

Abstract
Background and aim
Polychromatic light is actively used in medicine. However, its oncological safety and effect against cytotoxic therapy remains poorly studied. Multiple myeloma (MM) develops in the bone marrow and therefore malignant plasma cells are inaccessible to direct exposure to light. The aim of our work was to study the influence of polychromatic visible and infra-red light (pVIS + pIR) on growth and sensitivity of the myeloma cells to the cytotoxic effect of drug bortezomib (BTZ) through systemic mechanism.
Materials and methods
We explored the effect of volunteers blood sera after their 4-daily irradiations with pVIS + pIR light (480–3400 nm) on growth and viability of the human myeloma RPMI 8226 cells in the presence of BTZ at its application in 2 modes: short-term (1 h, 300 nM) and long-term ( 96 h, 5 nM). Viability and proliferative activity of cells was evaluated by MTT assay.
Results
It was found that photomodified blood sera delayed growth of myeloma RPMI 8226 cells (by 25 % in 48 h and 23 % in 96 h) but had no effect on spontaneous and mitogen-induced proliferation of autologous peripheral blood T- and B-lymphocytes. We also revealed that pVIS + pIR did not change RPMI 8226 cells sensitivity to BTZ.
Conclusion
The results suggest the systemic mechanism of polychromatic light and argue in favor of its oncological safety during/after BTZ therapy of MM patients without effect on the drug cytotoxicity.
Keywords: multiple myeloma, visible light, cell proliferation, cytotoxicity, Bortezomib
Introduction
Low intensity phototherapy, more recently termed photobiomodulation (PBM) 1), has been widely used in medicine since the end of 1960s 2). For the last 20 years, along with monochromatic or narrow band visible (VIS) and near infrared (IR) light of lasers and light-emitting diodes, polychromatic visible light combined with infrared (pVIS+pIR, 480–3400 nm) has been also actively applied to modulate immune and inflammatory processes, stimulate wound healing and increase blood microcirculation 3–7). Due to their properties, both monochromatic and polychromatic lights have been used in clinical oncology to reduce the frequency and severity of negative side effects of conservative treatment methods being applied. Thus, PBM is an effective tool for the prevention and treatment of broad range of complications (mucositis, dermatitis, dysphagia and blood microcirculation disorders) developed in patients in response to chemotherapy and radiotherapy. 7–10)
Despite the positive experience of using PBM in the field of oncology, the question of its safety for cancer patients remains undetermined. Less is known about antitumor activity of PBM. The effect of PBM on tumor cells is actively studied in vitro and in vivo and gives conflicting results depending on the parameters of the model systems being used. 2) Oncological safety of pVIS + pIR radiation was shown in our experiments on isolated tumor cells, laboratory animals with tumors and during post-operative immuno-rehabilitation of patients with breast cancer. 7, 11–13) Phototherapy approaches, as well as the problem of the interaction of light therapy and conservative approaches in the treatment of cancer patients need additional researches. There is only isolated data proving that PBM can enhance certain types of antitumor therapy, in particular, photodynamic 14) and radiation therapy. 15–16) To study the effect of light on the growth of tumor cells, direct local exposure of light to damaged tissues is predominantly used, whereas the value of the systemic mechanisms of light action through the circulatory and lymphatic systems is far from being fully estimated by experts. 17–18) Data showing tumor growth reduction obtained in vivo study is potentially connected to the PBM-activated innate immunity. 13, 19–20)
It is worth emphasizing that in medical practice when using phototherapeutic devices, only cells of the irradiated area are exposed to direct (local) effect of light, while cells of the tissues of internal organs, including tumor cells, experience action mediated by systemic mechanism through circulation systems. We believe that the transcutaneously photomodified blood makes a major contribution to the systemic mechanism of therapeutic effects of pVIS + pIR, which is the main (if not the only) case of those organs and tissues which are not accessible and exposed to the direct light. 21–22) Such tissues include, in particular, the hematopoietic tissue of the bone marrow and its malignant derivative - multiple myeloma (MM). MM is a widely spread and incurable hematologic malignancy with a median survival of 3 to 5 years. Bortezomib (Velcade®) is the first FDA approved proteasome inhibitor for clinical use in the treatment of MM. 23)
The goal of this work was to study the systemic mechanisms of influence of pVIS + pIR light (480–3400 nm, 40 mW/cm2), on the myeloma cells, including the action of the antitumor drug Bortezomib. For ethical reasons, we did not expose patients with MM to the phototherapeutic course. Therefore, the objectives of this study were to investigate the effect of blood sera of 10 healthy volunteers after daily (course) irradiations of their body surface on 1) viability and proliferation of human MM cells (line RPMI 8226) in vitro 2) effectiveness of the inhibitory effect on these cells of the drug Bortezomib (BTZ) when applied in 2 modes: under conditions of short-term exposure (1 h, IC50 = 300 nM) and under conditions of prolonged exposure (96 h, IC50 = 5 nM). Both modes simulate the clinical protocol of drug administration: intravenous and subcutaneous, respectively. Since human MM cells are by origin B-lymphocytes, we also studied the effect of blood sera of irradiated volunteers on the proliferation of healthy human lymphocytes of autologous blood.
2. Material and methods
2. 1. Volunteers and irradiation procedure
Practically healthy 25–50 -years old volunteers (n = 10) were irradiated for 4 days (low part of the back, 15 cm × 15 cm) using Bioptron-2 phototherapeutic device (Bioptron- AG, Switzerland, 480–3400 nm, power density -40 mW/cm2 for 5 min, dose- 12 J/cm2). This dose is the most often used in clinical and experimental settings. Polychromatic light of Bioptron apparatus simulates the spectral content of the terrestrial solar radiation and its power density in summer day in Central Europe without its minor spectral component – UV rays. However it has one peculiarity of laser light: high degree of linear polarization (95%). The study design was approved by the Ethical Committee of Institute of Cytology of Russian Academy of Sciences. The blood samples for the study were drawn twice: before light therapy (Pre-irrad) and after 4-daily irradiations of volunteers (Post-irrad). After clotting of blood, serum was separated by centrifugation for 10 min at 3000 g. Serum samples were frozen at -80°C for subsequent analysis.
2. 2. Cell Culture
The human myeloma cell line RPMI 8226 was obtained from Russian Cell Culture Collection (St-Petersburg, Institute of Cytology, Russian Academy of Science). Cells were cultivated in RPMI 1640 medium supplemented with 10% FBS, 2-mM L-glutamine, penicillin/streptomycine (100 µg/ml, 100 U/ml).
In experiments 5% individual volunteer's sera were used instead of FBS, serum concentration has been established in preliminary experiments.
2. 3. Evaluation of viability and proliferative activity of RPMI 8226 cells
Total index of viability and proliferative activity of cells was used. It was evaluated by calorimetric MTT (mitochondrial dye 3-(4,5-dimethylthiszol-2yl)-2,4 diphenyltetrazolium bromide) conversion assay. In brief, RPMI 8226 cells were seeded in 96-well microplate at a density of 5–8 × 104 cells/well, which allowed to register simultaneously both the logarithmic growth phase of myeloma cells and the cytotoxic effect of the antitumor drug BTZ. BTZ (® Velcade, Pierre Fabre, Medicament Production, France) was dissolved in dimethyl sulfoxide (DMSO) at appropriate concentration and added to culture medium. Final DMSO concentration was < 0,01% that did not affect cell viability. Two modes of cells exposure to BTZ were used: 1) short-term 1 h exposure (inhibitory concentration IC50 = 300 nM); 2) long-term 96 h exposure (IC50 = 5 nM). Drug concentration was chosen according to literature data 24) and our preliminary data (not shown). RPMI 8226 cells were incubated with or without BTZ for indicated time in the presence of volunteer's blood sera. Then culture media with BTZ was removed and replaced by drug-free media. 10% MTT dye (5 mg/ml (Sigma, USA) was added to each well for 3 h. Plates were then centrifuged and each well aspirated. The formazan crystals were solubilized with 50 µl DMSO and the solution optical density was measured at 540 nm on automated microtiter plate reader. Viable cell number was assessed at 24 h, 48 h, and 96 h and expressed as a percentage of the value of the initial cell level.
2. 4. Proliferative activity of lymphocytes
The proliferative response of peripheral blood lymphocytes in whole blood was evaluated by flow cytometry. Human peripheral blood lymphocytes were cultivated in wells of microtiter plates. After incubation for 3 days with phytohaemagglutinin (PHA, 15 µg/ml, Sigma) or with pokeweed mitogen (PWM, 15 µg/ml, Sigma) the cells were treated by Triton X-100 (1%, Sigma) and RNAse (1%, Sigma) and stained with ethidium bromide (1%, Sigma). The level of proliferative activity was calculated as the sum of cells in the synthetic, post-synthetic phases and in mitosis (cells in the stages S + G2/M) and expressed in percentage.
2. 5. Statistical analysis
Statistical processing of results was performed using Statistica. v10 Software. Data are presented as mean+ standard error of mean (M ± SEM). Each experiment with individual sera was performed in triplicate or more, and repeated twice. Statistical analysis was performed using parametric methods for matched pairs (Student t-test).
The results were considered as significant at p ≤0.05.
3. Results
3. 1. Influence of blood sera of volunteers irradiated with pVIS + pIR light on the proliferation of human myeloma RPMI 8226 cells.
First, we compared the influence of blood sera of volunteers before and after their percutaneous irradiation with pVIS + pIR light on the proliferation of RPMI 8226 cells. The results are shown in Figure 1. It can be seen that after 24 h of cultivation with blood sera of volunteers prior to irradiation (Pre-irrad), the cell amount increased on average to 137 ± 8 % of their initial level (100 %). The total number of myeloma cells continued to increase up to 198 ± 5.4 % and 206 ± 12.8 %, at 48 h and 96 h, respectively. The growth curve indicated a logarithmic character of the cell growth for the 24 h-48 h with reaching the plateau by 96 h (Figure 1). At the same time, the cultivation of cells in the presence of blood sera of volunteers after their 4-daily percutaneous irradiations with pVIS + pIR light (Post-irrad) led to the reduction in the cell growth in all test points (by 13 %, 25 % and 23 %, respectively), this effect was statistically significant at 48 h and 96 h (p < 0.05 and p < 0.01, respectively, Figure 1).
Figure 1:
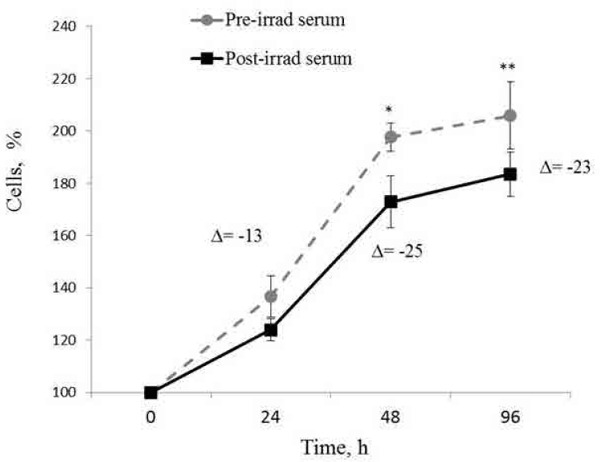
Dynamics of RPMI 8226 cells growth with blood sera of volunteers before (Pre-irrad) and after (Post-irrad) their 4-daily percutaneous irradiations with pVIS + pIR light. The percentage of viable cells was evaluated using MTT assay. Results are shown as a percent of initial cells amount. Data represent mean+SEM. Δ - difference between cells cultivated with Pre -irrad and Post -irrad serum. The differences are statistically significant at *p < 0.05, **p < 0.01.
3. 2. Influence of blood sera of volunteers irradiated with pVIS + pIR light on the proliferation of autologous peripheral blood lymphocytes.
To determine the effect of blood sera of irradiated volunteers on the proliferative activity of healthy human lymphocytes, the level of spontaneous proliferation of T- and B- lymphocytes and their proliferative response in the presence of the corresponding mitogens (PHA and PWM) have been investigated. Autologous blood of volunteers was used. The level of spontaneous lymphocyte proliferation in the presence of variants of sera (Pre-irrad or Post-irrad) remained unchanged as was the proliferative response of T-and B-lymphocytes to mitogens (Table 1). It is significant that there was not even a tendency to decrease proliferation of normal lymphocytes, unlike the transformed ones (RPMI 8226).
Table 1: Proliferation of healthy human lymphocytes cultured with autologous sera before (Pre-irrad) and after (Post- irrad) 4-daily exposures of volunteers to pVIS + pIR light.
| The number of cells in the synthetic, post-synthetic phase of the cycle and in mitosis (S+ G2/M), % of the total number of cells, Mean+ SEM | ||
|---|---|---|
| Pre-irrad serum | Post-irrad serum | |
| Spontaneous proliferation (Norm 0,5–1,5%) |
0,9 ± 0,4 | 1,1 ± 0,8 |
| PHA-induced T-lymphocytes proliferation (Norm 3–10%) |
6,9 ± 3,9 | 7,5 ± 4,4 |
| PWM-induced B-lymphocytes proliferation (Norm 13–60%) |
32,5 ± 15,7 | 32,9 ± 14,3 |
3. 3. Influence of blood sera of volunteers irradiated with pVIS + pIR light on viability and proliferation of human myeloma cells RPMI 8226 after a short-term (1 h) BTZ treatment (300nM).
We next investigated the viability of myeloma RPMI 8226 cells after 1 h short-treatment with BTZ (300 nM). As can be seen in Figure 2, after 24 h of cultivation viability of RPMI 822 cells decreased sharply in comparison to control cells without BTZ (89 % vs. 137 %) irrespective of irradiation factor . The cell viability continued to decrease in 48h after BTZ treatment, indicating the long-acting drug cytotoxicity. At this time there was difference in cell viability between cells incubated with Pre-irrad or Postirad sera of volunteers. The RPMI 8226 cells viability in cultures containing the blood sera of volunteers prior to exposure to pVIS + pIR was higher than in cultures with sera after exposure to light (48 h: Δ = −15 %, p ≤ 0.01). The next two days after the toxic effect of BTZ, the expansion of the surviving cells was gradually restored in both variants, but the difference in cell viability between the serum variants (Post-irrad versus Pre-irrad) significantly increased (96 h: Δ = −26%, p ≤ 0.01).
Figure 2:
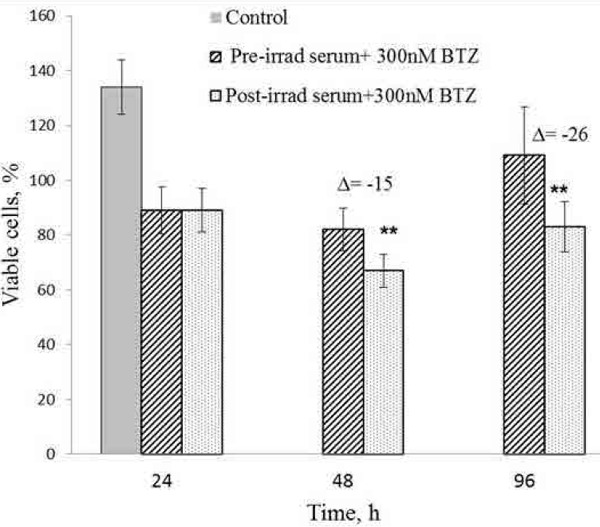
I nfluence of blood sera of volunteers before (Pre-irrad) and after ( Post-irrad) their 4- daily percutaneous irradiations with pVIS + pIR light on viability and growth of human myeloma RPMI 8226 cells treated for short- term (1h) with 300nM BTZ. The percentage of viable cells was evaluated using MTT assay. Results are shown as a percent of initial cells amount. Control -serum w/o irradiation and w/o BTZ. Data represent mean+SEM. Δ - difference between cells cultivated with Post-irrad and Pre-irrad sera. The differences are statistically significant at **p < 0,01
3. 4. Influence of blood sera of volunteers irradiated with pVIS + pIR light on viability and proliferation of human MM cells RPMI 8226 after long- term (96h) BTZ treatment (5 nM)
In case of long-term exposure to the antitumor drug BTZ, RPMI 8226 cells were incubated for 96 h in the medium supplemented with 5% sera of volunteers in the presence of BTZ (5 nM). At the first 24 h of BTZ treatment, cell viability was similar to viability in short- term treatment mode: it decreased up to the same level: 89 % and 91 % (Figure 2 and Figure 3). At 24 h cell viability decreased sharply compared to the control without BTZ and without irradiation (89 % versus 148 %) and continued to decrease at 48h (65%) and 96 h (29%) (Figure 3). There was no difference in the BTZ toxicity between cell cultures supplemented with Pre-irrad or Post-irrad sera of volunteers. The amount of viable cells for Pre-irrad and Post-irrad sera at 24 h was 91 % and 87 % , at 48 h -56 % and 55 %, at 96 h-29 % and 28 %, respectively. This result indicated that there was no influence of the irradiation factor on the effectiveness of the BTZ cellular toxicity.
Figure 3:
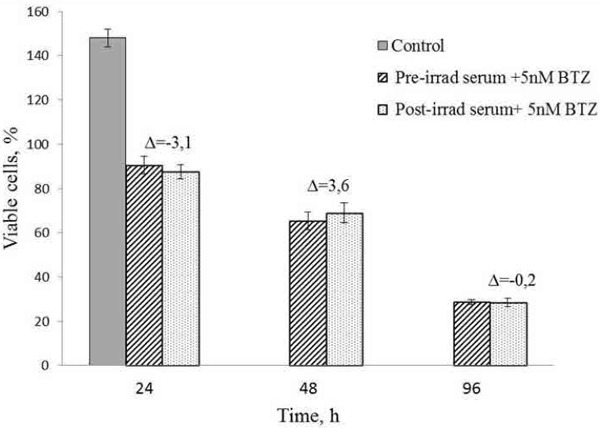
Influence of blood sera of volunteers before (Pre-irrad) and after (Post-irrad) their 4- daily percutaneous irradiations with pVIS + pIR light on viability and growth of human myeloma RPMI 8226 cells treated for long-term (96h) with 5nM BTZ. The percentage of viable cells was evaluated using MTT assay. Results are shown as a percent of initial cells amount. Control -serum w/o irradiation and w/o BTZ. Data represent mean+SEM. No statistically significant changes were observed.
Discussion
In the present work under experimental conditions we studied the influence of pVIS + pIR light on MM cells through systemic mechanism that supposed involvement of the blood circulation system. For this purpose we investigated how the sera of volunteers after their percutaneous exposures to pVIS + pIR light affected the viability and proliferation of human myeloma RPMI 8226 cells under influence of proteasome inhibitor BTZ. These are the results of preliminary research conducted on ten healthy volunteers. In further studies the usage of in vitro of photomodified blood from MM patients will be preferred.
Sera isolated from the blood of volunteers after irradiation of a small area of their body with pVIS + pIR light within 4 days delayed the proliferation of human MM cells but did not affect spontaneous and mitogen-induced proliferation of normal human blood lymphocytes. Available scientific data on cellular proliferative potential of irradiation led to a number of speculative conclusions that irradiation can also stimulate the growth of tumor cells and promote tumor progression. As summarized in the review of Zecha, 2) the effect of light on cell proliferation significantly depends on the parameters of irradiation (wavelength, power density), and also on the cell type. The light effect can be both stimulating 25–27) and inhibitory 28–31) or without effects. 12, 32–33)
The majority of studies on tumor cell irradiation are carried out on models with application of direct in vitro cell irradiation. Our previous investigations of anti-inflammatory, immunomodulating and wound-healing effects of pVIS + pIR light have shown that when a small area of the body surface was irradiated, the light-induced changes were developed within a few minutes in all types of blood cells and in many plasma components of the entire circulating blood volume. 3–4, 21–22) This is due to the fact that when penetrating into the skin the dense network of subepidermal micro-vessels where blood moves at a low speed and can receive an effective dose of light energy, pVIS + pIR radiation causes photomodification of blood. The use of the serum of the irradiated volunteers in cell cultivation allows us to study the systemic effect of percutaneous irradiation on the cellular model in vitro. This approach was successfully applied for cultivation of different normal and tumor cells. 11, 34)
Multiple myeloma is a B-cell malignancy which has features specific to B- lymphocytes. The appearance in the serum of factors inhibiting the proliferation of myeloma cells could have a similar effect on the behavior of normal lymphocytes, which would negatively affect the antitumor immunity. Apparently, the inhibitory effect of light-mediated factors is realized through other receptors / signaling molecules of transformed cells and is not associated with the ability of normal lymphocytes to mitogen- induced activation.
As it was previously published in scientific sources, normal cells and transformed cells may respond to phototherapy differently. It was observed 16) that phototherapy differently affected normal lymphoblasts and leukemia cells making the latter more sensitive to subsequent radiotherapy. Unlike normal fibroblasts and epithelial cells, application of low-level laser therapy in carcinoma cells led to apoptosis. 35)
In present work we found that pVIS + pIR irradiation did not directly affect the myeloma cell sensitivity to toxic action of BTZ. Proteasome inhibitors show antitumor action against myeloma cells and are considered to be widely applied for the treatment of MM. Proteasome dysfunction leads to an apoptosis of actively proliferating cells. BTZ is highly toxic to all myeloma cell lines, but sensitivity to chemotherapy in each cell line is different and depends on the time of its exposure and concentration. For the myeloma line RPMI 8226 there is evidence that the inhibitory concentration of IC50 is 5.9 nM for a continuous 48 h exposure and 208 nM for a short-term 1-h exposure. 24) According to our data, the concentration of IC50 for a long-term (up to 96 h) and short-term (1h) exposure was very similar to what has been mentioned above (5 nM and 300 nM, respectively). The mode of short-term treatment of BTZ reproduces conditions for intravenous clinical administration of the drug, at which a short-term high BTZ concentration in the blood is reached with its further decrease within an hour. In contrast, the long-term effect of the drug with its low concentration simulates its subcutaneous bolus injection. 36, 37)
Toxic effect of specified drug BTZ on myeloma cells is certainly much stronger in comparison to the light influence. Therefore, the systemic effect of light manifests itself only in the absence of BTZ. Because of this, we could observe the RPMI 8226 cell growth delay only after cultivation without BTZ.
Development of systemic effects of light is connected to the transcutaneous photomodification of blood and changes in the properties and functions of its components in the entire blood volume. The cytokine system is possible link providing this effect. Multiple myeloma is an example of an imbalance in the cytokine system with a changed level of both inflammatory and anti-inflammatory cytokines. However, the progression of MM appears to be determined not directly by inflammatory phenotypes, but rather by the balance between the proliferative - antiproliferative potential of the cytokines. 38) The level of some cytokines involved in the pathogenesis of MM can be regulated by the influence of light. 39) It was shown earlier in our studies, that irradiation of a small body surface area (15 × 15 cm) with pVIS + pIR light at a dose of 12 J/cm2, which was used in this study also, caused modulation of the cytokine network: a decrease in blood serum the inflammatory cytokine level (IL-6, TNF-α, IL12, IFN-γ) and an increase the anti-inflammatory cytokine amount (IL10, TGF-β) 4). Light therapy of patients with seasonal affective disorder significantly reduced inflammatory cytokines IL-1β, TNF α, IFN-γ production and increased anti-iflammatory cytokine IL-10 release in blood. 40) The effect of 780 nm light on the skin cells can regulate the level of IL-2 and IL-6 secretion. 41–42) The inflammatory cytokine IL-6 is the main factor of plasma cells differentiation and proliferation and also survival of myeloma cells. For MM patients IL-6 also becomes a major morbidity factor. 38) The possible lowering of the cytokine concentration with protumor activity in the blood after transcutaneous action of pVIS + pIR light could improve the condition and prognosis for patients with MM. Taking into account the obtained experimental data, the use of Bioptron − based phototherapy during or after BTZ therapy can contribute to effectiveness of treatment of MM patients. Moreover, the effect of pVIS + pIR light on the proliferative activity of plasma cells has an indirect effect and can be associated with mechanisms mediated by the production of cytokines. This effect can be achieved by inhibiting the proliferation of myeloma cells without lowering the sensitivity of tumor cells to chemotherapy. It should be noted that transcutaneous irradiation with pVIS + pIR light did not have a suppressive effect on the proliferation of immunocompetent cells of healthy volunteers, highly likely this effect will be reproduced on patients with MM. With the account of the results of this study an assumption can be made, that the involvement of Bioptron phototherapy could enhance response of MM patients to BTZ treatment. However, more studies are necessary to confirm the effectiveness and safety of the pVIS + pIR light therapy for oncological patients.
Acknowledgments
This work was supported by The Nikiforov Russian Center of Emergency and Radiation Medicine (St-Peterburg, Russia). We are very grateful to Prof. Sergei S. Aleksanin for providing support of this research
References
- 1: WALT/NAALT Photobiomodulation: mainstream medicine and beyond. September 9-2 2014; WALT Biennial Congress and NAALT Annual Conference; Arlington Virginia USA. [Google Scholar]
- 2: Zecha JAEM, Raber-Durlacher JE, Nair RG, Epstein JB, Sonis ST, Elad S, et al. Low level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: part 1: mechanisms of action, dosimetric, and safety considerations. Support Care Cancer, 2016; 24(6):2781-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3: Zhevago NA, Samoilova KA, Obolenskaya KD. The regulatory effect of polychromatic (visible and infrared) light on human humoral immunity. Photochem Photobiol Sci, 2004; 3(1):102-8. [DOI] [PubMed] [Google Scholar]
- 4: Zhevago NA, Samoilova KA. Pro- and Anti-inflammatory Cytokine Content in Human Peripheral Blood after Its Transcutaneous ( in Vivo ) and Direct ( in Vitro ) Irradiation with Polychromatic Visible and Infrared Light. Photomed Laser Surg, 2006; 24(2):129-39. [DOI] [PubMed] [Google Scholar]
- 5: Samoilova KA, Zhevago NA, Menshutina MA, Grigorieva NB. Role of Nitric Oxide in the Visible Light-Induced Rapid Increase of Human Skin Microcirculation at the Local and Systemic Level: I. Diabetic Patients. Photomed Laser Surg, 2008; 26(5):433-42. [DOI] [PubMed] [Google Scholar]
- 6: Samoilova KA, Zhevago NA, Petrishchev NN, Zimin AA. Role of Nitric Oxide in the Visible Light-Induced Rapid Increase of Human Skin Microcirculation at the Local and Systemic Levels: II. Healthy Volunteers. Photomed Laser Surg, 2008; 26(5):443-9. [DOI] [PubMed] [Google Scholar]
- 7: Zhevago NA, Zimin AA, Glazanova T V., Davydova NI, Bychkova N V., Chubukina Z V., et al. Polychromatic light (480- 3400nm) similar to the terrestrial solar spectrum without its UV component in post-surgical immunorehabilitation of breast cancer patients. J Photochem Photobiol B Biol, 2017; 166:44-51. [DOI] [PubMed] [Google Scholar]
- 8: Bensadoun R-J, Nair RG. Low-level laser therapy in the prevention and treatment of cancer therapy-induced mucositis: 2012 state of the art based on literature review and meta- analysis. Curr Opin Oncol, 2012; 24(4):363-70. [DOI] [PubMed] [Google Scholar]
- 9: Zharinov G.M., Zimin A.A., Samoilova K.A., Neklasova N.Yu., Volodina L.A., Ovsyannikov V.A. Late radiation lesions of urinary bladder and rectum in patients with prostate cancer after external radiation therapy and phototherapy with low power near infrared laser. Laser Therapy, 2010; 19(2):89-95. [Google Scholar]
- 10: Zecha JAEM, Raber-Durlacher JE, Nair RG, Epstein JB, Elad S, Hamblin MR, et al. Low-level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: part 2: proposed applications and treatment protocols. Support Care Cancer, 2016; 24(6):2793-805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11: Samoilova KA, Zimin AA, Buinyakova AI, Makela AM, Zhevago NA. Regulatory Systemic Effect of Postsurgical Polychromatic Light (480–3400 nm) Irradiation of Breast Cancer Patients on the Proliferation of Tumor and Normal Cells in Vitro. Photomed Laser Surg, 2015; 33(11):555-63. [DOI] [PubMed] [Google Scholar]
- 12: Knyazev NA, Samoilova KA, Abrahamse H, Filatova NA. Downregulation of Tumorogenicity and Changes in the Actin Cytoskeleton of Murine Hepatoma After Irradiation with Polychromatic Visible and IR Light. Photomed Laser Surg, 2015;33(4):185-192. [DOI] [PubMed] [Google Scholar]
- 13: Knyazev NA, Samoilova KA, Abrahamse H, Filatova NA. Polychromatic Light (480–3400 nm) Upregulates Sensitivity of Tumor Cells to Lysis by Natural Killers. Photomed Laser Surg, 2016; 34(9):373-8. [DOI] [PubMed] [Google Scholar]
- 14: Tsai S-R, Yin R, Huang Y-Y, Sheu B-C, Lee S-C, Hamblin MR. Low-level light therapy potentiates NPe6-mediated photodynamic therapy in a human osteosarcoma cell line via increased ATP. Photodiagnosis Photodyn Ther, 2015; 12(1):123-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15: Abraham EH, Woo VH, Harlin-Jones C, Heselich A, Frohns F. Application and possible mechanisms of combining LLLT (low level laser therapy), infrared hyperthermia and ionizing radiation in the treatment of cancer. In: Hamblin MR, Carroll JD, Arany P. editors. Progress in Biomedical Optics and Imaging - Proceedings of SPIE, 2014. p. 893202. [Google Scholar]
- 16: Barasch A, Raber-Durlacher J, Epstein JB, Carroll J. Effects of pre-radiation exposure to LLLT of normal and malignant cells. Support Care Cancer, 2016; 24(6):2497-501. [DOI] [PubMed] [Google Scholar]
- 17: Tuner J., Hode L. The Laser Therapy Handbook. Prima Books, 2004. [Google Scholar]
- 18: M Dyson. How phototherapy affects the immune system, Proc. SPIE, 6846 (2008) 68605-1-68605-68610. [Google Scholar]
- 19: Myakishev-Rempel M, Stadler I, Brondon P, Axe DR, Friedman M, Nardia FB, et al. A Preliminary Study of the Safety of Red Light Phototherapy of Tissues Harboring Cancer. Photomed Laser Surg, 2012; 30(9):551-558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20: Ottaviani G, Martinelli V, Rupel K, Caronni N, Naseem A, Zandona L, et al. Laser Therapy Inhibits Tumor Growth in Mice by Promoting Immune Surveillance and Vessel Normalization. EBioMedicine. 2016; 11:165-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21: Samoilova K.A., Obolenskaya K.D., Vologdina A.V., Snopov S.A., Shevchenko E.V. Single skin exposure to visible polarized light induces rapid modification of entire circulating blood. 1. Improvement of rheologic and immune parameters, Proc. SPIE. 3569 (1998a) 90-103. [Google Scholar]
- 22: Samoilova K.A., O.I.Zubanova K.D., Snopov S.A., Mukhuradze N.A., Mikhelson V.M. Single skin exposure to visible polarized light induces rapid modification of entire circulating blood. 2. Appearance of soluble factors restoring proliferation and chromosome structure in X-damaged lymphocytes, Proc. SPIE. 3569 (1998b) 26-33. [Google Scholar]
- 23: Kane RC, Bross PF, Farrell AT, Pazdur R. Velcade: U.S. FDA approval for the treatment of multiple myeloma progressing on prior therapy. Oncologist, 2003; 8(6):508-13. [DOI] [PubMed] [Google Scholar]
- 24: Shabaneh TB, Downey SL, Goddard AL, Screen M, Lucas MM, Eastman A, et al. Molecular Basis of Differential Sensitivity of Myeloma Cells to Clinically Relevant Bolus Treatment with Bortezomib. Tridandapani S. editor. PLoS One. 2013. February 27; 8(2):e56132 Internet : http://dx.plos.org/10.1371/journal.pone.0056132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25: Gao XJ, Chen TS, Xing D, Wang F, Pei YH, Wei XB. Single cell analysis of PKC activation during proliferation and apoptosis induced by laser irradiation. J Cell Physiol, 2006; 206(2):441-8. [DOI] [PubMed] [Google Scholar]
- 26: Sperandio FF, Giudice FS, Correa L, Pinto DS, Hamblin MR, de Sousa SCOM. Low-level laser therapy can produce increased aggressiveness of dysplastic and oral cancer cell lines by modulation of Akt/mTOR signaling pathway. J Biophotonics, 2013; 6(10):839-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27: Gomes Henriques AC, Ginani F, Oliveira RM, Keesen TSL, Galvao Barboza CA, Oliveira Rocha HA, et al. Low-level laser therapy promotes proliferation and invasion of oral squamous cell carcinoma cells. Lasers Med Sci, 2014; 29(4):1385-95. [DOI] [PubMed] [Google Scholar]
- 28: Sroka R, Schaffer M, Fuchs C, Pongratz T, Schrader-Reichard U, Busch M, et al. Effects on the mitosis of normal and tumor cells induced by light treatment of different wavelengths. Lasers Surg Med, 1999; 25(3):263-71. [DOI] [PubMed] [Google Scholar]
- 29: Liu YH, Cheng CC, Ho CC, Pei RJ, Lee KY, Yeh KT, et al. Effects of diode 808 nm GaAlAs low-power laser irradiation on inhibition of the proliferation of human hepatoma cells in vitro and their possible mechanism. ResCommunMol-PatholPharmacol, 2004:115-16, 185-201. [PubMed] [Google Scholar]
- 30: Huang L, Wu S, Xing D. High fluence low-power laser irradiation induces apoptosis via inactivation of Akt/GSK3⊠ signaling pathway. J Cell Physiol, 2011; 226(3):588-601. [DOI] [PubMed] [Google Scholar]
- 31: Murayama H, Sadakane K, Yamanoha B, Kogure S. Low-power 808-nm laser irradiation inhibits cell proliferation of a human-derived glioblastoma cell line in vitro. Lasers Med Sci, 2012; 27(1):87-93. [DOI] [PubMed] [Google Scholar]
- 32: Renno ACM, McDonnell PA, Parizotto NA, Laakso E-L. The Effects of Laser Irradiation on Osteoblast and Osteosarcoma Cell Proliferation and Differentiation in Vitro. Photomed Laser Surg, 2007; 25(4):275-80. [DOI] [PubMed] [Google Scholar]
- 33: Dastanpour S, Momen Beitollahi J, Saber K. The effect of low-level laser therapy on human leukemic cells. J Lasers Med Sci, 2015; 6(2): 74-9. [PMC free article] [PubMed] [Google Scholar]
- 34: Samoilova KA, Bogacheva ON, Obolenskaya KD, Blinova MI, Kalmykova N V., Kuzminikh E V. Enhancement of the blood growth promoting activity after exposure of volunteers to visible and infrared polarized light. Part I: stimulation of human keratinocyte proliferation in vitro. Photochem Photobiol Sci, 2004; 3(1):96. [DOI] [PubMed] [Google Scholar]
- 35: Schartinger VH, Galvan O, Riechelmann H, Dudas J. Differential responses of fibroblasts, non-neoplastic epithelial cells, and oral carcinoma cells to low-level laser therapy. Support Care Cancer, 2012; 20(3):523-9. [DOI] [PubMed] [Google Scholar]
- 36: Reece DE, Sullivan D, Lonial S, Mohrbacher AF, Chatta G, Shustik C, et al. Pharmacokinetic and pharmacodynamic study of two doses of bortezomib in patients with relapsed multiple myeloma. Cancer Chemother Pharmacol, 2011; 67(1):57-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37: Moreau P, Pylypenko H, Grosicki S, Karamanesht I, Leleu X, Grishunina M, et al. Subcutaneous versus intravenous administration of bortezomib in patients with relapsed multiple myeloma: A randomised, phase 3, non-inferiority study. Lancet Oncol, 2011; 12(5):431-440. [DOI] [PubMed] [Google Scholar]
- 38: Musolino C, Allegra A, Innao V, Allegra AG, Pioggia G, Gangemi S. Inflammatory and Anti-Inflammatory Equilibrium, Proliferative and Antiproliferative Balance: The Role of Cytokines in Multiple Myeloma. Mediators of Inflammation, 2017:1-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39: Gao X, Xing D. Molecular mechanisms of cell proliferation induced by low power laser irradiation. J Biomed Sci. 2009; 16(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40: Song C, Luchtman D, Kang Z, Tam EM, Yatham LN, Su KP, et al. Enhanced inflammatory and T-helper-1 type responses but suppressed lymphocyte proliferation in patients with seasonal affective disorder and treated by light therapy. J Affect Disord, 2015; 185:90-6. [DOI] [PubMed] [Google Scholar]
- 41: Gavish L, Asher Y, Becker Y, Kleinman Y. Low level laser irradiation stimulates mitochondrial membrane potential and disperses subnuclear promyelocytic leukemia protein. Lasers Surg Med. 2004; 35(5):369-76. [DOI] [PubMed] [Google Scholar]
- 42: Omi T, Kawana S, Sato S, Takezaki S, Honda M, Igarashi T, et al. Cutaneous immunological activation elicited by a low-fluence pulsed dye laser. Br J Dermatol, 2005; 153(s2):57-62. [DOI] [PubMed] [Google Scholar]