
Figure 1.
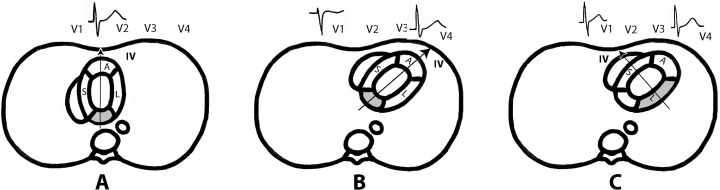
(A) Posterior (inferobasal) wall as it was wrongly considered to be placed. With this location an infarction vector of posterior or inferobasal infarction faces V1‐V2 and explains the RS pattern in these leads. (B) and (C) The real anatomic position of posterior (now named inferobasal segment) and lateral wall infarctions. The infarction vector of inferobasal segment faces V3‐V4 and not V1, and may contribute to the normal RS pattern seen in these leads. On the contrary, the vector of infarction of the lateral wall faces V1 and may explain RS pattern in this lead. However, we have to keep in mind that in the majority of cases, except in very lean individuals (see Fig 2C), the part of inferior wall that is rarely posterior just involves the area of late depolarization (Segment 4 or inferobasal). Therefore, in case of MI, there would not be changes in the first part of QRS because the infarction does not produce the presence of Q wave or equivalent (see text).