

Summary
Premature ventricular contractions are common in the general population and are often seen during general anaesthesia. A high frequency of premature ventricular contractions may be associated with underlying left ventricular dysfunction. Premature ventricular contraction‐induced cardiomyopathy is a rare disease and requires cardiologist input into peri‐operative management. Medical and interventional management strategies may completely reverse the disease process. A 19‐year‐old man was scheduled for removal of tibial metalwork, due to chronic pain, and ventricular bigeminy was noted in the anaesthetic room before induction of anaesthesia. Surgery was postponed and he was later diagnosed with premature ventricular contraction‐induced cardiomyopathy. Ventricular bigeminy noted before induction of anaesthesia may not always be benign.
Keywords: peri‐operative anaesthesia, cardiomyopathy, ventricular bigeminy
Introduction
Premature ventricular contractions (PVCs) are common and could be associated with underlying structural heart disease. There is a suggestion from published evidence that a high frequency of PVCs may induce cardiomyopathy in some individuals. The term ‘PVC‐induced cardiomyopathy’ was first used to describe a sustained improvement in left ventricular function following pharmacological control of PVCs 1. The pathophysiology is characterised by impaired left ventricular function, which is induced by a high frequency of PVCs of a single morphology, typically originating from the right or left ventricular outflow tract in those with previously structurally normal hearts.
General anaesthesia in patients with underlying cardiomyopathy is associated with an increased risk of cardiac complications, which may result in postoperative death. Induction of general anaesthesia together with positive pressure ventilation can cause significant haemodynamic instability in patients with cardiomyopathy of any aetiology. Furthermore, patients with a high frequency of PVCs are at risk of arrhythmias and sudden cardiac death. Appropriate investigation and optimisation are therefore essential before even minor elective surgical procedures 2.
Report
A 19‐year‐old man presented for elective surgery to remove metalwork from his right tibia due to ongoing pain and discomfort, which was impeding his ability to exercise. He was a cigarette smoker but had no associated comorbidities. He was fit, active and played a number of sports at a competitive level. A recent open reduction and internal fixation of his tibia under general anaesthesia was uneventful. His records from this operation recorded normal sinus rhythm and PVCs were not documented at any point in the peri‐operative course.
Before induction of general anaesthesia, standard monitoring was established 3. The three‐lead ECG monitor displayed sinus rhythm with ventricular bigeminy and a heart rate of 78 beats.min–1 but the patient was asymptomatic. The bigeminal rhythm was also seen on a subsequent 12‐lead ECG (Fig. 1) and over a further 30‐min period of monitoring following intravenous sedation with intravenous (i.v.) midazolam 2 mg and i.v. fentanyl 100 μg. As this was a persistent and unexpected arrhythmia, and as underlying structural heart disease had not been ruled out, together with the elective nature of the surgery, a decision was made to defer the operation and make a specialist outpatient cardiology referral.
Figure 1.
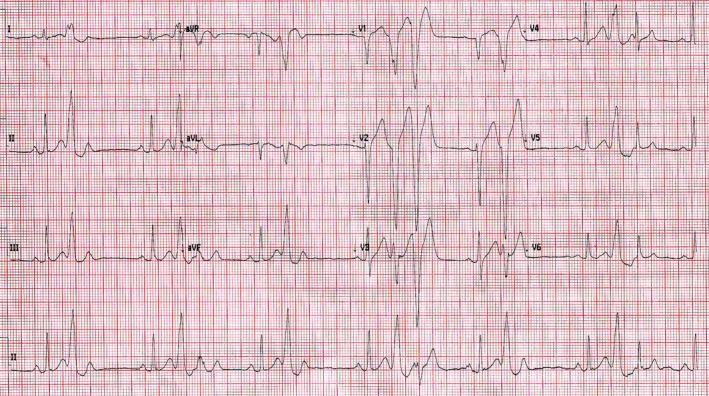
Patient's pre‐operative ECG displaying ventricular bigeminy
At the cardiology outpatient clinic, the patient described having experienced two episodes of chest pain radiating down his left arm in the preceding three months. His ECG displayed multiple PVCs thought to originate from the right ventricular outflow tract. He was prescribed bisoprolol (2.5 mg, once daily), and a 24‐h tape and cardiac magnetic resonance imaging (MRI) were arranged. The cardiac MRI images demonstrated increased left ventricular mass with a maximal wall thickness of 10 mm and a left ventricular ejection fraction of 57%. The right ventricular volume was at the upper limits of normal with low/normal wall motion and systolic function. The patient's compliance with beta‐blockade medication was poor due to resultant fatigue which he felt was impeding his performance in sport. A second cardiac MRI some months later demonstrated a progression of his disease with a dilated left ventricle and a left ventricular ejection fraction of 48%.
During this period, he remained keen to proceed with surgery and was seen at the pre‐operative assessment clinic. However, in view of the progression of his ventricular impairment and his lack of compliance with medical therapy, surgery was deferred. Given the failure of medical therapy, the cardiologist deemed it appropriate to undertake an interventional approach. The patient subsequently underwent an ablation procedure. The initial outcome was successful with the elimination of all PVCs, the return of normal sinus rhythm and cessation of symptoms. Unfortunately, he developed a recurrence of symptoms, PVCs and a further cardiac MRI demonstrated persistent biventricular impairment with a further deterioration in ventricular function. He currently awaits a repeat catheter ablation procedure.
Discussion
Although PVC‐induced cardiomyopathy was only characterised recently, the syndrome is supported by a mounting body of evidence. Strong associations have been described for many years between PVCs and stroke, coronary artery disease and sudden cardiac death 4. This prompted speculation in the cardiology community that, at least in some instances, and particularly when longstanding, PVCs may be less benign than previously thought and could possibly induce underlying structural heart disease 2. The most compelling observation has been the improvement in cardiac function observed in some patients following the suppression of PVCs with pharmacological or interventional treatment.
The pathophysiology of PVC‐induced cardiomyopathy has not been definitively elucidated, but it is thought that, through electromechanical asynchrony, PVCs may cause sequential instead of parallel activation of the myocardium, which in turn causes remodelling effects and cardiomyopathy 4. Patients presenting with a longer duration of symptoms have greater ventricular dysfunction at the time of presentation 5. There is also an association between the frequency of PVCs and the development of ventricular dysfunction 6. Suggested PVC frequency correlating with an increased risk include greater than 20,000 PVCs or greater than 20% PVCs over a 24‐h period 7.
PVC‐induced cardiomyopathy appears to be a dilated cardiomyopathy, with an increase in end‐systolic dimensions seen on echocardiography 8. It may occur in isolation in younger patients or may contribute to further deterioration in ventricular dysfunction in those with cardiomyopathies of other aetiologies. Certain characteristics of PVCs appear to be of pathological significance. A longer QRS interval duration places the patient at increased risk of induced cardiomyopathy, as does a higher coupling interval such as in a bigeminal or trigeminal pattern 9.
Recognised treatments of PVC‐induced cardiomyopathy include pharmacological and interventional approaches. In patients who are mildly symptomatic, a trial of beta‐blockade or calcium channel blockade is the recommended first‐line treatment. Flecainide has also been successfully used due to its potent suppression of PVCs but is not recommended in those with underlying structural heart disease. Amiodarone can also improve symptomatic control but is favoured for long‐term use, particularly in younger patients 4.
Interventional management in the form of catheter ablation remains the gold standard treatment. First described by Chugh et al. in 2000, it has a higher success rate in reversing underlying ventricular dysfunction than medical therapy alone 10. The origin of PVCs is important in determining the likelihood of successful treatment, with those originating from the right ventricular outflow tract more amenable to successful catheter ablation 11. A short PVC QRS duration is another independent predictor of the success of interventional management 10. Not all catheter ablations are successful, and when ablation is unsuccessful, the re‐appearance of PVCs can cause a recurrence of PVC‐induced cardiomyopathy. In such patients, repeat interventional management is often considered. Alternatively, resumption of pharmacological treatment may have beneficial effects in reducing symptom burden and improving quality of life 12.
Little has been reported regarding the appropriate anaesthetic management of patients with PVC‐induced cardiomyopathy. Anaesthetic risk is largely related to the severity of the underlying ventricular dysfunction. Haemodynamic alterations induced by anaesthesia can precipitate acute heart failure as well as sudden cardiac death in these patients. Decisions to proceed with elective surgery should be based on a multidisciplinary approach with input from cardiologists, anaesthetists and surgeons. Patients presenting for emergency surgery constitute an additional challenge due to the unpredictability of haemodynamic responses.
In conclusion, PVCs are common and a small number of patients may have underlying cardiac pathology. There are some features that should prompt suspicion of associated underlying heart disease. These include a high frequency of PVCs, wide QRS duration and associated red flag symptoms. The risks vs. benefits should be carefully considered before undertaking elective surgery in patients with known or suspected PVC‐induced cardiomyopathy. Involvement of a specialist cardiology service in pre‐operative management is essential. Appropriate treatment can lead to the elimination of PVCs and reversal of underlying ventricular dysfunction. In patients presenting for emergency surgery, the principles of management of patients with a dilated cardiomyopathy should apply 13.
Competing Interests
No external funding and no competing interests declared.
Acknowledgements
Published with the written consent of the patient.
References
- 1. Duffee DF, Shen W‐K, Smith HC. Suppression of frequent premature ventricular contractions and improvement of left ventricular function in patients with presumed idiopathic dilated cardiomyopathy. Mayo Clinic Proceedings 1998; 73: 430–3. [DOI] [PubMed] [Google Scholar]
- 2. Lee L, Tsai P, Ip K, Irwin M. Pre‐operative cardiac optimisation: a directed review. Anaesthesia 2019; 74: 67–79. [DOI] [PubMed] [Google Scholar]
- 3. Checketts M, Alladi R, Ferguson K, et al. Recommendations for standards of monitoring during anaesthesia and recovery 2015: Association of Anaesthetists of Great Britain and Ireland. Anaesthesia 2016; 71: 85–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Saurav A, Smer A, Abuzaid A, Bansal O, Abuissa H. Premature ventricular contraction‐induced cardiomyopathy. Clinical Cardiology 2015; 38: 251–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Yokokawa M, Kim HM, Good E, et al. Relation of symptoms and symptom duration to premature ventricular complex–induced cardiomyopathy. Heart Rhythm: The Official Journal of the Heart Rhythm Society 2012; 9: 92–5. [DOI] [PubMed] [Google Scholar]
- 6. Baman TS, Lange DC, Ilg KJ, et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm: The Official Journal of the Heart Rhythm Society 2010; 7: 865–9. [DOI] [PubMed] [Google Scholar]
- 7. Niwano S, Wakisaka Y, Niwano H, et al. Prognostic significance of frequent premature ventricular contractions originating from the ventricular outflow tract in patients with normal left ventricular function. Heart 2009; 95: 1230–7. [DOI] [PubMed] [Google Scholar]
- 8. Huizar JF, Kaszala K, Potfay J, et al. Left ventricular systolic dysfunction induced by ventricular ectopy: a novel model for premature ventricular contraction‐induced cardiomyopathy. Circulation: Arrhythmia and Electrophysiology 2011; 4: 543–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Del Carpio Munoz F, Syed FF, Noheria A, et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. Journal of Cardiovascular Electrophysiology 2011; 22: 791–8. [DOI] [PubMed] [Google Scholar]
- 10. Chugh SS, SHEN WK, Luria DM, Smith HC. First evidence of premature ventricular complex‐induced cardiomyopathy: a potentially reversible cause of heart failure. Journal of Cardiovascular Electrophysiology 2000; 11: 328–9. [DOI] [PubMed] [Google Scholar]
- 11. Kim Y‐H, Park S‐M, Lim HE, Pak H‐N, Kim Y‐H, Shim W‐J. Chronic frequent premature ventricular complexes originating from right and non‐right ventricular outflow tracts. International Heart Journal 2010; 51: 388–93. [DOI] [PubMed] [Google Scholar]
- 12. Deyell MW, Park K‐M, Han Y, et al. Predictors of recovery of left ventricular dysfunction after ablation of frequent ventricular premature depolarizations. Heart Rhythm: The Official Journal of the Heart Rhythm Society 2012; 9: 1465–72. [DOI] [PubMed] [Google Scholar]
- 13. Alexoudis A, Spyridonidou A, Vogiatzaki T, Iatrou C. Anaesthetic implications of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Anaesthesia 2009; 64: 73–8. [DOI] [PubMed] [Google Scholar]