

Abstract
Although performing exercise studies in patients with neuromuscular disorders (NMD) is difficult, the number of randomized controlled trials is steadily increasing. There is growing evidence for a positive effect of aerobic exercise in several NMD, on the other hand, the evidence for the effect of strength training is still scarce. Many NMD patients are captured in a vicious circle of physical inactivity, and it is important to let patients adhere to an active lifestyle, in order to prevent further chronic cardiovascular and muscle deconditioning and increased cardiovascular health risks. Exercise has to be prescribed as if it is medicine, in order to increase the adherence of patients and to optimize the efficacy of the intervention. Exercise in NMD is safe, although for some metabolic myopathies there is a contraindication for strenuous exercise. In NMD known to affect cardiac muscle, it is usually safe to exercise, but the consultation of a cardiologist is advised. Based on recent research, an increase in physical activity of moderate intensity and of sufficient duration, i.e. a physically active lifestyle, could be at least as effective and relevant as physical training. Underlying mechanisms of effect of exercise could be the influence of epigenetic mechanisms and the anti-inflammatory effect of exercise, but further studies are needed to confirm these hypotheses.
Key words: neuromuscular disorders, exercise, physical activity
Introduction
Scientific research regarding exercise in neuromuscular disorders
There are several limitations to consider when reviewing training studies in neuromuscular disorders (NMD). First of all, there are very few randomized controlled trials, each small in sample size. Second, studies are not immediately comparable because the training protocols often differ regarding the intensity and duration of the training, targeted muscle groups, type of strength or aerobic training, i.e. isometric or isokinetic, high or low intensity, and type of controls. The majority of exercise training studies have evaluated non-supervised home programs of relatively short duration, using submaximal, low-intensity training levels. The short duration of most studies does not allow differentiation between neural training effects versus muscle fiber hypertrophy and a real increase of aerobic capacity, which generally occurs after six weeks. Third, the compliance of patients, especially during non-supervised home protocols, is a possible confounding factor in all training studies. Fourth, because of the scarcity of patients of each NMD, studies have often grouped together several disorders. Persons with different types of NMD may however respond very differently to exercise (1). Fifth, some studies used the contralateral non-exercised muscle as a control in muscle strengthening interventions (2-4). The problem with this study design is that there may be confounding cross-over effect in the non-exercised muscles. Moreover, one can hardly expect meaningful effects of a single-limb training program on a patient’s activities, participation and well-being (1).
Altogether, scientific research regarding the effect of training in NMD is still scarce, but steadily growing. In 2013, a Cochrane review was published on aerobic training and strength training in muscle diseases (5). Only five randomized clinical trials (RCTs) met the inclusion criteria. The other studies were not randomized or used a healthy control group. The authors of the Cochrane review concluded that strength training in facioscapulohumeral muscular dystrophy (FSHD) and myotonic dystrophy did not show any positive, but also no negative effect. A combination of strength training and aerobic training is not harmful and shows a positive effect on aerobic capacity in patients with mitochondrial myopathy.
In 2004, a Cochrane review on training in patients with peripheral neuropathy appeared (6). Only one study was included in this review (7). This study in 34 patients with Charcot-Marie-Tooth (CMT) consisted of 24 weeks of isokinetic strength training of hip extension and knee extension and showed an improvement on the isokinetic knee extension force. Also, the required time for the 6-meter walk test decreased significantly. The authors of the Cochrane review conclude that there is little evidence for training in peripheral neuropathies, but that there is some evidence for strength training in CMT.
In 2013, a Cochrane review was published on training for Amyotrophic Lateral Sclerosis (ALS) and motor neuron disorders (8). In this Cochrane review, two trials were included that grouped the results of “endurance exercise” (unspecified) of limbs and thoracic muscles in 25 ALS patients (9) and strength training of arms and legs in 27 ALS patients (10). A significant improvement on the Amyotrophic Lateral Sclerosis Functional Rating Scale was observed after 3 months. There was no improvement in quality of life (measured with the SF-36), fatigue (measured with the Fatigue Severity Scale) or isokinetic and isometric muscular strength. No adverse reactions were reported. The general conclusion is that the numbers of patients in these studies are too small to be able to extrapolate the results to the general population.
After the appearance of these Cochrane reviews, more (large) RCTs have been published on exercise in NMD. The “No Use is Disuse” study describes a positive effect of cycling training with dynamic support on the functioning of boys with Duchenne, measured with the Motor Function Measure (MFM) (11). After 24 weeks, the MFM score had remained stable in the training group while it had dropped in the control group. No adverse effects of the training were found. The mechanism by which training could oppose the physical deterioration in children with a NMD is still unclear. Muscle fibers in NMD patients are abnormally vulnerable to contraction-induced injury due to the absence, or lack, of mechanical reinforcement of the sarcolemmal membrane (12). Eccentric exercises should therefore be avoided (13).
Three recently published RCTs in FSHD show a positive effect of cycling training on respectively aerobic capacity, walking speed, muscular strength, fatigue and of High Intensity Interval training on aerobic capacity (14-16). Fitness and strength training have a positive effect of on aerobic capacity and quality of life in polymyositis and dermatomyositis (17).
The Dutch FACTS-2-NMD study included three RCTs on the effect of cognitive behavioral therapy (CBT) and aerobic exercise in respectively ALS (18), post-polio syndrome (19) and FSHD (20, 21). An increase in the degree of physical activity was part of the CBT intervention. The FACTS-2-FSHD study studied the effect of 16 weeks of cycling training or CBT (including an activity module) in 57 patients with FSHD and severe chronic fatigue (22). After both cycling training and CBT patients were less fatigued and physically more active. After CBT, there was an increase in quality of life, the patients found themselves more active and the sleep quality improved. Approximately 80% of the participants in both intervention groups remained active even after the study. MRI measurements of the thigh showed a deceleration of the increase in fatty infiltration, after both cycling exercises and CBT, compared to the control group.
In contrary to the effect of cycling training and CBT, after 16 weeks of CBT or physical training in patients with Post-polio syndrome, no effect was seen on any outcome measure (19). The reason for the absence of effect is not yet known. No differences were found in fatigue-related cognitions between patients with Post-polio syndrome and patients with FSHD (23).
Recently, the results of the FACTS-2-ALS study were published. In this trial, 16 weeks of cycling training and usual care was not superior to usual care alone in preserving health related quality of life in ambulatory ALS patients. However, the study was unfortunately underpowered, because only 10 patients completed the protocol. The authors concluded that cycling training and usual care may preserve disease-specific health related quality of life in slow progressors.
Data from the “OPTIMISTIC” study, in which severely fatigued adult patients with myotonic dystrophy type 1 were included showed that, by month 10, cognitive behavioral therapy increased patients’ capacity for activity and participation, compared with standard care alone. Additionally, several secondary outcome measures of fatigue (Checklist Individual Strength, subscale fatigue and the fatigue and daytime sleepiness scale), exercise capacity (6-min walk test), and objective physical activity as measured with accelerometry were significantly improved with cognitive behavioral therapy compared with standard care alone (24). However, improvements in outcome measures for quality of life and disease burden were not significantly different between groups at 10 months. It should be noted that the trial was not powered for any of the secondary outcome measures except the 6-min walk test.
Strength training
The studies that have been conducted on strength training have been small, usually with mixed intervention groups and often without control groups (5, 25). The results of these studies must therefore be interpreted with caution. The aim of strength training is to maintain existing strength or reduce the progression of muscle weakness, and not necessarily to strengthen the affected muscles (26). Any increase in muscle strength is probably the result of effects on muscles that are relatively unaffected by the neuromuscular disease, but which may be deconditioned as a result of inactivity. Low intensity strength training (10-15 repetitions) may be beneficial for persons with sufficient muscle strength to move against gravity (27). There is no evidence that heavy strength training has additional beneficial effects beyond those of moderate exercise, and such training should therefore be avoided as it may lead to overloading of muscles (27). Heavy eccentric strength training is not recommended either for the same reason (28). The latter is also thought to be a frequent cause of serious muscle injury in those without NMD. Studies of limb girdle muscular dystrophy, FSHD, myotonic dystrophy type 1 and mitochondrial myopathies have shown that moderate strength training is safe and can have an impact on muscle strength and endurance, but results vary (27-29). Although studies generally point towards beneficial effects of moderate strength training, there is not yet sufficient evidence to make general recommendations for patients with NMD (5, 25). Major individual differences are seen in the intensity of training that can be tolerated, both between patients with different muscle diseases and among those with the same genetic disease variant.
Vicious circle of inactivity
When a training program is created, it is necessary to take into account various factors, among which are the diagnosis, the progressiveness of the condition, the condition of the heart and lungs, complaints of fatigue and pain, age, past and current activity level, kinesiophobia, the availability of exercise tools and lack of facilities. Sometimes it is necessary first of all to overcome kinesiophobia. Kinesiophobia is often based on years of belief that training is harmful to muscles. Many patients with NMD are captured in a vicious circle of inactivity (see Figure 1). Due to fatigue, patients often alter their lifestyles and reduce their activities. Low physical activity levels may lead to even greater weakness and atrophy of skeletal muscles, which causes a vicious circle of disuse and weakness. Physical inactivity in turn can lead to chronic cardiovascular and muscle deconditioning and increased cardiovascular health risks (30). For example, the average maximal oxygen uptake is abnormally low in patients with NMD (31). Body-composition measurements in NMD patients by various methods indicate reduced fat-free mass and increased adiposity in these patients relative to able-bodied control subjects of comparable ages and body weights (32, 33). The excess body fat of NMD patients additionally impairs mobility and further increases the risk of cardiovascular disease.
It is important to break this circle with training and encouraging an active lifestyle, especially in patients with no cardiac or pulmonary co-morbidity, such as in patients with FSHD.
Exercise in neuromuscular disorders is safe
In the past, clinicians were reluctant to prescribe exercise to patients with NMD. They often referred to possible muscle damage due to overuse. However, this hypothesis has never been proven with thorough research. Because of the weakness of the muscle membrane there is concern about the potentially damaging effects of eccentric and high-intensity muscle contractions during strength training. In animal models of NMD, there is evidence that eccentric contractions, known to stress muscle fibers, cause greater cell injury to these dystrophic muscle fibers. Although transferring results from animal studies to humans must be done with caution, eccentric training studies in NMD patients are so far being avoided. For some metabolic myopathies there is a contraindication for strenuous exercise. In lipid myopathy, rhabdomyolysis and myoglobulin may occur during training or strenuous exercise due to a defect in intramitochondrial transport and the use of fatty acids or glycogen. Cardiac involvement is common in some NMD. These include many muscular dystrophies (Duchenne, Becker and Emery-Dreyfuss muscular dystrophies, myotonic dystrophy types 1 and 2, limb-girdle muscular dystrophy types 1B, 2C-F, 2G and 2I) and certain congenital myopathies (34). Cardiac involvement may manifest as cardiomyopathy or cardiac arrhythmias. Training is always contraindicated in left ventricular/aortic outflow obstruction, threatening arrhythmias and cordial congestion. However, recent studies now also show a positive effect of training on the chance of survival and quality of life in patients with heart failure. In cases of known or suspected cardiac involvement, therefore, it is important for the patient to be monitored by a cardiologist irrespective of whether or not they have symptoms. In NMD known to affect cardiac muscle, it is usually safe to exercise, but advice on physical activity must be given after consultation with a cardiologist and preferably following a cardiac examination (34).
Exercise is medicine
What proved to be impossible in drug trials up to now did succeed in research using behavioral and exercise interventions. In FSHD and myotonic dystrophy, aerobic exercise training as well as CBT did not only reduce the degree of disease burden, but also established a beneficial effect at the muscular level probably as a result of increased physical activity. The question arises whether the “number needed to treat” and the (minor) side effect profile based on the FACTS-2-FSHD trial can be achieved with medication in future studies (35). Nevertheless, the scientific acceptance of exercise as medicine in NMD is still difficult. There is still uncertainty (and even scepsis) with regard to the underlying mechanisms. The acceptance of functionally targeted interventions can possibly be accelerated by providing more evidence for underlying mechanisms through basic research. However, the biggest challenge is to get the scientific and clinical world moving forward. This requires a societal change. A change in lifestyle requires a greater effort from patients and practitioners than taking or prescribing a drug. And even medication adherence is limited (36). In CBT, therapy sessions are usually structured by a collaboratively agreed-on agenda. Homework sessions encourage active participation. And during aerobic exercise training, patients exercise at home in addition to supervised training. Research has shown that a patient-centered approach improves treatment adherence in chronic patients and also improves job satisfaction in health professionals (37).
Guidelines for prescribing exercise in neuromuscular disorders
Currently, evidence-based exercise prescriptions do not exist for patients with NMD. Both patients and clinicians experience difficulties in preparing training programs (38). The recommendations for an effective aerobic exercise program by the American College of Sports Medicine are difficult to adhere to by many patients with NMD: 20 to 60 minutes aerobic exercise, 3 to 5 days per week at an intensity of 40 to 85% of the heart-rate reserve (39).
Furthermore, regular exercise tests cannot always be applied. Due to reduced muscular strength, it is often not possible to achieve the theoretical maximum heart rate and a maximal exercise test is less suitable to determine the training intensity. Recently an article has been published that describes that the anaerobic threshold in patients with post-polio syndrome could be determined by a submaximal exercise test in nearly 80% of the participants. If the anaerobic threshold cannot be determined, the authors advise to work with a Borg scale (40).
Both patients and practitioners experience difficulties in drawing up training schedules. Voorn et al evaluated the current application of aerobic exercise in adult neuromuscular rehabilitation in a cross-sectional survey (41). All respondents (n = 52) prescribed aerobic exercise and in a wide variety of NMD, mostly applying sessions of more than 20 min, two days per week, over a period of 9-16 weeks, using different exercise modes and methods to target intensity. The majority (81%) agreed that aerobic exercise should be incorporated into neuromuscular rehabilitation. However, all respondents perceived barriers to the application of aerobic exercise in one or more domains, and 77% of the respondents indicated needing support to improve application of this type of training, mostly with respect to screening procedures (54%) and dosing of exercise programs (48%).
The results of the FACTS-2-FSHD and OPTIMISTIC study and the experiences of the physiotherapists showed that the Borg scale, the talk test (which means that one can carry on a light conversation while exercising), and the rule that activities of daily life should not be negatively influenced by the exercise program are useful indicators for a proper exercise intensity (42). Previous research from Canada has shown that, in clinical practice, the exercise intensity is frequently determined based on simple tests such as the response of participants to the training, the Borg scale and/or the talk test (43).
In any case, to maintain the highest possible compliance, it is recommended to prescribe exercise as medicine with a clear description of exercise duration, frequency, intensity, location and supervision, and to search for a physical activity that the patient prefers. The barriers that patients still experience when exercising such as costs, shame for their limitations, and lack of facilities should be taken into account (44). It is for a reason that the FSHD lifestyle guide refers to “one has to move, if possible. “It is important to realize that a patient does not always have to exercise. The results of the FACTS-2-FSHD study emphasize the relevance of a physically active lifestyle. Ideally, an intervention for the improvement of chronic fatigue would no longer be needed. When adherence to a physically active lifestyle is already recommended shortly after the diagnosis, and physical activity and exercises are maintained, a patient may not be caught in a downward spiral as a result of physical inactivity.
Physical activity versus physical training
During CBT, a reliable increase in physical activity is an important part of the treatment. Aerobic exercise training focuses primarily on physical exercise, for example on an ergometer. At first sight, physical activity and physical exercise seem to be similar, but on second thought they are substantially different. Physical activity is defined as “any effort of skeletal muscles resulting in higher energy consumption than in resting conditions (45)”. Physical (aerobic) exercise is a form of physical activity and is defined as “planned, structured and repetitive exercises with an increasing magnitude and intensity in order to maintain or improve physical fitness or aerobic capacity (45)”.
The recommendations on physical activity for the healthy population have been prescribed in the Dutch Standard for Healthy Exercise (Nederlandse Norm Gezond Bewegen; NNGB). This standard aims at a physically active lifestyle and comprises a total of 30 minutes of exercise of moderate intensity (at a slightly higher heart and respiration rate than usual) of at least 4.0 MET a day, in blocks of at least 10 minutes at least five days a week.
The MET value or the metabolic equivalent is a unit of measurement within physiology expressing the amount of energy for a certain physical effort compared with the amount of energy required at rest. One MET (metabolic equivalent) corresponds to the resting metabolic rate, the amount of energy consumed during inactivity. One MET is equivalent to 3.5 ml of oxygen per kg of body weight per minute. The NNGB leads to a total duration of 150 minutes of physical activity per week of 4.0 MET, which implies a total increase of 450 MET per week compared to a physically inactive lifestyle. Physical activity within the NNGB includes not only sports activities but also daily-life activities such as household activities, cycling or walking the dog.
For physical exercise, the Dutch government has issued a standard for physical fitness. This standard is aimed primarily at maintaining aerobic capacity through physical exercise and requires intense physical activity of at least 6.0 MET for at least 20 minutes and at least three times a week. Although the intensity is higher than in the NNGB, the total length and the increase in MET per week is less, namely 300 MET. Thus, one can still have a physically inactive or sedentary lifestyle, in spite of meeting the standard for physical fitness. In other words, the NNGB leads to a higher level of physical activity than the Dutch standard for physical fitness.
The Dutch standard for physical fitness and the NNGB are defined only for healthy adults and for healthy elderly. The minimum standard for patients with a chronic disease, including FSHD, has not yet been defined. The NNGB not only leads to a higher level of physical activity; this standard is probably also more feasible for patients with FSHD, because daily-life activities are included. In other progressive neurological diseases, such as Parkinson’s disease, there is already growing evidence for a positive effect of decreasing the sedentary time (46). The question now arises whether physical exercise of minimum intensity and an increase in aerobic capacity are really necessary for the treatment of fatigue in patients with NMD. Would an increase in physical activity of moderate intensity and of sufficient duration, i.e. a physically active lifestyle, not be much more relevant?
Underlying mechanisms of effect of exercise and physical activity
Both CBT and aerobic exercise slow down the progression of fatty replacement of muscle tissue in FSHD. This raises the question: “How is it possible that an increase in physical activity causes a beneficial effect at the muscular level?” Epigenetics and the inflammation theory can possibly offer an explanation.
FSHD is a genetic disorder. More than 95% of cases of FSHD are associated with the absence of certain pieces of DNA at the end of chromosome 4 (genetic location: 4q35), the so-called D4Z4 deletion. This results in expression of the harmful DUX4 gene and production of a toxic protein (DUX4) that causes dystrophy (fatty replacement) of the skeletal muscles (47). The conversion of DNA into functional products for the cell, such as proteins, is dependent on both the DNA code itself (genetics) as well as on factors that may affect the activity of genes (gene expression), so-called epigenetic factors (48, 49). Epigenetic phenomena determine the “open” or “closed” state of parts of the genome and, thus, control the “on” or “off” position of genes. This can take place by means of changes in methylation, RNA molecules (intermediates between DNA and protein), or by the so-called histone proteins that are involved in the packing (and hence access) of the DNA in the chromosomes. FSHD is, therefore, an epigenetic disease (49). In FSHD patients, the degree of methylation of the DNA influenced by epigenetic factors plays an important role. Sometimes a small molecule group is added to the DNA, a so-called methyl group, which carries additional information. FSHD patients with a D4Z4 deletion (FSHD-1) show a decreased methylation of the D4Z4 region on the chromosomes 4q and 10q.
However, the degree of methylation is not already determined at birth. It varies between persons and may change under the influence of environmental factors during one’s lifetime.
Epigenetic factors ensure that the genetic defect in different people, even within families, can be expressed differently (50). In recent research, the difference in severity of the disease within families with FSHD is, among other phenomena, attributed to epigenetic factors (51).
An increase in physical activity and/or physical exercise can cause changes in the DNA methylation of healthy persons (52). It is possible that a physically active lifestyle is an epigenetic factor for FSHD and can slow down the progression of fatty replacement of muscle tissue by changes in DNA methylation. It is not a coincidence that the perpetuating factors of fatigue, i.e. physical inactivity, sleep disorders and pain, are known epigenetic factors (53). The degree of methylation can be different for every individual cell under the influence of epigenetic factors. This could be an explanation for the differences in effect on the fatty replacement between different muscles of patients with FSHD after CBT and aerobic exercise, as measured by quantitative magnetic resonance imaging (MRI) (54). To conclude, the first hypothesis is that AET as well as CBT influence the fatty replacement of muscle tissue by modifying epigenetic mechanisms.
A second explanation can perhaps be found in the beneficial effect of physical activity on inflammation. Inflammatory reactions seem to play a role in the increase in fatty replacement of muscle tissue in patients with FSHD and also in the development of chronic experienced fatigue in various neurological disorders (55). In approximately 5% of the muscles of patients with FSHD, edema has been observed using MRI(54, 56). There is evidence that an increase in edema is preceded by inflammation and is followed by fatty replacement of the muscle tissues (57, 58). The inhibition of inflammatory reactions could, therefore, theoretically slow down the progression of the disease. In healthy people, the anti-inflammatory effect of physical activity has already been proven extensively (59). Not only immune cells produce molecules that play a role in inflammatory responses (cytokines). Skeletal contracting muscles also release significant amounts of interleukin IL-6. IL-6 is a pro-inflammatory cytokine, in this situation also called a myokine. IL-6 causes inflammation when it is excreted as a cytokine by immune cells, but fights inflammation when it is released as a myokine by muscle cells. This is most likely because other cytokines are not produced anymore and another, “healthier” environment has been created (60, 61). In healthy adults, the production of IL-6 during exercise is for at least 50% related to the intensity and duration of the exercise (62, 63) To conclude, the second hypothesis is that aerobic exercise and CBT influence the fatty replacement of muscle tissue by positively influencing inflammatory reactions. This again argues in favor of a physically active lifestyle beyond physical exercise of limited duration.
To summarize, the evidence regarding the effect of aerobic exercise and a physically active lifestyle in NMD is increasing. However, there is still a strong need for a more tailored approach, in order to increase the magnitude of effect.
Figures and tables
Figure 1.
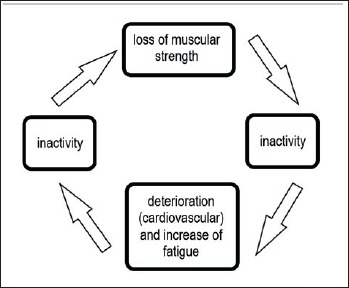
The vicious circle of inactivity. It is important to break this circle with training and encouraging an active lifestyle, especially in patients with no cardiac or pulmonary co-morbidity, such as in patients with FSHD.
Footnotes
Conflict of interest
The Author declare to have no conflict of interest.
References
- 1.Fowler WMJ. Role of physical activity and exercise training in neuromuscular diseases. Am J Phys Med Rehabil 2002;81(Suppl 11):S187-95. [DOI] [PubMed] [Google Scholar]
- 2.Aitkens SG, McCrory MA, Kilmer DD, et al. Moderate resistance exercise program: its effect in slowly progressive neuromuscular disease. Arch Phys Med Rehabil 1993;74:711-5. [DOI] [PubMed] [Google Scholar]
- 3.Kilmer DD, McCrory MA, Wright NC, et al. The effect of a high resistance exercise program in slowly progressive neuromuscular disease. Arch Phys Med Rehabil 1994;75:560-3. [PubMed] [Google Scholar]
- 4.Tollback A, Eriksson S, Wredenberg A, et al. Effects of high resistance training in patients with myotonic dystrophy. Scand J Rehabil Med 1999;31:9-16. [PubMed] [Google Scholar]
- 5.Voet NB, van der Kooi EL, Riphagen II, et al. Strength training and aerobic exercise training for muscle disease. Cochrane Database Syst Rev 2013;7:CD003907. [DOI] [PubMed] [Google Scholar]
- 6.White CM, Pritchard J, Turner-Stokes L. Exercise for people with peripheral neuropathy. Cochrane Database Syst Rev 2004;(4):CD003904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lindeman E, Leffers P, Spaans F, et al. Strength training in patients with myotonic dystrophy and hereditary motor and sensory neuropathy: a randomized clinical trial. Arch Phys Med Rehabil 1995;76:612-20. [DOI] [PubMed] [Google Scholar]
- 8.Dal Bello-Haas V, Florence JM. Therapeutic exercise for people with amyotrophic lateral sclerosis or motor neuron disease. Cochrane Database of Syst Rev 2008. April 16;(2):CD005229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Drory VE, Goltsman E, Reznik JG, et al. The value of muscle exercise in patients with amyotrophic lateral sclerosis. J Neurol Sci 2001;191:133-7. [DOI] [PubMed] [Google Scholar]
- 10.Bello-Haas VD, Florence JM, Kloos AD, et al. A randomized controlled trial of resistance exercise in individuals with ALS. Neurology 2007;68:2003-7. [DOI] [PubMed] [Google Scholar]
- 11.Jansen M, van Alfen N, Geurts AC, et al. Assisted bicycle training delays functional deterioration in boys with duchenne muscular dystrophy: the randomized controlled trial “no use is disuse”. Neurorehabil Neural Repair 2013;27:816-27. [DOI] [PubMed] [Google Scholar]
- 12.Petrof BJ. The molecular basis of activity-induced muscle injury in Duchenne muscular dystrophy. MolCell Biochem 1998;179:111-23. [DOI] [PubMed] [Google Scholar]
- 13.Lim JH, Kim DY, Bang MS. Effects of exercise and steroid on skeletal muscle apoptosis in the mdx mouse. Muscle Nerve 2004;30:456-62. [DOI] [PubMed] [Google Scholar]
- 14.Andersen G, Prahm KP, Dahlqvist JR, et al. Aerobic training and postexercise protein in facioscapulohumeral muscular dystrophy: RCT study. Neurology 2015;85:396-403 [DOI] [PubMed] [Google Scholar]
- 15.Andersen G, Heje K, Buch AE, et al. High-intensity interval training in facioscapulohumeral muscular dystrophy type 1: a randomized clinical trial. J Neurol 2017;264:1099-106. [DOI] [PubMed] [Google Scholar]
- 16.Bankolé LC, Millet GY, Temesi J, et al. Safety and efficacy of a 6-month home-based exercise program in patients with facioscapulohumeral muscular dystrophy: a randomized controlled trial. Medicine 2016;95:e4497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Alexanderson H, Munters LA, Dastmalchi M, et al. Resistive home exercise in patients with recent-onset polymyositis and dermatomyositis – A randomized controlled single-blinded study with a 2-year followup. J Rheumatol 2014;41:1124-32. [DOI] [PubMed] [Google Scholar]
- 18.van Groenestijn AC, Schröder CD, van Eijk RPA, et al. Aerobic exercise therapy in ambulatory patients with ALS: a randomized controlled trial. Neurorehabil Neural Repair 2019;33:153-64. [DOI] [PubMed] [Google Scholar]
- 19.Koopman FS, Voorn EL, Beelen A, et al. No reduction of severe fatigue in patients with post-polio syndrome by exercise therapy or cognitive behavioral therapy: results of an RCT. Neurorehabil Neural Repair 2016;30:402-10. [DOI] [PubMed] [Google Scholar]
- 20.Voet N, Bleijenberg G, Hendriks J, et al. Both aerobic exercise and cognitive-behavioral therapy reduce chronic fatigue in FSHD: an RCT. Neurology 2014;83:1914-22. [DOI] [PubMed] [Google Scholar]
- 21.Janssen B, Voet N, Geurts A, et al. Quantitative MRI reveals decelerated fatty infiltration in muscles of active FSHD patients. Neurology 2016;86:1700-7. [DOI] [PubMed] [Google Scholar]
- 22.Voet NB, Bleijenberg G, Padberg GW, et al. Effect of aerobic exercise training and cognitive behavioural therapy on reduction of chronic fatigue in patients with facioscapulohumeral dystrophy: protocol of the FACTS-2-FSHD trial. BMC Neurol 2010;10:56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Koopman FS, Brehm MA, Beelen A, et al. Cognitive behavioural therapy for reducing fatigue in post-polio syndrome and in facioscapulohumeral dystrophy: a comparison. J Rehabil Med 2017;49:585-90. [DOI] [PubMed] [Google Scholar]
- 24.Okkersen K, Jimenez-Moreno C, Wenninger S, et al. Cognitive behavioural therapy with optional graded exercise therapy in patients with severe fatigue with myotonic dystrophy type 1: a multicentre, single-blind, randomised trial. Lancet Neurol 2018;17:671-80. [DOI] [PubMed] [Google Scholar]
- 25.Gianola S, Pecoraro V, Lambiase S, et al. Efficacy of muscle exercise in patients with muscular dystrophy: a systematic review showing a missed opportunity to improve outcomes. PLoS One 2013;8:e65414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Johnson LB, Florence JM, Abresch RT. Physical therapy evaluation and management in neuromuscular diseases. Phys Med Rehabil Clin N Am 2012;23:633-51. [DOI] [PubMed] [Google Scholar]
- 27.Abresch RT, Han JJ, Carter GT. Rehabilitation management of neuromuscular disease: the role of exercise training. J Clin Neuromuscular Dis 2009;11:7-21. [DOI] [PubMed] [Google Scholar]
- 28.Siciliano G, Simoncini C, Giannotti S, et al. Muscle exercise in limb girdle muscular dystrophies: pitfall and advantages. Acta Myol 2015;34:3-8. [PMC free article] [PubMed] [Google Scholar]
- 29.Anziska Y, Inan S. Exercise in neuromuscular disease. Semin Neurol 2014;34:542-56. [DOI] [PubMed] [Google Scholar]
- 30.McDonald CM. Physical activity, health impairments, and disability in neuromuscular disease. Am J Phys Med Rehabil 2002;81(Suppl 11):S108-20. [DOI] [PubMed] [Google Scholar]
- 31.Lewis SF, Haller RG. Skeletal muscle disorders and associated factors that limit exercise performance. Exerc Sci Rev 1989;17:67-113. [PubMed] [Google Scholar]
- 32.Kilmer DD, Abresch RT, McCrory MA, et al. Profiles of neuromuscular diseases. Facioscapulohumeral muscular dystrophy. Am J Phys Med Rehabil 1995;74(Suppl 5):S131-9. [DOI] [PubMed] [Google Scholar]
- 33.Johnson ER, Abresch RT, Carter GT, et al. Profiles of neuromuscular diseases. Myotonic dystrophy. Am J Phys Med Rehabil 1995;74(Suppl 5):S104-16. [PubMed] [Google Scholar]
- 34.Finsterer J, Stöllberger C. Heart disease in disorders of muscle, neuromuscular transmission, and the nerves. Korean Circ J 2016;46:117-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Vina J, Sanchis-Gomar F, Martinez-Bello V, et al. Exercise acts as a drug; the pharmacological benefits of exercise. Br J Pharmacol 2012;167:1-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Haynes RB, McDonald H, Garg AX, et al. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev 2002;(2):CD000011. [DOI] [PubMed] [Google Scholar]
- 37.Michie S, Miles J, Weinman J. Patient-centredness in chronic illness: what is it and does it matter? Patient Educ Couns 2003;51:197-206. [DOI] [PubMed] [Google Scholar]
- 38.Nierse CJ, Abma TA, Horemans AM, et al. Research priorities of patients with neuromuscular disease. Disabil Rehabil 2013;35:405-12. [DOI] [PubMed] [Google Scholar]
- 39.Garber CE, Blissmer B, Deschenes MR, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sport Exerc 2011;43:1334-59. [DOI] [PubMed] [Google Scholar]
- 40.Borg G. Perceived exertion as an indicator of somatic stress. Scand J Rehabil Med 1970;2:92-8. [PubMed] [Google Scholar]
- 41.Voorn E, Koopman F, Nollet F, et al. Aerobic exercise in adult neuromuscular rehabilitation: a survey of healthcare professionals. J Rehabil Med 2019;51:518-24. [DOI] [PubMed] [Google Scholar]
- 42.Reed JL, Pipe AL. The talk test: a useful tool for prescribing and monitoring exercise intensity. Curr Opin Cardiol 2014;29:475-80. [DOI] [PubMed] [Google Scholar]
- 43.Doyle L, Mackay-Lyons M. Utilization of aerobic exercise in adult neurological rehabilitation by physical therapists in Canada. J Neurol Phys Ther 2013;37:20-6. [DOI] [PubMed] [Google Scholar]
- 44.Phillips M, Flemming N, Tsintzas K. An exploratory study of physical activity and perceived barriers to exercise in ambulant people with neuromuscular disease compared with unaffected controls. Clin Rehabil 2009;23:746-55. [DOI] [PubMed] [Google Scholar]
- 45.Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Heal Rep 1985;100:126-31. [PMC free article] [PubMed] [Google Scholar]
- 46.van der Kolk NM, van Nimwegen M, Speelman AD, et al. A personalized coaching program increases outdoor activities and physical fitness in sedentary Parkinson patients; a post-hoc analysis of the ParkFit trial. Park Relat Disord 2014;20:1442-4. [DOI] [PubMed] [Google Scholar]
- 47.Salani M, Morini E, Scionti I, et al. Facioscapulohumeral muscular dystrophy: from clinical data to molecular genetics and return. In: Zaher A, Ed. Neuromuscular disorders. Intech Open 2012. [Google Scholar]
- 48.Jirtle RL, Skinner MK. Environmental epigenomics and disease susceptibility. Nat Rev Genet 2007;8:253-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Daxinger L, Tapscott SJ, van der Maarel SM. Genetic and epigenetic contributors to FSHD. Curr Opin Genet Dev 2015;33:56-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Neguembor MV, Gabellini D. In junk we trust: repetitive DNA, epigenetics and facioscapulohumeral muscular dystrophy. Epigenomics 2010;2:271-87. [DOI] [PubMed] [Google Scholar]
- 51.Tawil R, van der Maarel SM, Tapscott SJ. Facioscapulohumeral dystrophy: the path to consensus on pathophysiology. Skelet Muscle 2014;4:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Barrès R, Yan J, Egan B, et al. Acute exercise remodels promoter methylation in human skeletal muscle. Cell Metab 2012;15:405-11. [DOI] [PubMed] [Google Scholar]
- 53.Skinner MK. Environmental stress and epigenetic transgenerational inheritance. BMC Med 2014;12:153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Janssen BH, Voet NB, Nabuurs CI, et al. Distinct disease phases in muscles of facioscapulohumeral dystrophy patients identified by MR detected fat infiltration. PLoS One 2014;9:e85416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gandevia SC. Spinal and supraspinal factors in human muscle fatigue. Physiol Rev 2001;81:1725-89. [DOI] [PubMed] [Google Scholar]
- 56.Friedman SD, Poliachik SL, Carter GT, et al. The magnetic resonance imaging spectrum of facioscapulohumeral muscular dystrophy. Muscle Nerve 2012;45:500-6. [DOI] [PubMed] [Google Scholar]
- 57.Friedman SD, Poliachik SL, Otto RK, et al. Longitudinal features of stir bright signal in FSHD. Muscle Nerve 2014;49:257-60. [DOI] [PubMed] [Google Scholar]
- 58.Frisullo G, Frusciante R, Nociti V, et al. CD8(+) T Cells in facioscapulohumeral muscular dystrophy patients with inflammatory features at muscle MRI. J Clin Immunol 2011;31:155-66. [DOI] [PubMed] [Google Scholar]
- 59.Gleeson M, Bishop NC, Stensel DJ, et al. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol 2011;11:607-15. [DOI] [PubMed] [Google Scholar]
- 60.Pedersen L, Hojman P. Muscle-to-organ cross talk mediated by myokines. Adipocyte 2012;1:164-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Petersen AM, Pedersen BK. The anti-inflammatory effect of exercise. J Appl Physiol 2005;98:1154-62. [DOI] [PubMed] [Google Scholar]
- 62.Pedersen BK, Steensberg A, Schjerling P. Muscle-derived interleukin-6: possible biological effects. J Physiol 2001;536:329-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiol Rev 2008;88:1379-406. [DOI] [PubMed] [Google Scholar]