
Figure 4.
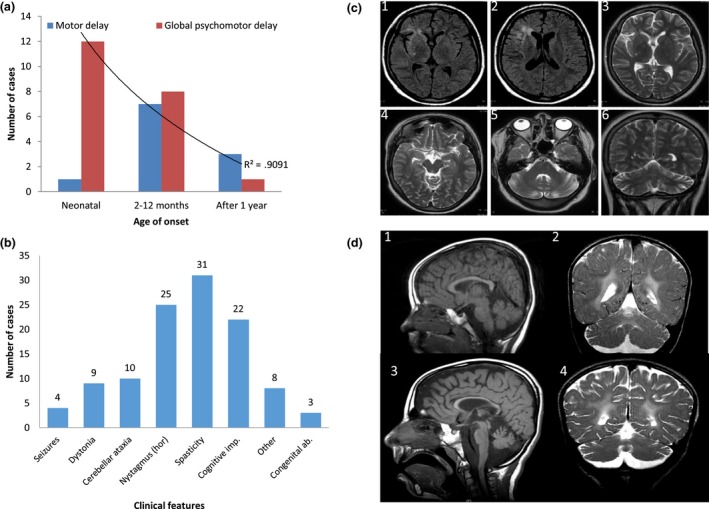
Genetype–phenotype correlation and neuroimaging spectrum of NKX6‐2 mutations. (a) The neonatal‐onset group has a statistically significant higher frequency of global psychomotor developmental delay (red) compared with the other two groups (onset from 2 months to 1 year and onset after 1 year). Childhood onset is associated with predominantly motor delay (blue). P = 0.05, r 2 = 0.9. (b) Clinical features associated with NKX6‐2 mutations (the horizontal axis) with the number of cases on the vertical axis (total n = 33). hor, horizontal gaze‐evoked nystagmus. (c) Fluid‐attenuated inversion recovery and T2‐weighted MRI acquisitions from case F1‐III:1 exhibiting T2 hyperintense signal change in periventricular WM surrounding the frontal horn of the right lateral ventricle, and frontal and temporal opercular and subinsular WM T2‐weighted hyperintense signal change associated with a degree of cortical volume loss. Note the normal signal intensity of the globi pallidi, thalami and external capsules, mesencephalon and pons. There is disproportionate cerebellar volume loss with mild T2‐weighted hyperintense signal change in the peri‐dentate WM. (d) Longitudinal MRI in case F7‐II:3 at ages of 4 years (D1, D2) and 8½ years (D3, D4) (D1, D3, mid‐sagittal T1‐weighted; D2, D4, coronal T2‐weighted) showing progressive thinning of the corpus callosum and cerebellar atrophy associated with WM abnormality sparing the U fibres (2, 4). There is progressive enlargement of the cortical sulci and extra axial cerebrospinal fluid spaces indicating underlying global brain atrophy.