
Figure 1.
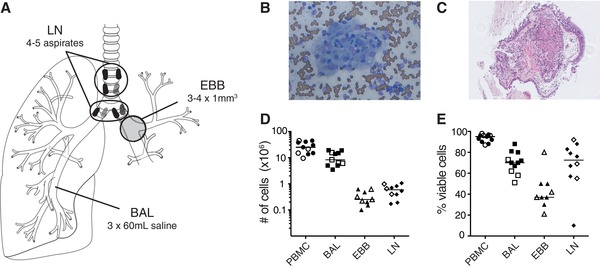
Sufficient numbers of viable cells recovered from four anatomical locations from the same sarcoidosis patient. (A) Bronchoscopy was performed on seven non‐LS and four LS sarcoidosis patients to obtain endobronchial biopsies (EBBs) from the main bronchial divisions of one lung, while bronchoalveolar lavage (BAL) was performed to retrieve aspirates from the lower airways from the contralateral side to avoid contamination due to bleeding. Subsequently, lung‐draining lymph node (LLN) aspirates were collected using endobronchial ultrasound‐guided transbronchial needle aspiration (EBUS‐TBNA) sampling the mediastinal and hilar lymph nodes. Patients provided blood samples prior to the bronchoscopy and peripheral blood mononuclear cells (PBMCs) were isolated. All samples were processed immediately after the bronchoscopy. Representative image of non‐necrotizing granuloma in (B) LLNs (Diff‐Quik staining) and (C) EBBs (hematoxylin and eosin staining) of a sarcoidosis patient. (D) Total number and (E) percentage of viable cells in single cell suspensions of PBMC (circle), BAL (square), EBBs (triangle) and LLNs (diamond) in non‐LS (filled symbols) and LS sarcoidosis patients (open symbols) were determined using Trypan Blue exclusion stain and manual counting with a Bürker counting chamber under a light microscope. One aspirate from the LLN with reduced viability (<10%) was excluded from further analysis. Lines indicate median values. n = 11 for all samples except LLNs with n = 10