

ABSTRACT
In this article, we review the evidence underpinning the broader prehabilitation concept and the target behavioural and lifestyle risk factors including their perioperative impact and evidence for prehabilitation intervention. We also identify principles for delivering prehabilitation in practice, alongside lessons for the perioperative setting from well-established allied interventions; cardiac and pulmonary rehabilitation.
KEYWORDS: Perioperative, surgery, prehabilitation, exercise, smoking, alcohol, cancer
Major surgery in the UK: Why complications matter
The UK NHS undertakes approximately 2,414 major elective surgical procedures per 100,000 population annually.1 Surgery involving a major body cavity provokes a global neuroendocrine inflammatory response, placing significant physiological strain upon the patient.2 Mortality is estimated at up to 4% with attention increasingly focused upon surgical morbidity as a key driver of postoperative death.3 Postoperative complications affect 15–40% of patients.4 The immediate impact is stark, including a 2–4 fold increase in hospital length of stay (HLOS) and increased readmissions.5,6 The NHS cost impact is substantial, inflating the £5.6 billion burden of major elective surgery.1 Equally concerning is the longer-term impact on patients. Many fail to regain their preoperative functional status and independence.7 These factors undermine health related quality of life (HRQOL).8 Following adjustment, a postoperative complication reduces life expectancy for years following discharge.9
A range of factors determines complication risk. The ‘high-risk’ surgical patient is typically older, demonstrates multiple comorbidities and may be frail.10 Lifestyle and behavioural factors also elevate risk including physical inactivity and poor fitness, smoking, hazardous drinking, malnutrition and adverse psychological factors. Collectively these reduce the body's resilience to manage the physiological stress of the operation. The physiological challenge of major surgery has been likened to running a marathon. In both cases, preparation is critical. ‘Prehabilitation’ aims to enhance general health and wellbeing prior to major surgery. By intervening in the preoperative period to modify behavioural and lifestyle risk factors, the ‘physiological reserve’ of the patient is enhanced to buffer the surgical stress response.11
Fit to fight: Prehabilitation for major surgery
Prehabilitation prepares individuals to ‘weather the storm’ of their operation and to avoid or overcome complications (Fig 1). The preoperative period is considered a ‘teachable moment’ in healthcare.12 During this window, individuals may be more receptive to structured behavioural intervention. Our recent research has highlighted a high degree of patient motivation to change behaviour for perioperative benefits, however a comparative lack of confidence identified a need for structured support.13 The wider public health opportunity offered by surgery to embed lasting lifestyle change should not be ignored. Effective prehabilitation is person centred, placing the patient at the core of their perioperative journey. Patients can regain some control over their own outcomes. Prehabilitation support should be multidisciplinary and cross healthcare sectors, requiring expertise and input from a range of professionals (Fig 2).
Fig 1.
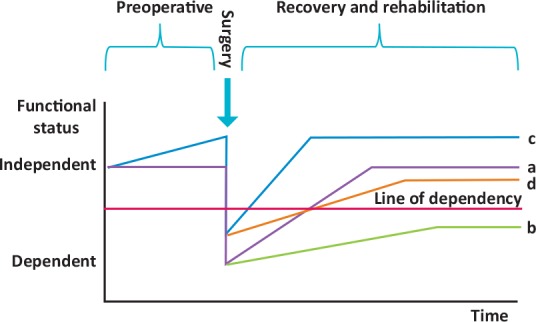
The prehabilitation concept. a) All patients undergoing surgery experience a reduction in functional status postoperatively followed by a recovery period. b) Patients suffering a complication may experience a slower and incomplete recovery threatening longer-term independence. c) Prehabilitated patients are better placed to cope. d) Should a complication occur, prehabilitation might be crucial to safeguarding longer-term functional status and independence. Reproduced and adapted with permission from Tew GA, Ayyash R, Durrand J, Danjoux GR. Clinical guideline and recommendations on pre-operative exercise training in patients awaiting major non-cardiac surgery. Anaesthesia 2018;73:750–68.
Fig 2.
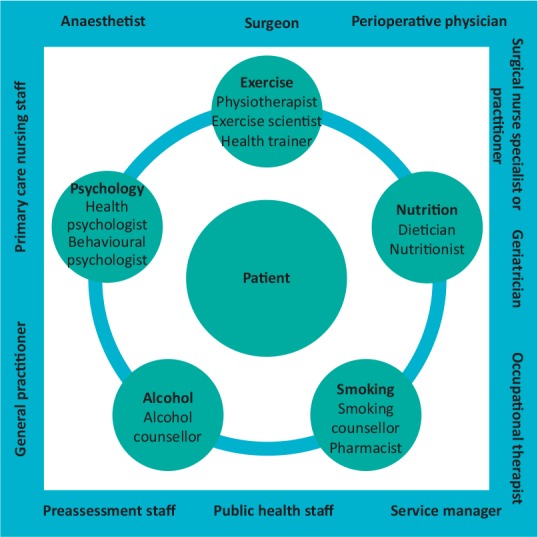
The multidisciplinary prehabilitation team. With the patient as the key member, involvement of all clinical and non-clinical staff in the preoperative pathway as members of the prehabilitation team is crucial to facilitate optimal use of available preoperative time and ‘make every contact count’ to support behaviour change prior to surgery.
Unhealthy behaviours and lifestyle factors frequently cluster in the same individual and may be particularly common in surgical populations, driving development of surgical pathologies.13,14 In our recent study, 42% of patients demonstrated two or more risk factors. This emphasises both the possibility of a ‘risk multiplier’ effect from several risk factors, and the need for multimodal intervention to modify factors simultaneously in the potentially time-pressured preoperative window.13 Evidence exists suggesting multimodal intervention may be more effective than single or sequential intervention but this is not fully established.15 Sequential intervention may be too lengthy for the preoperative timeframe and the order in which to prioritise risk factors is unclear. There may be a synergistic benefit to multiple interventions, for example, increased activity may facilitate weight loss, with nutritional support underpinning improvement in body composition resulting from exercise. Critically, the target factors must be determined collaboratively with the individual through appropriate goal setting. Models of prehabilitation should also generally encompass three stages, screening, intervention and monitoring, alongside post-intervention evaluation for benefit.
Risk factor prehabilitation
Prehabilitation can be offered to all patients undergoing major surgery, however the scope and intensity will vary. A ‘tiered’ approach has been proposed (Fig 3).16 Table 1 provides a summary of specific screening, assessment and intervention principles for key risk factors. As a guiding principle, patients should be shown both ‘what’ to do and ‘how’ to do it.
Fig 3.
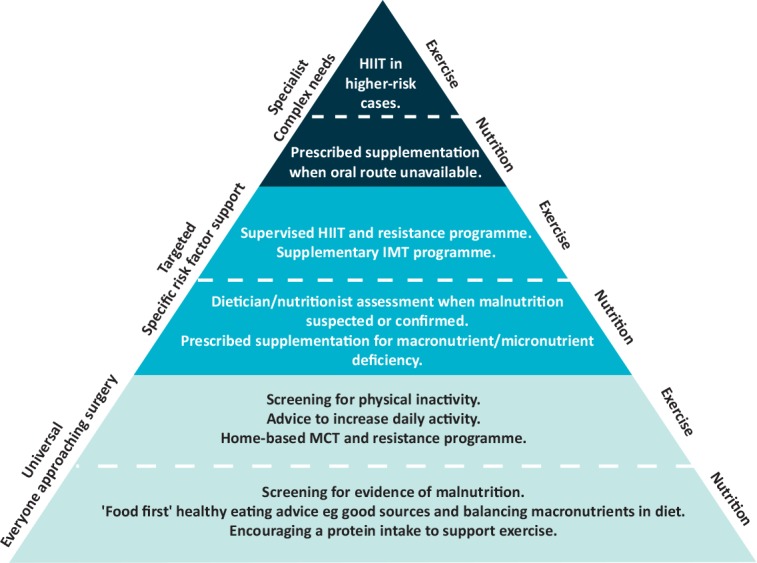
Proposed tiered approach to prehabilitation intervention (nutritional support and exercise used as examples).16 To balance access to prehabilitation against resource, a graded approach to risk factor prehabilitation has been proposed recognising varying individual need. Simple screening and initial advice and instructions should be provided to all patients (universal) available from the wider perioperative team, with escalating degree of intervention, supervision and involvement of more specialist team members (targeted) up to higher-risk patients and those requiring intensive preoperative risk factor support (specialist). HIIT = High-intensity interval training; IMT = inspiratory muscle training; MCT = moderate continuous training.
Table 1.
Overview of risk factor prehabilitation strategies. Screening tools can be employed by multiple clinicians at the earliest opportunity in the preoperative pathway. Further assessment may need to be conducted by specialist healthcare professionals such as a dietician or nutritionist. Prehabilitation interventions should follow similar key principles aiming to achieve meaningful risk factor modification in the available time before surgery.
| Risk factor | Screening (all patients) | Assessment (at risk patients) | Intervention principles | Prehabilitation goals |
|---|---|---|---|---|
| Physical activity | Assess against chief medical officer recommendations for healthy adults:
150 minutes moderate intensity exercise per week or 75 minutes vigorous intensity exercise per week plus muscle strengthening exercise on 2 or more days per week. Patients failing to meet one or both criteria should be offered exercise prehabilitation. |
Objective assessment of physical fitness eg
cardiopulmonary exercise test 6 minute walk test incremental shuttle walk test. |
Combined aerobic and resistance training programme.
Prescribed based on objective fitness assessment. Monitored and modified to account for improvements in fitness. |
Improve aerobic capacity
Develop lean muscle mass |
| Inspiratory muscle training | ARISCAT score.
Consider IMT in ‘intermediate-’ and ‘high-’ risk patients. |
n/a | Structured IMT programme. | Develop muscles of respiration and reduce risk of perioperative pulmonary complications. |
| Smoking | Establish smoking status.
All smokers should be offered cessation support. |
Support access to cessation services for assessment.
Fagerström score used to titrate nicotine therapy. |
Gold-standard cessation programme (combines counselling and nicotine replacement therapy). | Preoperative cessation. |
| Alcohol | Establish weekly intake in units.
Patients with a ‘hazardous’ intake (>14 units per week) should undergo further assessment. |
AUDIT/AUDIT-C questionnaires in those with higher intakes. | Patients with features of dependence will require input from specialist alcohol services.
Those with ‘hazardous’ intakes may respond to the ‘brief alcohol intervention’. |
Modify intake to non-hazardous levels. |
| Nutrition | MUST (Can be adapted for preoperative setting). 39 | Dietician/nutritionist assessment. | Identify macro- and micronutrient deficiencies (ensure total protein intake 1.5–2.0 g/kg daily).
‘Food first’ approach to correction. Consider protein supplementation following exercise training sessions. |
Correct preoperative malnutrition.
Support exercise training. |
| Psychological factors | HADS | Assessment for poorly controlled depression and anxiety and low self-efficacy to engage with prehabilitation. | Build self-efficacy through other risk factor interventions.
Education programmes. Specialist input for psychological intervention. |
Improve control of anxiety and depression.
Develop self-efficacy for prehabilitation and surgery. |
ARISCAT = assess respiratory risk in surgical patients in Catalonia; AUDIT/AUDIT-C = alcohol use disorders identification test; HADS = hospital anxiety depression scale; IMT = inspiratory muscle training; MUST = malnutrition universal screening tool; n/a = not applicable.
Physical inactivity and poor fitness
Poor physical fitness predicts adverse perioperative outcome. This is consistent across multiple specialties.17 One-third of surgical populations may be inactive, reflecting rates observed in UK adults widely.18 Objective assessment of functional capacity using cardiopulmonary exercise testing (CPET) for risk stratification of patients and shared decision making is now established in the UK. Specific variables including peak oxygen consumption (VO2 peak), anaerobic threshold (AT) and ventilatory equivalents for carbon dioxide clearance (VE/VCO2) are linked to outcome.19 The surgical stress response elevates tissue and organ demand for oxygen, with aerobically ‘unfit’ patients struggling to meet this, placing them at increased risk for adverse outcome. This may result from general physical deconditioning through inactivity and/or exercise intolerance from specific pathology.20 Advancing age compounds this situation through a decline in aerobic fitness and activity levels.21 Age is similarly associated with reduced lean muscle mass (sarcopaenia), an independent risk factor for adverse outcome. Other factors predisposing to sarcopaenia include inactivity, chronic health conditions and medication effects, ‘sarcopaenic obesity’ presents specific challenges. Sarcopaenia prevents the patient from readily mobilising postoperatively and fully engaging with physiotherapy.22
Physical fitness can be improved within preoperative timeframes (eg 4–6 weeks) using appropriate exercise interventions.23 Programmes should offer combination training to enhance aerobic capacity and alter body composition (increase lean muscle mass). Components should be prescribed, monitored and adjusted based on repeat objective fitness assessment. ‘Moderate continuous training’ involves exercise at sustained intensities usually below AT. High-intensity interval training (HIIT) alternates periods above or around AT with lower intensity periods. High-intensity training may confer advantages including greater, time efficient improvements in aerobic capacity.24 Preoperative exercise is recognised as safe, based on numerous event-free maximal effort CPET tests and trials, including HIIT in patients approaching aortic aneurysm repair.20,25 To date, single-centre randomised controlled trials have demonstrated improved aerobic fitness with reductions in postoperative morbidity and HLOS with several multi-centre studies in progress.26 The cost-effectiveness of preoperative exercise interventions has also been shown.27
Inspiratory muscle training
Preoperative inspiratory muscle training (IMT) is a form of resistance training for the respiratory muscles. A handheld device is used to support a training programme guided by the maximal inspiratory pressure generated by the patient on initial testing. Training has demonstrated reductions in postoperative pulmonary complications (PPCs) in surgical populations.28 Pulmonary complications are a key contributor to the postoperative morbidity burden and consideration should be given to addition of IMT to a mixed resistance and aerobic programme. The assess respiratory risk in surgical patients in Catalonia (ARISCAT) score provides a validated method of assessing perioperative PPC risk.
A clinical guideline encompassing the broader evidence base for preoperative exercise training and IMT has recently been published.39
Smoking
Smoking is an established perioperative risk factor affecting up to 25% of surgical patients.30 The toxic effects on pulmonary, cardiac and immune function render patients less able to meet surgical demands. Rates of multiple complications including postoperative pneumonia, myocardial events and failed wound are substantially increased.30,31 Smoking status should be established in all patients. National guidance has underlined the importance of preoperative cessation.32 Of concern, awareness of the perioperative impact of smoking among surgical patients is poor. Surgical patients may be less motivated and confident in quitting preoperatively compared to other lifestyle risk factors.13 Encouragingly, the preoperative setting remains an opportune moment to achieve cessation.33 Measurable reductions in postoperative complications require 4–6 weeks preoperative cessation.34 There is no apparent harm from initiating cessation efforts closer to surgery than this.34 Given that measurable physiological benefits occur within minutes of the last cigarette, all smokers should be supported to quit preoperatively using a combination of counselling and titrated nicotine replacement therapy, ideally via access to a cessation service. No evidence exists surrounding e-cigarette use (‘vaping’) perioperatively.
Alcohol
Alcohol appears to exacerbate the neuroendocrine response to surgery leading to an established dose–response relationship with perioperative complications beyond two units daily. Hazardous alcohol consumption may affect up to 23% of surgical patients.35 Patients with manifest features of alcohol dependence and organ dysfunction require specialist preoperative support.36 Patients may drink ‘hazardously’ (above recommended levels of 14 units weekly), elevating surgical risk without any features of dependence or organ dysfunction. Weekly unitary intake should therefore be established in all patients. Reducing consumption to within recommended limits reduces incidence of postoperative complications.37 The ‘brief alcohol intervention’ deliverable by a wide range of professionals appears an effective route to achieve this.37
Nutrition
Preoperative nutritional support is challenging. Malnutrition is a key perioperative risk factor severely undermining recovery. Major surgery induces a profound catabolic state. Patients lacking reserves to manage this then experience significantly poorer outcomes. Malnutrition may involve macronutrient (carbohydrate, protein and fat) deficiency (malnourished malnutrition) or excess (obesity).38 This may be accompanied by micronutrient deficiency and sarcopaenia. Malnutrition screening should be considered in all patients approaching major surgery. The malnutrition universal screening tool (MUST) can be adapted for preoperative use.38 While preoperative healthy eating advice can be provided to all patients, specific assessment and support should be under the supervision of a dietician or nutritionist, a ‘food first’ approach is preferred which may be difficult in the context of swallowing difficulties. The aims of support should be correction of preoperative malnutrition, ensuring sufficient daily protein intake (1.5–2.0 g/kg daily) and support of concurrent exercise training in altering body composition.39
Psychological support
Psychological preparation is an emerging area of prehabilitation practice. A number of psychological traits have now been linked to postoperative outcomes.40 Influential positive and adverse traits have been highlighted relating to mood, attitude and personality.41 Adverse mood states, such as depression and anxiety, alongside attitudinal factors may present targets for preoperative psychological support. An optimal perioperative screening tool is yet to emerge, but several are available including the hospital anxiety and depression score (HADS). Evidence for the impact of preoperative interventions to address these factors is limited, however, positive effects have been demonstrated resulting from preoperative educational interventions, relaxation techniques and hypnosis.42 Successful intervention across the other risk factors may also influence adverse traits.
Prehabilitation for patients with cancer
Patients approaching major cancer surgery face particular challenges. All of the risk behaviours discussed including inactivity, poor diet, smoking and alcohol contribute to carcinogenesis. Surgery remains a key intervention for solid-organ malignancies. Preoperatively, the diagnosis, disease process and therapeutic interventions take a toll upon physical and mental health.16 Neoadjuvant chemoradiotherapy specifically reduces physical fitness potentially transitioning a patient from lower to higher risk.43 Short preoperative timeframes available compound this problem. However, fitness improvements can be made in as little as 2 weeks.44 Recognition of the clear challenges and potential benefits of prehabilitation is detailed in recent national guidance.16
Delivering prehabilitation in practice
At the time of writing, several successful multimodal prehabilitation programmes are underway in the UK and internationally, demonstrating successful patient engagement, adherence and risk factor modification. A number of principles have underpinned the success of these programmes, alongside learning from the established, and the National Institute for Health and Care Excellence recommended, interventions of cardiac rehabilitation and pulmonary rehabilitation.
Cardiac and pulmonary rehabilitation
Strong parallels exist between individuals undergoing prehabilitation and rehabilitation in terms of age, comorbidity profile and the programmes offered. Rehabilitation patients are supported in simultaneous multimodal behaviour change including exercise and activity, smoking and psychological support. Patients attend two to three weekly sessions, structured around a supervised exercise programme. Cardiac rehabilitation demonstrates cost-effectiveness and significant patient benefits across a range of conditions. These include secondary event prevention, reduced hospital readmission, improvements in cardiorespiratory fitness and HRQOL.45 Similar improvements, particularly in exercise capacity and HRQOL, are seen in patients with chronic obstructive pulmonary disease undergoing pulmonary rehabilitation.46
Pathway mapping
Understanding the patient preoperative journey is an essential first step. Preoperative pathways will vary significantly between surgical specialty, underlying condition and local arrangements. Pathway mapping identifies key opportunities to initiate and embed prehabilitation initiatives, defining the time available. Logically, established programmes have sought opportunities to contact patients as early as is feasible following diagnosis or referral.
Cross-sector working and ‘making every contact count’
The majority of surgical pathways will involve primary and secondary care clinicians. The tendency for ‘silo working’ between healthcare sectors does not support prehabilitation intervention and a ‘cross-sector’ approach is mandatory for success. As the clinicians most likely to first identify that an operation may be required, primary care staff are uniquely placed to initiate screening activity and intervention or signpost patients to relevant prehabilitation services supported by secondary care colleagues.
From this ‘point of referral’ to admission, multiple clinician contacts and opportunities exist to initiate and re-enforce prehabilitation initiatives, support and encourage patients in their efforts. This is the ‘making every contact count’ concept.47 The potentially short preoperative timeframes required in some cases make this particularly important. Anecdotal evidence from established services have emphasised the weight patients place upon their surgeon's endorsement; programmes have adopted a ‘surgical champions’ approach to support referrals and engagement.
Involvement of public health is valuable. Clinicians frequently have an overview of available facilities, such as community gyms, charities or smoking cessation services that may have capacity available. The potential longer-term health benefits resulting from lasting preoperative behaviour change align well with broader public health goals. Delivering prehabilitation at existing community venues may be particularly appealing to patients wishing to avoid additional preoperative hospital visits.
Mode of delivery
Most existing prehabilitation programmes, hospital or community-based, are ‘face-to-face’ interventions. It is increasingly recognised that ‘one size may not fit all’. In previous work, one in three surgical patients expressed a preference for ‘home-based’ facilitated self-managed prehabilitation support.13 Service experience has highlighted travel distance and other commitments as key reasons for turning down face-to-face programmes. Home-based alternatives are offered by several programmes but are less researched. Potential advantages include flexibility, cost and the scope to engage a cohort of patients who otherwise would not have prehabilitation access. Equally, concerns exist around patient adherence without close supervision and the absence of peer and staff support to build self-efficacy in the approach to surgery. Digital home-based interventions have been successfully utilised in cardiac rehabilitation including the Activate Your Heart platform. This was successfully tested in patients who turned down face-to-face rehabilitation.48 A systematic review concluded that home-based interventions attained similar outcomes to centre-based models.49 Of note, broader NHS initiatives to more widely utilise digital healthcare interventions and telemedicine recognise growing internet utilisation and confidence among older patients.50
Patient education
Cardiac and pulmonary rehabilitation are underpinned by educational components, aiming to improve patient understanding of their conditions and the importance of lifestyle modification. This is a route to increased patient self-efficacy. The ‘joint school’ concept is now embedded in many orthopaedic pathways. The evolution of this to other major-surgery ‘surgery school’ is now a central component of many prehabilitation programmes. By informing patients and managing expectations of the perioperative period, they are better prepared to engage with prehabilitation initiatives and enhanced recovery pathways.
References
- 1.Abbott TE, Fowler AJ, Dobbs TD, et al. Frequency of surgical treatment and related hospital procedures in the UK: a national ecological study using hospital episode statistics. Br J Anaesth 2017;119:249–57. [DOI] [PubMed] [Google Scholar]
- 2.Helander EM, Webb MP, Menard B, et al. Metabolic and the surgical stress response considerations to improve postoperative recovery. Curr Pain Headache Rep 2019;23:33. [DOI] [PubMed] [Google Scholar]
- 3.Pearse RM, Moreno RP, Bauer P, et al. Mortality after surgery in Europe: a 7-day cohort study. Lancet 2012;380:1059–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hughes MJ, Hackney RJ, Lamb PJ, et al. Prehabilitation before major abdominal surgery: a systematic review and meta-analysis. World J Surg 2019;20:1–8. [DOI] [PubMed] [Google Scholar]
- 5.Perioperative Quality Improvement Programme Annual report 2017–18. London: Royal College of Anaesthetists, 2018. https://pqip.org.uk/pages/ar2018 [Accessed 05 July 2019]. [Google Scholar]
- 6.Kassin MT, Owen RM, Perez SD, et al. Risk factors for 30-day hospital readmission among general surgery patients. J Am Coll Surg 2012;215:322–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lawrence VA, Hazuda HP, Cornell JE, et al. Functional independence after major abdominal surgery in the elderly. J Am Coll Surg 2004;199:762–72. [DOI] [PubMed] [Google Scholar]
- 8.Couwenberg AM, de Beer FS, Intven MP, et al. The impact of postoperative complications on health-related quality of life in older patients with rectal cancer; a prospective cohort study. J Geriatr Oncol 2018;9:102–9. [DOI] [PubMed] [Google Scholar]
- 9.Moonesinghe SR, Harris S, Mythen MG, et al. Survival after postoperative morbidity: a longitudinal observational cohort study. Br J Anaesth 2014;113:977–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Boyd O, Jackson N. Clinical review: How is risk defined in high-risk surgical patient management? Crit Care 2005;9:390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Santa Mina D, Scheede-Bergdahl C, Gillis C, Carli F. Optimization of surgical outcomes with prehabilitation. Appl Physiol Nutr Metab 2015;40:966–9. [DOI] [PubMed] [Google Scholar]
- 12.Flocke SA, Clark E, Antognoli E, et al. Teachable moments for health behavior change and intermediate patient outcomes. Patient Educ Couns 2014;96:43–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.MacDonald S, Yates D, Durrand J, et al. Exploring patient attitudes to behaviour change before surgery to reduce perioperative risk: preferences for short versus long-term behaviour change. Anaesthesia 2019:in press. [DOI] [PubMed] [Google Scholar]
- 14.Levett DZ, Edwards M, Grocott M, et al. Preparing the patient for surgery to improve outcomes. Best Pract Res Clin Anaesthesiol 2016;30:145–7. [DOI] [PubMed] [Google Scholar]
- 15.Prochaska JJ, Spring B, Nigg CR. Multiple health behavior change research: an introduction and overview. Prev Med 2008;46:181–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Macmillan Cancer Support, NIHR Cancer and Nutrition Collaboration, Royal College of Anaesthetists Prehabilitation for people with cancer: Principles and guidance for prehabilitation within the management and support of people with cancer. Macmillan, 2019. www.macmillan.org.uk/assets/prehabilitation-guidance-for-people-with-cancer.pdf [Accessed 08 July 2019]. [Google Scholar]
- 17.Moran J, Wilson F, Guinan E, et al. The preoperative use of field tests of exercise tolerance to predict postoperative outcome in intra-abdominal surgery: a systematic review. J Clin Anesth 2016;35:446–55. [DOI] [PubMed] [Google Scholar]
- 18.Richardson K, Levett DZ, Jack S, Grocott MP. Fit for surgery? Perspectives on preoperative exercise testing and training. Br J Anaesth 2017;119(Suppl 1):i34–i43. [DOI] [PubMed] [Google Scholar]
- 19.Hennis PJ, Meale PM, Grocott MP. Cardiopulmonary exercise testing for the evaluation of perioperative risk in non-cardiopulmonary surgery. Postgrad Med J 2011;87:550–7. [DOI] [PubMed] [Google Scholar]
- 20.Levett DZ, Jack S, Swart M, et al. Perioperative cardiopulmonary exercise testing (CPET): consensus clinical guidelines on indications, organization, conduct, and physiological interpretation. Br J Anaesth 2018;120:484–500. [DOI] [PubMed] [Google Scholar]
- 21.Karavidas A, Lazaros GE, Tsiachris D, Pyrgakis VL. Aging and the cardiovascular system. Hellenic J Cardiol 2010;51:421–7. [PubMed] [Google Scholar]
- 22.Friedman J, Lussiez A, Sullivan J, Wang S, Englesbe M. Implications of sarcopenia in major surgery. Nutr Clin Pract 2015;30:175–9. [DOI] [PubMed] [Google Scholar]
- 23.Kothmann E, Batterham AM, Owen SJ, et al. Effect of short-term exercise training on aerobic fitness in patients with abdominal aortic aneurysms: a pilot study. Br J Anaesth 2009;103:505–10. [DOI] [PubMed] [Google Scholar]
- 24.Weston M, Weston KL, Prentis JM, Snowden CP. High-intensity interval training (HIT) for effective and time-efficient pre-surgical exercise interventions. Perioperative Medicine 2016;5:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Weston M, Batterham AM, Tew GA, et al. Patients awaiting surgical repair for large abdominal aortic aneurysms can exercise at moderate to hard intensities with a low risk of adverse events. Front Physiol 2017;7:684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Barberan-Garcia A, Ubré M, Roca J, et al. Personalised prehabilitation in high-risk patients undergoing elective major abdominal surgery: a randomized blinded controlled trial. Ann Surg 2018;267:50–6. [DOI] [PubMed] [Google Scholar]
- 27.Tew GA, Batterham AM, Colling K, et al. Randomized feasibility trial of high-intensity interval training before elective abdominal aortic aneurysm repair. Br J Surg 2017;104:1791–801. [DOI] [PubMed] [Google Scholar]
- 28.Katsura M, Kuriyama A, Takeshima T, Fukuhara S, Furukawa TA. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev 2015:CD010356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tew GA, Ayyash R, Durrand J, Danjoux GR. Clinical guideline and recommendations on pre-operative exercise training in patients awaiting major non-cardiac surgery. Anaesthesia 2018;73:750–68. [DOI] [PubMed] [Google Scholar]
- 30.Schmid M, Sood A, Campbell L, et al. Impact of smoking on perioperative outcomes after major surgery. Am J Surg 2015;210:221–9. [DOI] [PubMed] [Google Scholar]
- 31.An D, Ayob F, Rajaleelan W, Chung F, Wong J. Preoperative smoking cessation as part of surgical prehabilitation. Can J Anesth 2019;3:1–4. [DOI] [PubMed] [Google Scholar]
- 32.Fauculty of Public Health, Royal College of Surgeons of Edinburgh, Royal College of Anaesthetists, Action on Smoking and Health Joint briefing: Smoking and surgery. London: RCoA, 2018. www.rcoa.ac.uk/sites/default/files/Joint-briefing-Smoking-Surgery.pdf [Accessed 07 July 2019]. [Google Scholar]
- 33.Nayan S, Gupta MK, Strychowsky JE, Sommer DD. Smoking cessation interventions and cessation rates in the oncology population: an updated systematic review and meta-analysis. Otolaryngol Head Neck Surg 2013;149:200–11. [DOI] [PubMed] [Google Scholar]
- 34.Thomsen T, Villebro N, Møller AM. Interventions for preoperative smoking cessation. Cochrane database Syst Rev 2014:CD002294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nath B, Li Y, Carroll JE, et al. Alcohol exposure as a risk factor for adverse outcomes in elective surgery. J Gastrointest Surg 2010;14:1732–41. [DOI] [PubMed] [Google Scholar]
- 36.Eliasen M, Grønkjær M, Skov-Ettrup LS, et al. Preoperative alcohol consumption and postoperative complications: a systematic review and meta-analysis. Ann Surg 2013;258:930–42. [DOI] [PubMed] [Google Scholar]
- 37.Oppedal K, Møller AM, Pedersen B, Tønnesen H. Preoperative alcohol cessation prior to elective surgery. Cochrane Database Syst Rev 2012:CD008343. [DOI] [PubMed] [Google Scholar]
- 38.Gillis C, Wischmeyer PE. Pre-operative nutrition and the elective surgical patient: why, how and what? Anaesthesia 2019;74:27–35. [DOI] [PubMed] [Google Scholar]
- 39.Gillis C, Carli F. Promoting perioperative metabolic and nutritional care. Anesthesiol 2015;123:1455–72. [DOI] [PubMed] [Google Scholar]
- 40.Rosenberger PH, Jokl P, Ickovics J. Psychosocial factors and surgical outcomes: an evidence-based literature review. J Am Acad Orthop Surg 2006;14:397–405. [DOI] [PubMed] [Google Scholar]
- 41.Levett DZ, Grimmett C. Psychological factors, prehabilitation and surgical outcomes: evidence and future directions. Anaesthesia 2019;74:36–42. [DOI] [PubMed] [Google Scholar]
- 42.Powell R, Scott NW, Manyande A, et al. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst Rev 2016:CD008646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Jack S, West MA, Raw D, et al. The effect of neoadjuvant chemotherapy on physical fitness and survival in patients undergoing oesophagogastric cancer surgery. Eur J Surg Oncol 2014;40:1313–20. [DOI] [PubMed] [Google Scholar]
- 44.Faithfull S, Turner L, Poole K, et al. Prehabilitation for adults diagnosed with cancer: a systematic review of long-term physical function, nutrition and patient-reported outcomes. Eur J Cancer Care (Engl) 2019;28:e13023. [DOI] [PubMed] [Google Scholar]
- 45.Anderson LJ, Taylor RS. Cardiac rehabilitation for people with heart disease: an overview of Cochrane systematic reviews. Int J Cardiol 2014;177:348–61. [DOI] [PubMed] [Google Scholar]
- 46.McCarthy B, Casey D, Devane D, et al. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane database Syst Rev 2015:CD003793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.NHS England An implementation guide and toolkit for making every contact count: using every opportunity to achieve health and wellbeing. NHS, 2019. www.england.nhs.uk/wp-content/uploads/2014/06/mecc-guid-booklet.pdf [Accessed 08 July 2019]. [Google Scholar]
- 48.Houchen-Wolloff L, Gardiner N, Devi R, et al. Web-based cardiac REhabilitatioN alternative for those declining or dropping out of conventional rehabilitation: results of the WREN feasibility randomised controlled trial. Open heart 2018;5:e000860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Anderson L, Sharp GA, Norton RJ, et al. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst Rev 2017;6:CD007130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.NHS The Topol review: Preparing the healthcare workforce to deliver the digital future. Health Education; England, 2018. https://topol.hee.nhs.uk [Accessed 08 July 2019]. [Google Scholar]