aggressive behaviour and prosocial behaviour: A 5-year longitudinal study. BMC Psychology, 3(1). 10.1186/s40359-015-0073-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ornaghi V, Brazzelli E, Grazzani I, Agliati A, & Lucarelli M (2017). Does Training Toddlers in Emotion Knowledge Lead to Changes in Their Prosocial and Aggressive Behavior Toward Peers at Nursery? Early Education and Development, 28(4), 396–414. 10.1080/10409289.2016.1238674 [DOI] [Google Scholar]
- Ornaghi V, Grazzani I, Cherubin E, Conte E, & Piralli F (2015). ‘Let’s Talk about Emotions!’. The Effect of Conversational Training on Preschoolers’ Emotion Comprehension and Prosocial Orientation: Emotion Comprehension and Prosocial Orientation. Social Development, 24(1), 166–183. 10.1111/sode.12091 [DOI] [Google Scholar]
- Ornaghi V, Pepe A, & Grazzani I (2016). False-Belief Understanding and Language Ability Mediate the Relationship between Emotion Comprehension and Prosocial Orientation in Preschoolers. Frontiers in Psychology, 7 10.3389/fpsyg.2016.01534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Toole SE, Monks CP, & Tsermentseli S (2017). Executive function and theory of mind as predictors of aggressive and prosocial behavior and peer acceptance in early childhood. Social Development, 26(4), 907–920. 10.1111/sode.12231 [DOI] [Google Scholar]
- Padilla-Walker LM, Dyer WJ, Yorgason JB, Fraser AM, & Coyne SM (2015). Adolescents’ Prosocial Behavior Toward Family, Friends, and Strangers: A Person-Centered Approach. Journal of Research on Adolescence, 25(1), 135–150. 10.1111/jora.12102 [DOI] [Google Scholar]
- Peters E, Cillessen AHN, Riksen-Walraven JM, & Haselager GJT (2010). Best friends’ preference and popularity: Associations with aggression and prosocial behavior. International Journal of Behavioral Development, 34(5), 398–405. 10.1177/0165025409343709 [DOI] [Google Scholar]
- Pettygrove DM, Hammond SI, Karahuta EL, Waugh WE, & Brownell CA (2013). From cleaning up to helping out: Parental socialization and children’s early prosocial behavior. Infant Behavior and Development, 36(4), 843–846. 10.1016/j.infbeh.2013.09.005 [DOI] [PubMed] [Google Scholar]
- Pons F, Harris PL, & de Rosnay M (2004). Emotion comprehension between 3 and 11 years: Developmental periods and hierarchical organization. European Journal of Developmental Psychology, 1(2), 127–152. 10.1080/17405620344000022 [DOI] [Google Scholar]
- Quiles ZN, & Bybee J (1997). Chronic and predispositional guilt: Relations to mental health, prosocial behavior, and religiosity. Journal of Personality Assessment, 69(1), 104–126. [DOI] [PubMed] [Google Scholar]
- Rakow A, Forehand R, McKee L, Coffelt N, Champion J, Fear J, & Compas B (2009). The Relation of Parental Guilt Induction to Child Internalizing Problems When a Caregiver Has a History of Depression. Journal of Child and Family Studies, 18(4), 367–377. 10.1007/s10826-008-9239-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubin KH, & Coplan RJ (2004). Paying Attention to and Not Neglecting Social Withdrawal and Social Isolation. Merrill-Palmer Quarterly, 50(4), 506–534. 10.1353/mpq.2004.0036 [DOI] [Google Scholar]
- Saarni C, Campos JJ, Camras LA, & Witherington D (2006). Emotional Development: Action, Communication, and Understanding. In Eisenberg N, Damon W, & Lerner RM (Eds.), Handbook of child psychology: Social, emotional, and personality development, Vol. 3, 6th ed. (pp. 226–299). Hoboken, NJ: John Wiley & Sons Inc; Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2006-08776-005&site=ehost-live [Google Scholar]
- Sandstrom MJ, & Coie JD (1999). A Developmental Perspective on Peer Rejection: Mechanisms of Stability and Change. Child Development, 70(4), 955–966. 10.1111/1467-8624.00069 [DOI] [PubMed] [Google Scholar]
- Svetlova M, Nichols SR, & Brownell CA (2010). Toddlers’ Prosocial Behavior: From Instrumental to Empathic to Altruistic Helping: Toddlers’ Prosocial Behavior. Child Development, 81(6), 1814–1827. 10.1111/j.1467-8624.2010.01512.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tangney JP, Stuewig J, & Mashek DJ (2007). Moral Emotions and Moral Behavior. Annual Review of Psychology, 58(1), 345–372. 10.1146/annurev.psych.56.091103.070145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tilghman-Osborne C, Cole DA, & Felton JW (2010). Definition and measurement of guilt: Implications for clinical research and practice. Clinical Psychology Review, 30(5), 536–546. 10.1016/j.cpr.2010.03.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tilghman-Osborne C, Cole DA, & Felton JW (2012). Inappropriate and Excessive Guilt: Instrument Validation and Developmental Differences in Relation to Depression. Journal of Abnormal Child Psychology, 40(4), 607–620. 10.1007/s10802-011-9591-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whalen DJ, Belden AC, Tillman R, Barch DM, & Luby JL (2016). Early Adversity, Psychopathology, and Latent Class Profiles of Global Physical Health From Preschool Through Early Adolescence: Psychosomatic Medicine, 78(9), 1008–1018. 10.1097/PSY.0000000000000398 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widen SC, & Russell JA (2003). A closer look at preschoolers’ freely produced labels for facial expressions. Developmental Psychology, 39(1), 114–128. 10.1037/0012-1649.39.1.114 [DOI] [PubMed] [Google Scholar]
- Williamson RA, Donohue MR, & Tully EC (2013). Learning how to help others: Two-year-olds’ social learning of a prosocial act. Journal of Experimental Child Psychology, 114(4), 543–550. 10.1016/j.jecp.2012.11.004 [DOI] [PubMed] [Google Scholar]
- Zahn-Waxler C, Radkerrow M, Wagner E, & Chapman M (1992). Development of Concern for Others. Developmental Psychology, 28(1), 126–136. [Google Scholar]
- Zahn-Waxler C, Radke-Yarrow M, & King RA (1979). Child rearing and children’s prosocial initiations toward victims of distress. Child Development, 50(2), 319–330. 10.2307/1129406 [DOI] [PubMed] [Google Scholar]