
Figure 1.
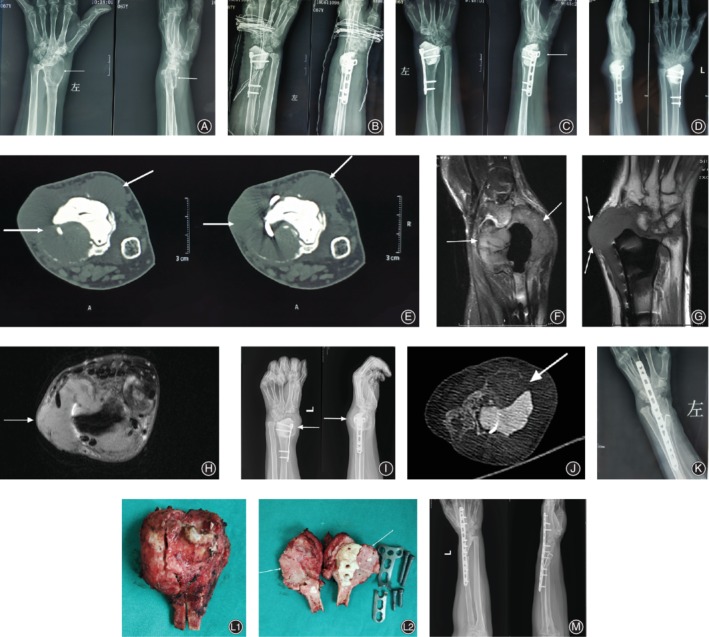
A 67‐year‐old female with a recurrent left distal radius GCTB. (A‐C) Images of the primary curettage surgery in outer hospital. (A) Plain radiograph (before surgery) of a typical GCTB demonstrating a lytic and expansile lesion (arrows) in the distal radius. (B) The immediately postoperative radiographs of the surgery of curettage, cementation and internal fixation. (C) Plain radiograph showing local recurrence (arrows) 2 months after the surgery. 4 months after the primary curettage surgery, the patient was referred to our hospital. (D‐H) Plain radiograph(D), CT (axial E), and MRI (sagittal, coronal, axial F‐H) showing local recurrence of the distal radius with cortical discontinuity and massive soft tissue component (arrows). (I‐J) Plain radiograph (I) and CT (J axial) following denosumab treatment demonstrating significant shrinkage of tumor size, and calcified sclerotic rim(arrows) and central sclerosis. (K) Immediately postoperative radiographs following a resection procedure with allograft bone reconstruction and wrist arthrodesis. (L) Resection material: 1. cross section of the resected tumor. 2. the new formed tissue after denosumab treatment (arrows). (M) Plain radiograph showing no signs of local recurrence 12months after the 2nd surgery.