
Fig. 2.
Cell surface and soluble CD163 are significantly increased among people living with HIV with opioid-use disorders and hepatitis C or B co-infection.
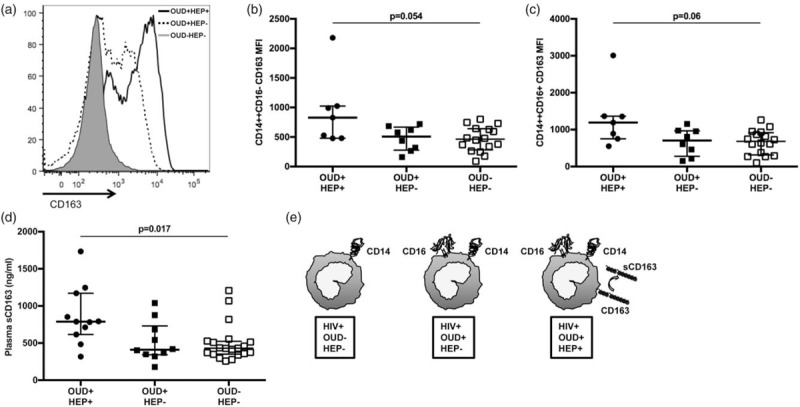
CD163 expression was analyzed on CD14++CD16−, CD14++CD16+ and CD14dimCD16+ monocytes using flow cytometry among individuals in OUD+/HEP+, OUD+/HEP−, and OUD−/HEP− cohorts. Data from three representative individuals are displayed as a histogram with mean fluorescence intensity (MFI) of CD163 on CD14++CD16− monocytes, on the x-axis (a). Shown are unadjusted medians with interquartile ranges of CD163 MFI on classical (b) and intermediate (c) monocytes. Soluble CD163 (sCD163; ng/ml) in the plasma of OUD+/HEP+, OUD+/HEP−, and OUD−/HEP− participants was quantified using a standard ELISA (medians with interquartile ranges displayed; d). P values to assess for differences among three cohorts were calculated using Kruskal--Wallis test. Adjusted analysis examining differences between OUD+/HEP+ vs. OUD−/HEP−, OUD+/HEP− vs. OUD−/HEP−, and OUD+/HEP+ vs. OUD+/HEP−, are shown in Table 2. A model illustrating the phenotypic differences among monocytes from OUD+/HEP+, OUD+/HEP−, and OUD−/HEP− participants is shown in panel (e). HEP, hepatitis C or B co-infection; OUD, opioid-use disorders.