

Abstract
Background:
Infertility causes change according to local demographics. There is thus the need to find the causes of infertility in context to local population to aid and direct management strategies accordingly.
Aims:
The aims were to study the causes of infertility and to calculate the proportion of the individual factors contributing to it in the population coming to a tertiary level public health facility. Setting and Design: This cross-sectional, observational study was done in an infertility clinic in a medical college and government hospital.
Materials and Methods:
The study comprised 120 couples who came for infertility evaluation and treatment. Cause of infertility in the couple was assigned on the basis of history and examination findings. The prevalence of each cause was evaluated.
Statistical Analysis:
Results were tabulated, and the prevalence of individual factors was calculated. Intratable analysis was done using SPSS 16.0.
Results:
Primary infertility (57.5%) was more prevalent than secondary infertility (42.5%). Female factor accounted for 46.6% of the cases with polycystic ovarian syndrome (PCOS) being the leading cause (46%). Infertility was seen equally in lean and obese PCOS cases. Infectious causes such as pelvic inflammatory disease and tuberculosis were significantly associated with tubal factor infertility (P = 0.001). Infertility causes changed as the age of marriage increased. In couples married for less than 5 years, PCOS was the main cause whereas later,male factor and unexplained infertility were the most common causes seen. Male factor contributed to 20% of the cases of infertility, and both tobacco and alcohol consumption were significantly associated with abnormal semen reports (P = 0.001).
Conclusion:
Causes of infertility vary according to the age of the couples and age of marriage. Although PCOS remains the main cause, infections are a major cause of tubal factor infertility, and tobacco and alcohol worsen the male factor. One-third of the cases still remain unexplained.
KEYWORDS: Infertility, lean and obese polycystic ovarian syndrome, male factor infertility, oligospermia, prevalence, public sector
INTRODUCTION
Infertility affects roughly 10% of the world's population. The WHO ranks infertility in the young population as the fifth highest serious global disability. According to the Maternal Health Task Force 2010, 50 million couples worldwide are infertile.
In 1981, in India, approximately 13% of ever-married women of reproductive age were childless, which increased to nearly 16% in 2001.[1] According to the ICMR survey carried out in 13 districts and sampling 37,570 women, the prevalence of primary infertility in urban areas is 4% and is 3.7% in rural areas. According to the data from the District Level Household and Facility Survey carried out in India during 2007–2008, 8% of the married women reported infertility. Thus, it is now established beyond doubt that infertility has become a major medical concern for sizeable amount of the young population in all types of demographical settings in India, urban as well as rural.
Historically, the main causes of infertility were infections such as gonorrhea and sexually transmitted diseases, but today, they have been replaced by stress, male factor, etc., and with all our armamentariums, a sizable chunk still needs to be classified as unexplained infertility. Furthermore, the increasing prevalence of medical disorders such as diabetes, hypertension, and hypothyroidism and lifestyle diseases such as obesity and addictions in the young has also shown to contribute to the problem of infertility.
Many studies have been undertaken worldwide, and in India, to know the common causes of infertility, however, extrapolation of one study cannot be done to the general population as infertility is a multifactorial problem and needs to be seen in the local context of the factors causing it. In countries such as India, the prevalence of tuberculosis (TB) being high, infectious diseases contributing to infertility becomes a major factor.[2] Thus, infertility needs to be seen in context to the local population. Furthermore, infertility not only is a medical challenge but also takes a major toll psychologically and financially on the couples.[3] Thus, we have undertaken this study to know the commonest causes of infertility prevalent locally and to know the prevalence of each factor in order to ensure the prompt and effective management of these cases.
Aims and objectives
To study the causes of infertility in the patients attending an infertility clinic in a tertiary care center
To calculate the proportion of the individual factors causing infertility in the patients attending an infertility clinic.
MATERIALS AND METHODS
This was a cross-sectional, observational, descriptive study in an infertility clinic in the department of obstetrics and gynecology of a tertiary care center. The study was conducted after the approval of the ethics committee for a duration of 1½ years.
Study participants
A sample of 120 patients were selected by simple random sampling from and included in the study after taking a written, valid, and informed consent. Women married for more than 1 year in the age group of 19–49 years, cohabiting women, and women without the use of contraceptives either as cases of primary or secondary infertility were included in the study.
Methodology
Patients attending an infertility clinic were enrolled in the study, and on the first visit, a detailed history of the couples was taken. Data from the consenting patients were collected by oral interview, examination, and review of records. The data were documented in a structured case record form that documented the following information – demographic details, detailed infertility history including history of any previous treatment taken, surgical history, and coital history. Examination findings were documented including the general and specific examination findings. Reports of investigations done and any detail of any previous infertility treatment taken were also documented.
Statistical analysis
Analysis of the data was done using the software SPSS 16.0 (Released 2016. IBM SPSS Statistics for Windows, Version 24.0. IBM Corp., Armonk, New York). The study included both quantitative and qualitative data, and the results were documented in the form of charts, tables, and pie diagrams.
RESULTS
The qualitative and quantitative data of the study population were analyzed using means, medians, and percentages and the Fisher's exact test to obtain the degree of significance [Table 1].
Table 1.
Demographical characteristics of the study population
| Characteristics | Female (n=120) | Male (n=120) |
|---|---|---|
| Mean age | 28.35 | 32.88 |
| Education (%) | 10th pass (65) | 12th pass (70) |
| Occupation (%) | Homemaker (95) | On job (97) |
| Addictions (%) | 1.7 | 33.3 |
Majority of the patients were in the age group of 25–30 years in women (56/120), and the next most common age group was more than 30 years (38/120).
Couples were married for a mean duration of 6.7 years ± 2 years before taking treatment. We had a nearly equal proportion of couples who were married for up to 5 years and those for more duration (57 vs. 63). The comparison of common causes of infertility according to the duration of marriage is summarized in Table 2.
Table 2.
Causes and prevalence of factors causing infertility according to age of marriage
| Factor | Prevalence in couples married for up to 5 years (%) | Prevalence in couples married for >5 years (%) |
|---|---|---|
| PCOS | 28 | 22 |
| Tubal factor | 19.2 | 20 |
| Male factor | 10 | 20 |
| Unexplained infertility | 33 | 38 |
PCOS=Polycystic ovarian syndrome
Thus, as the age of marriage increases, infertility due to tubal factor, male factor, and unknown causes increases.
History of addictions studied revealed that while, in women, the prevalence was negligible, more than one in three men had some form of addiction, of which 95% consumed some form of tobacco.
The causes of infertility in the 120 couples were divided into four standard categories as follows:
Female factor
Male factor
Combined causes
Unexplained infertility [Figure 1].
Figure 1.
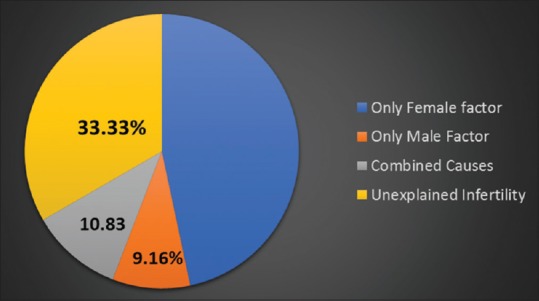
Distribution of the causes of infertility as found in our study
Analyzing the female factor in detail where it was responsible for infertility, it was found that the main cause found in our study population was the ovarian cause (polycystic ovarian syndrome [PCOS]) [Figure 2].
Figure 2.
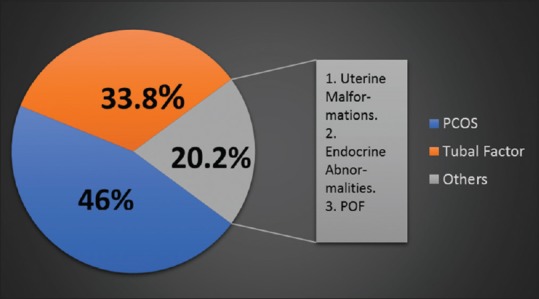
Causes of female factor infertility
Tubal pathologies included pelvic inflammatory disease (PID), genital TB, and endometriosis, and uterine causes (malformations and fibroids) with endocrine causes contributed to 20%. There was one case of premature ovarian failure.
While majority of the females did not have any medical comorbidity, the most common ones seen were endocrine disorders [Figure 3].
Figure 3.
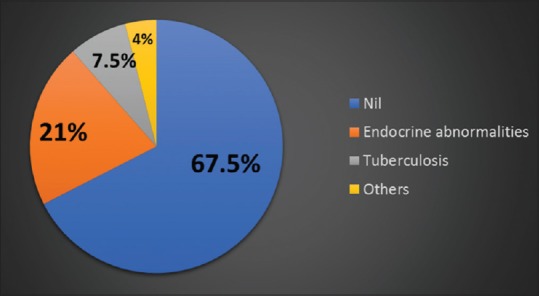
Comorbid medical conditions in infertile women
Hypothyroidism was the most common endocrine disorder followed by diabetes mellitus. There were ten cases of TB and three cases having more than one endocrine disorder.
For the diagnosis of PCOS, the sensitivity of Transvaginal Sonography (TVS) was 73.33%, diagnosing 2 of the 30 designated as PCOS. Other findings on TVS encountered were leiomyomas, ovarian cysts, and endometriosis [Table 3].
Table 3.
Results of TVS in the study population
| TVS findings | Frequency (n=120), n (%) |
|---|---|
| PCOS | 22 (16.67) |
| Leiomyomas | 10 (7.5) |
| Simple ovarian cysts (unilateral/bilateral) | 6 (5) |
| Endometriosis | 3 (2.5) |
| Normal | 79 (65.83) |
PCOS=Polycystic ovarian syndrome, TVS=Transvaginal sonography
Another investigation that was done in more than half of the female partners in the study population was hysterosalpingography (HSG). HSG was performed as the second-line investigation when no cause was found on TVS and examination and when tubal disease was suspected. The common findings noted are summarized in Table 4.
Table 4.
Results of hysterosalpingography in the study population (n=66)
| HSG findings | Frequency, n (%) |
|---|---|
| Unilateral tubal block (left/right) | 5 (7.57) |
| Bilateral tubal block | 9 (13.63) |
| Peritubal adhesions | 10 (15.15) |
| Uterine anomaly | 4 (6.06) |
| Normal | 38 (57.57) |
HSG=Hysterosalpingography
In 45 patients, a diagnostic laparoscopy was performed along with hysteroscopy in 40 patients. The results of the same are summarized in Table 5.
Table 5.
Results of hysteroscopy and laparoscopy in the study population
| Frequency, n (%) | |
|---|---|
| Hysteroscopy findings | n=40 |
| Polyps | 1 (2.5) |
| Adhesions | 1 (2.5) |
| Septum | 3 (7.5) |
| Normal findings | 35 (87.5) |
| Laparoscopy findings | n=45 |
| Leiomyomas | 2 (4.4) |
| Endometriosis | 4 (8.8) |
| Tuberculosis, adhesions | 10 (22.2) |
| Ovarian pathology | 1 (2.2) |
| Tubal blocks | 3 (6.6) |
| Uterine anatomical anomaly | 12.2) |
| Normal findings | 24 (53.3) |
Twenty-three patients who had an HSG had undergone a hysteroscopy and laparoscopy for further evaluation. The sensitivity of HSG for diagnosing a tubal block was found to be 73.33% and specificity of 57.14% by comparing the results of the HSG with laparoscopy findings.
Furthermore, the diagnosis of endometriosis was established conclusively only by laparoscopy in all the four cases with the TVS being normal in these patients.
For the evaluation of male infertility, semen analysis was done in all males, and 24 males had abnormal reports. The age distribution of men with semen abnormalities is shown in Figure 4.
Figure 4.
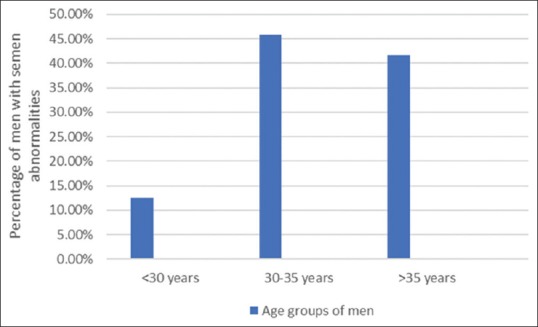
Correlation of age with semen analysis
Thus, the proportion of semen abnormalities increases as the age of the male partners increases.
Identifying the types of abnormalities, the semen characteristics in study population are summarized in Table 6.
Table 6.
Semen characteristics in study population (n=120)
| Semen characteristic | n (%) |
|---|---|
| Oligospermia | 17 (10) |
| Disorder of motility | 3 (0.83) |
| Disorder of morphology | 5 (2.54) |
| Combination | 4 (3.33) |
| Azoospermia | 4 (3.33) |
| Normal | 96 (80) |
Furthermore, a statistically significant correlation was found between men with semen abnormalities consuming alcohol, smoking, or chewing tobacco or a combination of the above (P = 0.001).
DISCUSSION
The overwhelming statistics about population growth usually buries a graver problem of population dynamics that we are facing today – “infertility.”
The European Society of Human Reproduction and Embryology (ESHRE) in 2007 did a comprehensive review of 28 studies that were published since 1900 on infertility and concluded that the overall prevalence of infertility was 9%. This varied from 3.5%–16.7% in developed countries to 6.9%–9.3% in developing nations.[4] In an analysis of 277 demographic and health surveys, to determine infertility trends since 1990–2010, it was seen that infertility prevalence was highest in South Asia, Sub-Saharan Africa, North Africa/Middle East, and Central/Eastern Europe and Central Asia.[5]
The National Family Health Survey 1, 2, 3, and 4 show that the prevalence of primary infertility is consistently more than secondary infertility in urban areas.[6] In our study also, the prevalence of primary infertility was 57.5% versus 42.5% of secondary infertility. Furthermore, studies done worldwide by Allow et al., Farhi and Ben-Haroush, and Masoumi et al.[7,8,9] show that the incidence of primary infertility is more than that of secondary infertility.
Female age is the most important determinant of spontaneous as well as pregnancies from assisted reproduction. Fecundity starts declining in the fourth decade and fertility starts declining as early as 32 years, and hence, late childbearing is often defined after the age of 35 years.[10] The average age of the female partners coming for infertility treatment in our study is 28 years. The average age of the husbands was found to be 33 years. Furthermore, as the age of marriage increases, the incidence of infertility increases.[11] In our study, the age of marriage varied from 1.5 years to 18 years and the average age being 6.7 years.
Apart from individual age of the female and male partners, the age of marriage also influences the cause of infertility. In couples married for <5 years, PCOS and tubal causes related to sexually transmitted infections were more commonly found, whereas in couples married for >5 years, the proportion of unexplained infertility and male factor increased. This can be correlated to the increasing age of both the partners leading to reduction in the quality and quantity of both ova and sperms.
In our study, the prevalence of female factor exclusively causing infertility was found to be 46.6%.
Among the causes of female infertility found, PCOS and tubal pathology were the most common causes contributing 46% and 33.8%, respectively, to all cases attributed to female infertility. Studies done by Mittal et al. in Haryana, Patel et al. in Indore, and Rajashekar et al. in Bangalore also show that the main female factor causing infertility is PCOS.[12,13,14] Studies done worldwide also prove that PCOS is the single most common cause of female factor of infertility.[8,15,16] We also found that there was no statistical significance in the patients with PCOS who were either overweight or obese and those with normal body mass index (P = 0.682), showing that the lean PCOS patients are equally prone for infertility as the obese PCOS. Studies have shown that in cases of lean PCOS, 6%–22% of them had insulin resistance. Thus, they needed some form of ovulation induction and sometimes intrauterine insemination (IUI) for conception. This implies that lean PCOS patients also suffer from some form of infertility.
Tubal factor infertility was the second most common cause of female infertility contributing to 33.8% of the cases. The prevalence of tubal factor causing infertility was found to be between 15% and 20% by Elussein et al., Masoumi et al., and Farhi and Ben-Haroush.[8,9,17] This increased prevalence of the tubal factor causing infertility can be attributed to the increased prevalence of PID and genital TB in the South Asian countries. We have found a statistically significant correlation between tubal damage (tubal blocks and hydrosalpinx) and history of PID and/or genital TB (P = 0.002). Endometriosis causing tubal distortion was found in 7.6% of the cases. Thus, early detection and timely treatment of PID is very essential to address this cause of infertility.
The most common initial test done for tubal patency evaluation was HSG, with a sensitivity of 73.33% and a specificity of 57.14%. The sensitivity and specificity of HSG for evaluation of the bilateral tubal patency and unilateral or bilateral block as quoted in literature are 77.8% and 52.94%, respectively.[18] It can be concluded that in a low-resource setting, HSG can be used for evaluating tubal status. However, the low specificity of HSG makes laparoscopy a more reliable option. In 94% cases, HSG findings showing patent tubes were confirmed on laparoscopy showing a good negative predictive value of HSG; however, the positive predictive value was only 56%.
Around 20% of the causes of female infertility were attributed to uterine fibroids, endocrine abnormalities, or a combination of the above factors.
Among the comorbidities in infertile females, the most common ones seen are the endocrine abnormalities. Thyroid disorders were the most common endocrine abnormalities, seen in 21.6% of the infertile population who were screened for the same. Our results correlate with those of Verma et al. where they found the prevalence of hypothyroidism in infertile women to be 23.9%.[19] Thus, all infertile women need to get a basic screen for hypothyroidism done.
Male factor is the cause of infertility in one-third of the couples who are infertile. Studies by Elussein et al., Farhi and Ben-Haroush, and Allow et al. show the prevalence of male factor between 30% and 45% in infertile couples. In our study, male factor was the sole cause of infertility in around 10% of the couples and contributed as a combined cause in another 10% of the infertile population.
A basic semen analysis has been quoted to have a sensitivity of 89.6% to diagnose a case of male factor infertility.[20] In all our patients, a semen analysis was done, and isolated semen abnormalities without any local or hypothalamic cause were most commonly seen. Abnormal semen parameters are seen in approximately 7% of the infertile couples.[21] In our study, they were seen in 20.8% of the males. Studies all over the world and two large studies done in South India and AIIMS have shown that the average sperm count of males is reducing. Furthermore, more importantly, the prevalence of low counts with abnormal forms is increasing. This represents a qualitative deterioration in the semen parameters.[18,20] Two notable factors responsible for this found in our study were husband's age and history of addictions.
Correlating the age of the husbands and the semen analysis, it was seen that 70.83% of men were in the age group of more than 30 years. An Iran study[9] quotes that they had 43% of infertile men in the age group of 30–40 years. Various studies have quoted that there is a significant decrease (0.17% to 0.6% per year) in sperm motility according to increasing age.
Sharma et al. in 2012 showed that heavy smoking resulted in reduced sperm number and alcohol consumption is associated with an increase in morphologically abnormal sperms.[22] Our study confirms the above with tobacco and alcohol being the most prevalent addictions significantly affecting semen quality.
Prevalence of combined causes for infertility as seen by Phillapov et al. is 38%, Bayasgalen 18.8%, whereas Zarger from Kashmir, India, reported it only to be 5.2%. Our study puts it at 10.8%.
In the combination of female and male factors, ovulatory disorders with abnormal semen were the most common combination followed by tubal infertility combined with abnormal semen.
Furthermore, in combined female factors, ovulation disorders with tubal factor were the most common combination seen. Hence, it is seen that it is important to evaluate both the partners in cases of infertility.
Unexplained infertility is a diagnosis of exclusion after evaluation of the male and female factors fails to identify a specific cause for infertility. The incidence of unexplained infertility is quoted to be around 30%.[23] In our study, of 120 couples, 34% of the couples had unexplained infertility. Gelbaya et al. in their review of literature from 1950 to 2013 found that even after doing standard fertility tests, in 15%–30% of couples, no cause will be identified.[24] However, again in the past 10 years, the proportion of unexplained infertility is increasing again. This is seen in studies done by Elussein et al. in 2008 and Farhi and Ben-Haroush in 2011 quoting the incidence of unexplained infertility as 13% and 20.7%, respectively, and 32.5% seen in our study.[8,17]
This cross-sectional observational study was conducted in a public sector tertiary care center. Being an observational study, we were just able to gather information regarding history and investigations done at the point of contact. No intervention in the form of investigations and treatment was possible. Hence, critical investigations from infertility point of view such as serum thyroid-stimulating hormone were found to be missing in some cases. Furthermore, especially in cases that were classified as unexplained infertility, it was noted that diagnostic hysterolaparoscopy was not done in all those cases. Thus, we will remain unaware of the underlying cause in those patients.
The center where the study was conducted has facilities that included only the basic diagnosis of female and male infertility and provision of basic assisted reproductive technology like IUI. For the socioeconomic class that the hospital caters to, nonaffordability of infertility services and lack of knowledge regarding the same were the main barriers noted that prevented the patients from seeking treatment earlier.
CONCLUSION
In the population coming to a public sector tertiary care center, the incidence of primary infertility is more than secondary infertility. Increasing age of marriage influences the causes with unexplained infertility and male factor more commonly seen as the age of marriage increases. Female factor remains the main cause of infertility followed by unexplained causes. Among the female causes, PCOS remains the most common cause followed by tubal factor. In PCOS patients, the prevalence of infertility is equal in obese as well as lean PCOS. Tubal factor infertility is significantly associated with PID and TB confirming the fact that in our country, infections do cause a significant proportion of infertility. HSG still remains the investigation of choice for low-resource setting for excluding tubal factor, whereas laparoscopy remains the gold standard for confirming it. All patients should be screened for hypothyroidism as a part of the infertility workup. Male factor is a significant cause of infertility with semen parameters being affected by age and by consumption of tobacco and alcohol.
The problem of infertility has become universal now, and thus, understanding of the causes is the first step in solving this issue.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to thank Dr. Madhva Prasad for constant support and encouragement.
REFERENCES
- 1.Sarkar S, Gupta P. Socio-demographic correlates of women's infertility and treatment seeking behaviour in India. J Reprod Infertility. 2016;17:123–32. [PMC free article] [PubMed] [Google Scholar]
- 2.Sharma JB, Dharmendra S, Agarwal S, Sharma E. Genital tuberculosis and infertility. Fertil Sci Res. 2016;3:6–18. [Google Scholar]
- 3.Patel A, Sharma PS, Kumar P, Binu VS. Sociocultural determinants of infertility stress in patients undergoing fertility treatments. J Hum Reprod Sci. 2018;11:172–9. doi: 10.4103/jhrs.JHRS_134_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of infertility prevalence and treatment-seeking: Potential need and demand for infertility medical care. Hum Reprod. 2007;22:1506–12. doi: 10.1093/humrep/dem046. [DOI] [PubMed] [Google Scholar]
- 5.Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med. 2012;9:e1001356. doi: 10.1371/journal.pmed.1001356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ganguly S, Unisa S. Trends of infertility and childlessness in India: Findings from NFHS data. Facts Views Vis Obgyn. 2010;2:131–8. [PMC free article] [PubMed] [Google Scholar]
- 7.Allow AK, Sadek SM, Maryam B. distribution of infertility factors among infertile couples in Yemen. J Clin Dev Biol. 2016;1:3. [Google Scholar]
- 8.Farhi J, Ben-Haroush A. Distribution of causes of infertility in patients attending primary fertility clinics in Israel. Isr Med Assoc J. 2011;13:51–4. [PubMed] [Google Scholar]
- 9.Masoumi SZ, Parsa P, Darvish N, Mokhtari S, Yavangi M, Roshanaei G. An epidemiologic survey on the causes of infertility in patients referred to infertility center in Fatemieh hospital in Hamadan. Iran J Reprod Med. 2015;13:513–6. [PMC free article] [PubMed] [Google Scholar]
- 10.Johnson JA, Tough S SOGC GENETICSCOMMITTEE. Delayed child-bearing. J Obstet Gynaecol Can. 2012;34:80–93. doi: 10.1016/S1701-2163(16)35138-6. [DOI] [PubMed] [Google Scholar]
- 11.Pal M, Devgun P, Chalana H, Kaur H, Biswas A, Sen S. A study of prevalence and socio-demographic profile of infertile couples in field practice area of a tertiary care centre, Amritsar, Punjab, India. International Journal of Community Medicine and Public Health. 2017;3:1472–6. [Google Scholar]
- 12.Mittal A, Yadav S, Yadav SS, Bhardwaj A, Kaur R, Singh P, et al. An epidemiological study of infertility among urban population of Ambala, Haryana. Int J Interdiscip Multidiscip Stud. 2015;2:124–30. [Google Scholar]
- 13.Patel A, Sharma PS, Narayan P, Binu VS, Dinesh N, Pai PJ. Prevalence and predictors of infertility-specific stress in women diagnosed with primary infertility: A clinic-based study. J Hum Reprod Sci. 2016;9:28–34. doi: 10.4103/0974-1208.178630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rajashekar L, Krishna D, Patil M. Polycystic ovaries and infertility: Our experience. J Hum Reprod Sci. 2008;1:65–72. doi: 10.4103/0974-1208.44113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Stewart-Smythe GW, van Iddekinge B. Lessons learned from infertility investigations in the public sector. S Afr Med J. 2003;93:141–3. [PubMed] [Google Scholar]
- 16.Chiamchanya C, Su-Angkawatin W. Study of the causes and the results of treatment in infertile couples at thammasat hospital between 1999-2004. J Med Assoc Thai. 2008;91:805–12. [PubMed] [Google Scholar]
- 17.Elussein EA, Magid YM, Omer MM, Adam I. Clinical patterns and major causes of infertility among Sudanese couples. Trop Doct. 2008;38:243–4. doi: 10.1258/td.2007.070125. [DOI] [PubMed] [Google Scholar]
- 18.Foroozanfard F, Sadat Z. Diagnostic value of hysterosalpingography and laparoscopy for tubal patency in infertile women. Nurs Midwifery Stud. 2013;2:188–92. doi: 10.5812/nms.10661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Verma I, Sood R, Juneja S, Kaur S. Prevalence of hypothyroidism in infertile women and evaluation of response of treatment for hypothyroidism on infertility. Int J Appl Basic Med Res. 2012;2:17–9. doi: 10.4103/2229-516X.96795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Adiga SK, Jayaraman V, Kalthur G, Upadhya D, Kumar P. Declining semen quality among South Indian infertile men: A retrospective study. J Hum Reprod Sci. 2008;1:15–8. doi: 10.4103/0974-1208.38972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lotti F, Maggi M. Ultrasound of the male genital tract in relation to male reproductive health. Hum Reprod Update. 2015;21:56–83. doi: 10.1093/humupd/dmu042. [DOI] [PubMed] [Google Scholar]
- 22.Sharma R, Harlev A, Agarwal A, Esteves SC. Cigarette smoking and semen quality: A new meta-analysis examining the effect of the 2010 World Health Organization laboratory methods for the examination of human semen. Eur Urol. 2016;70:635–45. doi: 10.1016/j.eururo.2016.04.010. [DOI] [PubMed] [Google Scholar]
- 23.Fritz MA, Speroff L. Clinical Gynaecologic Endocrinology and Infertility. 8th ed. New Delhi: Wolters Kluwer Health – Lippincott Williams & Wilkins; 2011. Induction of eovulation; pp. 1293–330. [Google Scholar]
- 24.Gelbaya TA, Potdar N, Jeve YB, Nardo LG. Definition and epidemiology of unexplained infertility. Obstet Gynecol Surv. 2014;69:109–15. doi: 10.1097/OGX.0000000000000043. [DOI] [PubMed] [Google Scholar]