
Figure 1.
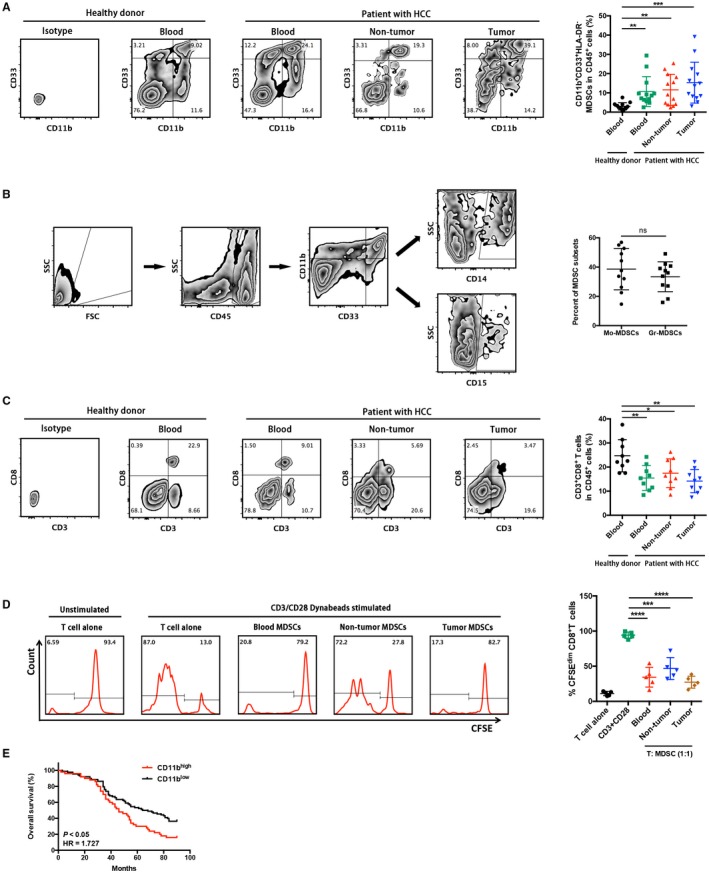
Tumor‐infiltrating CD11b+CD33+HLA‐DR− MDSCs in patients with HCC exert potent autologous CD8+ T‐cell suppression. (A) Representative CD11b+CD33+ MDSC zebra plots are shown in blood, nontumor, and tumor tissues from patients with HCC and healthy controls following a leukocyte gate (CD45+HLA‐DR−). Cells stained by isotype antibody were used as fluorescence baseline control. CD11b+CD33+HLA‐DR− cells were further analyzed and presented in 13 patients with HCC and 13 healthy donors. **P < 0.01, ***P < 0.001. (B) Gating strategies of MDSC subsets in flow cytometry. Similar levels of CD14+ monocytic and CD15+ granulocytic subsets were observed in HCC tissues. (C) Corresponding CD3+CD8+ T‐cell proportions in CD45+ leukocytes were determined. *P < 0.05, **P < 0.01. (D) Autologous T‐cell proliferation assay. The percentage of 5(6)‐carboxyfluorescein succinimidyl ester low population represents the proportion of proliferating CD3+CD8+ T cells. Representative flow‐cytometric data and a statistical diagram are shown. ***P < 0.001, ****P < 0.0001. (E) Kaplan‐Meier overall survival curves of patients with HCC with high or low expression (stratified by median) of CD11b. Abbreviations: CFSE, 5(6)‐carboxyfluorescein succinimidyl ester; FSC, forward scatter; SSC, side scatter.