

Abstract
Brugada syndrome is a form of inherited arrhythmia syndrome characterized by a distinct ST‐segment elevation in the right precordial leads. Brugada phenocopies are clinical entities that present with an electrocardiographic pattern identical to Brugada syndrome and may obey to various clinical conditions. We present a case of a suicidal attempt using a high dose of propafenone causing a Brugada‐type electrocardiographic pattern. Is this a Brugada syndrome case, a Brugada phenocopy or something else?
Keywords: Brugada phenocopy, brugada syndrome, ECG, propafenone
1. INTRODUCTION
Brugada syndrome (BrS) is a form of inherited arrhythmia syndrome characterized by a distinct ST‐segment elevation in the right precordial leads with no apparent structural heart disease Brugada & Brugada, 1992;. Brugada phenocopies (BrPs) are clinical entities characterized by electrocardiogram (ECG) patterns presumed to be identical to those of true BrS but are elicited by various other underlying conditions such as myocardial ischemia, electrolyte and metabolic disorders, and others Baranchuk et al. 2012; Hunuk et al. 2016; Awad et al. 2013; Ferrando‐Castagnetto et al. 2016; Genaro et al. 2014; Rambod, Elhanafi, & Mukherjee, 2015;. Propafenone is a Class 1C antiarrhythmic drug which also exhibits β‐adrenergic and calcium channel‐blocking activities. Propafenone, at standard doses, can cause many ECG changes including prolongation of the PR interval, bundle branch block, widening of the QRS and QT intervals, ventricular tachycardia and bradycardia Thompson et al. 1988. We present a case of a suicidal attempt with a high dose of propafenone causing a Brugada ECG pattern.
2. CASE REPORT
A 36‐year‐old woman was admitted to the emergency room due to a suicidal attempt using a large dose of propafenone (150 mg, 36 tablets) followed by loss of consciousness and generalized tonic–clonic seizure. Anamnesis was obtained from the family. She had no previous history of heart disease, syncope, cardiac arrhythmia nor family history. Physical examination revealed blood pressure 70/40 mm Hg and heart rate of 95 bpm. The initial 12‐lead ECG demonstrated irregular wide QRS rhythm with a QRS duration of 160 ms and ST‐segment elevation in leads V1–V2 consistent with a Brugada ECG pattern (Figure 1). She arrested and cardiopulmonary resuscitation was initiated with restoration of electrical activity. The 12‐lead ECG the next day showed resolution of the Brugada ECG pattern (Figure 2). An ajmaline challenge test failed to induce a Brugada ECG pattern (Figure. 3). After a full recovery, the patient was discharged with follow‐up by the psychiatry division.
Figure 1.
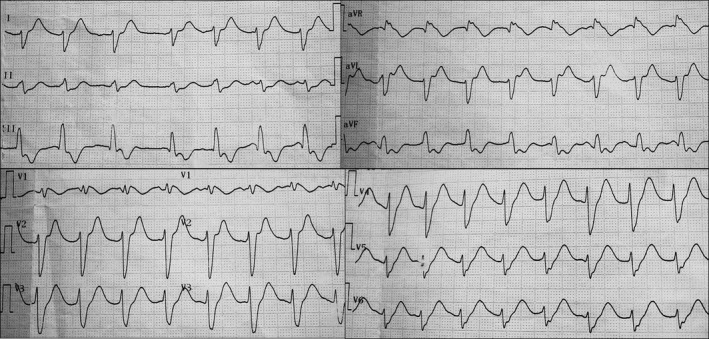
Twelve‐lead ECG on admission: Brugada ECG pattern after propafenone overdose
Figure 2.
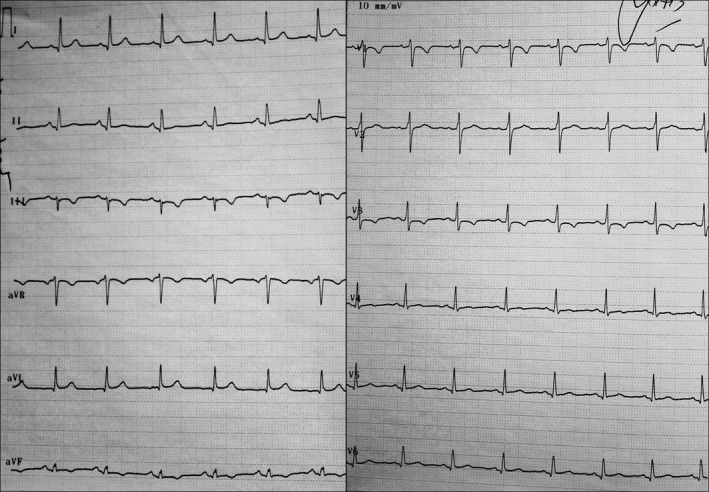
Twelve‐lead ECG is showing resolution of the Brugada ECG pattern
Figure 3.
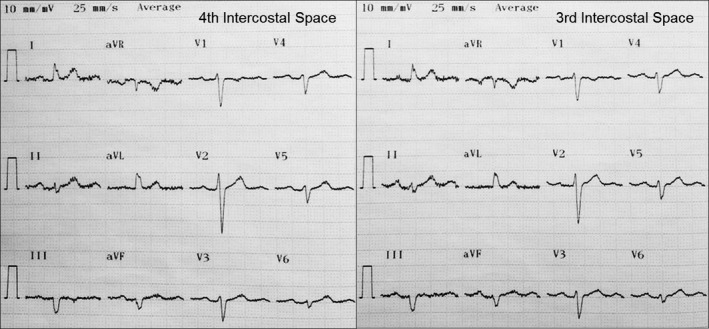
Twelve‐lead ECG from third and fourth intercostal spaces after negative ajmaline challenge test
3. DISCUSSION
Brugada phenocopies are clinical entities that present with identical ECG patterns to those of true congenital BrS but are elicited by various other clinical circumstances Baranchuk et al. 2012; Hunuk et al. 2016; Awad et al. 2013; Ferrando‐Castagnetto et al. 2016; Genaro et al. 2014; Rambod et al. 2015. Differentiating BrP from BrS is very important for preventing misdiagnosis and unnecessary treatment. The diagnosis criteria for BrP include the following: Brugada ECG pattern identical to BrS and a recognizable underlying condition; normalization of the ECG pattern after resolution of the underlying condition; low clinical pretest probability for true BrS and a negative provacative tests with sodium channel blockers (ajmaline, flecainide, procainamide) and, if possible, a negative genetic testing Anselm, Evans, & Baranchuk, 2014. Sodium channel blocking agents are used to unmask BrS in patients suspected to have the syndrome Antzelevitch et al. 2005. Propafenone is a Class Ic antiarrythmic drug which blocks the sodium channels. Brugada ECG pattern and QRS complex widening have been seen with the use of propafenone and other class IC antiarrhythmic agents Hasdemir et al. 2006. In propafenone overdose, PR prolongation, QRS widening, bundle branch block, ventricular arrythmia, bradicardia and hypotension were reported Thompson et al. 1988. However, the effect on the sodium channels with a huge overdose of propafenone has not been reported yet. We speculate that a large dose of propafenone may turn the sodium channel dysfunctional; even in the absence of a genetic mutation.
The term BrP does not include Brugada ECG patterns induced by medications that block the sodium channels, thus, this case of Propafenone overdose should not be considered a BrP. Having a normal sodium channel test in a controlled environment, indicates a very low probability of low Brugada syndrome. Thus, this case could labeled as “acquired sodium channel dysfunction,” induced by a toxic dose of propafenone; instead of BrS or BrP.
CONFLICT OF INTEREST
None to declare.
Kocabas U, Hasdemir C, Kaya E, Turkoglu C, Baranchuk A. Brugada syndrome, Brugada phenocopy or none? Ann Noninvasive Electrocardiol. 2017;22:e12470 10.1111/anec.12470
REFERENCES
- Anselm, D. D. , Evans, J. M. , & Baranchuk, A. (2014). Brugada phenocopy: A new electrocardiogram phenomenon.World. Journal of Cardiology, 6, 81–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antzelevitch, C. , Brugada, P. , Borggrefe, M. , Brugada, J. , Brugada, R. , Corrado, D. , … Wilde, A. (2005). Brugada syndrome: Report of the second consensus conference: Endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation, 111, 659–670. [DOI] [PubMed] [Google Scholar]
- Awad, S. F. , Barbosa‐Barros, R. , Belem Lde, S. , Cavalcante, C. P. , Riera, A. R. , Garcia‐Niebla, J. , … Baranchuk, A. (2013). Brugada phenocopy in a patient with pectus excavatum: Systematic review of the ECG manifestations associated with pectus excavatum. Annals of Noninvasive Electrocardiology, 18, 415–420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baranchuk, A. , Nguyen, T. , Ryu, M. H. , Femenía, F. , Zareba, W. , Wilde, A. A. , … Pérez‐Riera, A. R. (2012). Brugada phenocopy: New terminology and proposed classification. Annals of Noninvasive Electrocardiology, 17, 299–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brugada, P. , & Brugada, J. (1992). Right bundle branch block, persistent ST segment elevation and sudden cardiac death: A distinct clinical and electrocardiographic syndrome. A multicenter report. Journal of the American College of Cardiology, 20, 1391–1396. [DOI] [PubMed] [Google Scholar]
- Ferrando‐Castagnetto, F. , Garibaldi‐Remuñan, A. , Vignolo, G. , Ricca‐Mallada, R. , & Baranchuk, A. (2016). Brugada phenocopy as a dynamic electrocardiographic pattern during acute anterior myocardial infarction. Annals of Noninvasive Electrocardiology, 21, 425–428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Genaro, N. R. , Anselm, D. D. , Cervino, N. , Estevez, A. O. , Perona, C. , Villamil, A. M. , … Baranchuk, A. (2014). Brugada phenocopy clinical reproducibility demonstrated by recurrent hypokalemia. Annals of Noninvasive Electrocardiology, 19, 387–390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasdemir, C. , Olukman, M. , Ulucan, C. , & Roden, D. M. (2006). Brugada‐type ECG pattern and extreme QRS complex widening with propafenone overdose. Journal of Cardiovascular Electrophysiology, 17, 565–566. [DOI] [PubMed] [Google Scholar]
- Hunuk, A. , Hunuk, B. , Kusken, O. , & Onur, O. E. (2016). Brugada phenocopy induced by electrolyte disorder: A transient electrocardiographic sign. Annals of Noninvasive Electrocardiology, 21, 429–432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rambod, M. , Elhanafi, S. , & Mukherjee, D. (2015). Brugada phenocopy in concomitant ethanol and heroin overdose. Annals of Noninvasive Electrocardiology, 20, 87–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson, K. A. , Iansmith, D. H. , Siddoway, L. A. , Woosley, R. L. , & Roden, D. M. (1988). Potent electrophysiologic effects of the major metabolites of propafenone in canine Purkinje fibers. Journal of Pharmacology and Experimental Therapeutics, 244, 950–955. [PubMed] [Google Scholar]