
Figure 3.
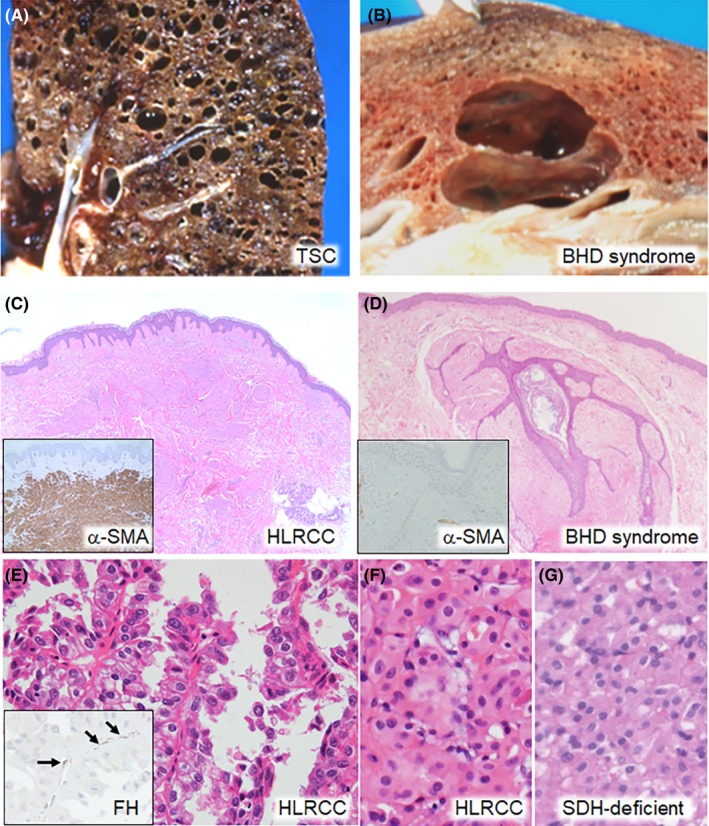
Differential diagnosis between Birt‐Hogg‐Dubé (BHD) syndrome and other hereditary diseases. A, Gross section of the lung of a 28‐year‐old woman with tuberous sclerosis complex. Numerous round cysts are observed in a diffuse arrangement. B, Gross section of the lung of an 81‐year‐old man with BHD syndrome. Two oval cysts extend along the interstitial tissue in a back to back way, compressing the alveolar structures between them. C, Histology of the skin tumor of a 75‐year‐old woman with hereditary leiomyomatosis and renal cell cancer (HLRCC). Proliferation of piloleiomyoma cells is observed in the dermic layer. Inset: immunostaining of α‐smooth muscle actin (α‐SMA). Tumor cells show diffuse staining. D, Histology of the skin tumor of a 54‐year‐old man with BHD syndrome. Proliferation of basaloid epithelial cells around a hair follicle and surrounding fibrous tissue is observed, which is consistent with fibrofolliculoma. Inset: immunostaining of α‐SMA. Fibrous tissue is negative. E, Histology of HLRCC‐associated RCC in a 49‐year‐old man. Type 2 papillary RCC with a high nuclear grade is observed. Inset: immunostaining of fumarate hydratase (FH). Capillary endothelial cells show FH staining (arrows), but the tumor cells are negative. F, G, Histology of HLRCC‐associated RCC in a 57‐year‐old man (F) and SDH‐deficient RCC in a 40‐year‐old man (G). Both patients were diagnosed by genetic testing. Oncocytic tumor cells are arranged in a solid sheet‐like pattern. They were indistinguishable from oncocytomas by H&E staining alone