

Abstract
Papillary thyroid carcinoma with nodular fasciitis-like stroma (PTC-NFS) is a rare lesion with dual pathological features, that behaves more aggressively if positive for β-catenin gene (CTNNB1) mutations. Recently, we encountered a recurrent PTC-NFS with CTNNB1 mutations. A 48-year-old female presented with a recurrent enlarging tumor with a diagnosis of desmoid-type fibromatosis 6 months after her initial operation for PTC-NFS. Over a 2-year observation period, she underwent remedial surgery to resect the recurrent tumor. During the operation, the left recurrent laryngeal nerve was engulfed and scarified. Local invasion, β-catenin aberrant staining, and CTNNB1 mutations were detected both in the primary tumor stroma and the recurrent tumor. This case indicates that CTNNB1 mutation screening and β-catenin staining should be performed in PTC-NFS cases as a predictor for recurrence. If either of these are positive, a wider surgical resection should be adopted to achieve negative margins. Otherwise, radiotherapy should be considered. Furthermore, the lesion might be better known as papillary thyroid carcinoma with desmoid-type fibromatosis in such situations to reflect its local aggressive nature.
Keywords: Papillary thyroid carcinoma, desmoid tumor, desmoid-type fibromatosis, CTNNB1 mutations, β-catenin aberrant staining
Introduction
Papillary thyroid carcinoma with nodular fasciitis-like stroma (PTC-NFS) is a rare variant of PTC that accounts for only 0.17%-0.5% of all cases [1]. It is synonymous with PTC with fibromatosis-like stroma (PTC-FMS) [2], and both terminologies refer to the two intermingled components of the lesion: the predominant mesenchymal element resembling nodular fasciitis or fibromatosis, and the minor epithelial part that is characteristic of PTC [3]. To date, no more than 30 cases have been documented, and only one of these shown to have mutations in the β-catenin gene (CTNNB1) of the mesenchymal component [4]. Herein, we present a recurrent case of PTC-NFS with CTNNB1 mutations that is newly described.
Case report
A 48-year-old female with no remarkable personal or familial medical history developed an enlarging recurrent tumor in her left thyroid bed 6 months after an initial operation for a T4aN0M0 PTC-NFS in her left thyroid lobe (Figure 1A). The initial operation was a total thyroidectomy plus prophylactic ipsilateral central neck dissection with fine preservation of the recurrent laryngeal nerves (RLN) and parathyroid glands. During the operation, the primary tumor was found to have seriously infiltrated surrounding tissues of the lesion.
Figure 1.
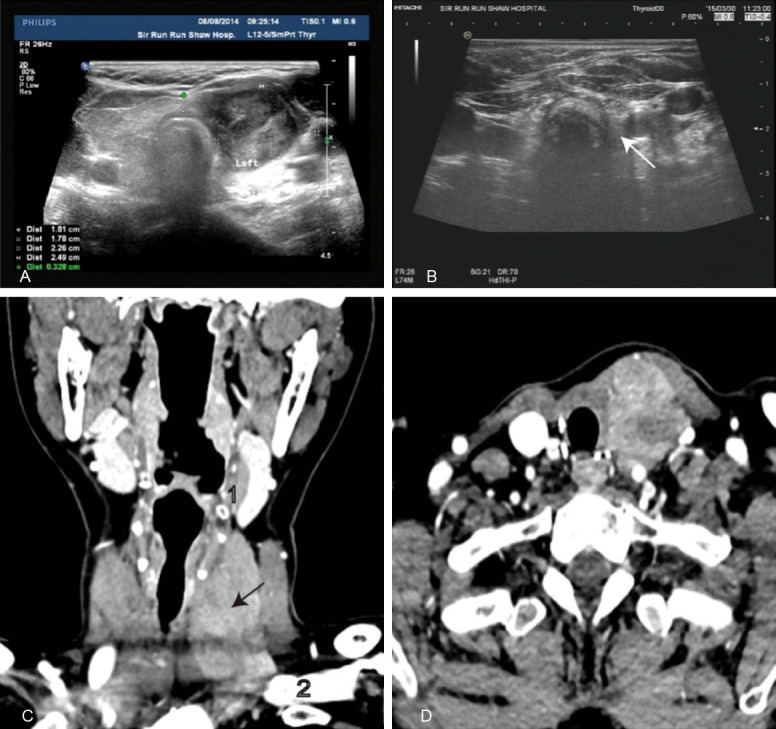
A. Ultrasound image of the primary tumor showing an irregular hypo-echo mass (3.46 × 2.04 cm) in the left thyroid lobe. B. Ultrasound image of the recurrent tumor (white arrow) 6 months after the initial operation. An irregular hypo-echo mass (1.2 × 0.67 cm) with ill-defined margins is shown. C. Computed tomography (CT) image of the recurrent tumor (black arrow) 1 month before the second operation. The tumor is superior to the hyoid bone1, and inferior to the innominate vein2. D. CT cross section of the recurrent tumor showing the shift in muscles and cervical vessels.
Both frozen section and routine pathological diagnoses were PTC-NFS. Radioactive iodine (RAI) therapy with 100 mCi was administered 3 months later, although functional scans revealed a negative or faint uptake in the thyroid bed. After the initial therapy, the patient accepted regular thyroid stimulating hormone (TSH) suppression, in which TSH levels were maintained between 0.05-2.05 IU/ml. Thyroglobulin antibody levels were continuously declining from 354.15 to 5.45 IU/ml with a negative thyroglobulin level.
The recurrent tumor, which had grown from 1.2 cm to 4.54 cm, was monitored by a series of ultrasound examinations for 2 years (Figure 1B). The tumor was diagnosed as a recurrence because cytology revealed it to consist of spindle cells, which were the main cellular component of the primary tumor. An enhanced computed tomography scan was outlined the lesion before the remedial operation, and revealed that the tumor had shifted the strap muscles and main cervical vessels (Figure 1C and 1D). During the remedial operation, the tumor was found to be fixed to the strap muscles, trachea, and esophagus; it had also adhered to the carotid artery, internal jugular vein, and vagus, and had engulfed the left RLN. An extended resection of the tumor that invaded the muscles and the parathyroid glands was performed with a sharp dissection of the trachea, esophagus, main cervical vessels, and vagus, while the left RLN was sacrificed. Both frozen section and pathological diagnoses of the recurrent tumor were desmoid-type fibromatosis. The patient refused radiotherapy, and is currently free of disease.
Histologically, the primary tumor consisted of a minor epithelial component harboring typical features of PTC, and a predominant mesenchymal component harboring features of desmoid-type fibromatosis (Figure 2A, 2B and 2E). The mesenchymal component separated and surrounded the epithelial component into small nodules, and was composed of an exuberant proliferation of spindle cells arranged in bundles of fascicles with abundant fibrous tissue. The recurrent tumor exhibited a homogeneous histological appearance of desmoid-type fibromatosis that was similar to the mesenchymal component of the primary tumor (Figure 2C). Immunohistochemically, both the mesenchymal component of the primary tumor and the recurrent tumor expressed aberrant β-catenin nuclear staining and negative thyroglobulin staining, whereas the epithelial component of the primary tumor expressed normal cytoplasmic β-catenin staining with positive thyroglobulin staining (Figure 2D). Furthermore, a c.134C>T (p. S45F) mutation in exon 2 of CTNNB1 (reference sequence: NM_0019.4.3) was detected both in the mesenchymal component of the primary tumor and the recurrent tumor (Figure 2F).
Figure 2.
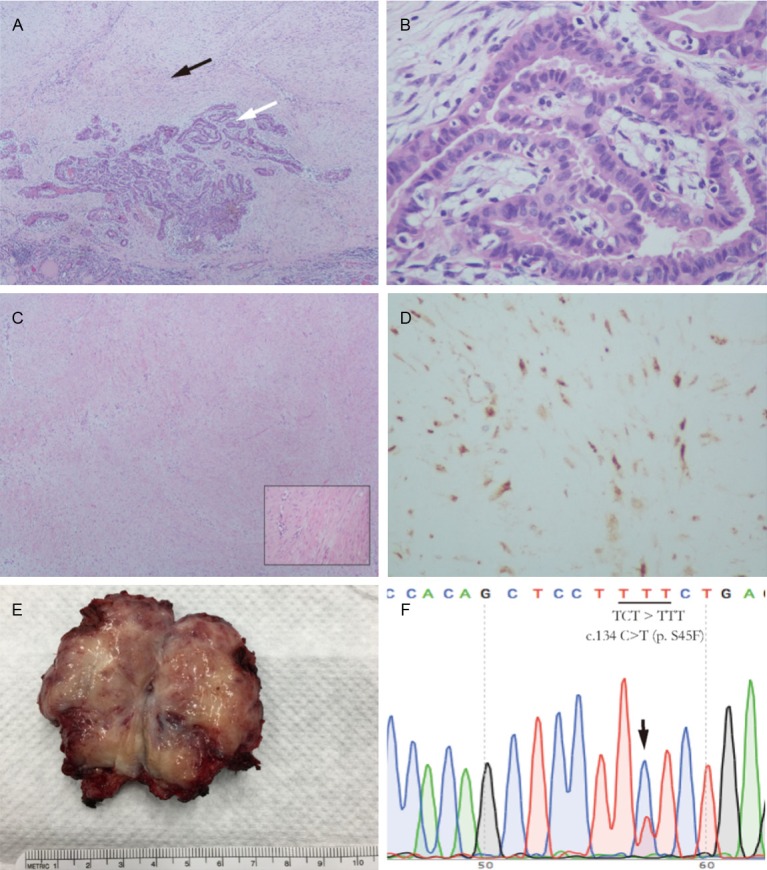
A. Overview of the primary tumor. The mesenchymal component (black arrow) surrounds and separates the epithelial component (white arrow) into small nodules (hematoxylin & eosin (HE) staining; magnification, 40×). B. The epithelial component of the primary tumor. Epithelial cells are arranged in a papillary architecture and show irregular, overlapping nuclei with disturbed polarity (HE staining; magnification, 400×). C. Overview of the recurrent tumor. Homogeneous fibrous cells with varying amounts of collagen (HE staining; magnification, 20×). Insert shows fibrous cells arranged in bundles or fascicles, with varying amounts of collagen (HE staining; magnification, 400×). D. β-catenin staining of the recurrent tumor. Aberrantly-stained nuclei and cytoplasmic staining of fibrous cells (magnification, 400×). E. Cut section of the recurrent tumor. Homogeneous, yellowish cut section (7.5 × 3.5 cm). F. CTNNB1 mutation analysis of the recurrent tumor: c.133C>T (p. S45F) mutation was detected in exon 2 of CTNNB1.
Discussion
In previous reports, the terms nodular fasciitis and fibromatosis were used interchangeably to describe the exuberant proliferated mesenchymal component of all lesions such as PTC-NFS and/or PTC-FMS because of their similar morphology, although they have different clinical courses [5,6]. Nodular fasciitis is a self-limited, spontaneously regressing lesion, while fibromatosis is a benign lesion with a recurrent tendency that is commonly referred to as desmoid-type fibromatosis or a desmoid tumor [7-9]. Mutations in exon 3 of CTNNB1, which are the main casue of aberrant β-catenin nuclear staining, are highly common in desmoid-type fibromatosis and desmoid tumors, and are closely associated with recurrence [10,11]. Some researchers have therefore suggested that PTC-NFS is not suitable terminology to refer to aberrant β-catenin staining [12]. In a recent study, the novel terminology ‘PTC with desmoid-type fibromatosis’ was used to rename these lesions with CTNNB1 mutations [4].
In the current case, the mesenchymal component of the primary tumor exhibited many clinicopathological features of desmoid-type fibromatosis, including local invasion, an exuberant proliferation of spindle cells, aberrant β-catenin staining, and recurrence [13]. It is possible that the unreported mutation in exon 2 of CTNNB1 causes these features, although further research is needed to confirm this [14]. Because the exact nature of the lesion had not yet been determined at the time of the initial operation, guidelines for PTC were followed [15]. However, once recurrence was detected, this suggested that advice for desmoid-type fibromatosis should be adhered to rather than PTC guidelines [16]. Additionally, RAI therapy, TSH suppression therapy, and biochemical surveillance appeared ineffective in the current case because the main component of the lesion did not derive from thyroid follicles. Therefore, both the diagnosis and therapeutic strategy for situations such as the current case should be revised and altered to match its dual nature, especially that of desmoid-type fibromatosis.
Complete surgical resection is the main therapy for desmoid-type fibromatosis, but this is difficult to achieve in the head and neck region while preserving complex and vital anatomy [7,8]. In cases of positive resection margins, radiotherapy should therefore be considered [17]. In most cases, including ours, the PTC component accounts for a minor part of the entire lesion and is usually inoffensive [14]. Hence, total thyroidectomy might not be necessary or suitable, although it was undertaken in our case with resection of the infiltrated tissues around the affected lobe to gain negative margins. We initially adopted the “wait and see” strategy after identifying the recurrent tumor, which is also advised by many experts [17]. However, continuous enlargement of the tumor and invasion of many important structures during the observation period implied that this policy was not suitable in our case.
In conclusion, aberrant β-catenin nuclear staining and/or CTNNB1 mutations should be assessed in cases of PTC-NFS and/or PTC-FMS. If either of these are positive, a much wider local resection should be performed to achieve complete resection. Otherwise, radiotherapy should be undertaken to decrease the likelihood of recurrence. Moreover, we propose that the terminology “PTC with desmoid-type fibromatosis” should be considered to reflect the local invasive nature of the lesion in such situations.
Acknowledgements
We thank Sarah Williams, PhD, from Liwen Bianji, Edanz Group China (www.liwenbianji.cn), for editing the English text of a draft of this manuscript.
Disclosure of conflict of interest
None.
References
- 1.Ginter PS, Scognamiglio T. Papillary thyroid carcinoma with nodular fasciitis-like stroma: a usual entity with distinctive morphology. Int J Surg Pathol. 2015;23:305–307. doi: 10.1177/1066896915570362. [DOI] [PubMed] [Google Scholar]
- 2.Mizukami Y, Kurumaya H, Kitagawa T, Minato H, Nonomura A, Michigishi T, Noguchi M. Papillary carcinoma of the thyroid gland with fibromatosis-like stroma: a case report and review of the literature. Mod Pathol. 1995;8:366–370. [PubMed] [Google Scholar]
- 3.Batsakis JG, Rice DH, Howard DR. The pathology of head and neck tumors: spindle cell lesions (sarcomatoid carcinomas, nodular fasciitis, and fibrosarcoma) of the aerodigestive tracts, Part 14. Head Neck Surg. 1982;4:499–513. doi: 10.1002/hed.2890040609. [DOI] [PubMed] [Google Scholar]
- 4.Rebecchini C, Nobile A, Piana S, Sarro R, Bisig B, Gerasimos SP, Saglietti C, Matter M, Marino L, Bongiovanni M. Papillary thyroid carcinoma with nodular fasciitis-like stroma and β-catenin mutations should be renamed papillary thyroid carcinoma with desmoid-type fibromatosis. Mod Pathol. 2017;30:236–245. doi: 10.1038/modpathol.2016.173. [DOI] [PubMed] [Google Scholar]
- 5.Chan JK, Carcangiu ML, Rosai J. Papillary carcinoma of thyroid with exuberant nodular fasciitis-like stroma. Report of three cases. Am J Clin Pathol. 1991;95:309–314. doi: 10.1093/ajcp/95.3.309. [DOI] [PubMed] [Google Scholar]
- 6.Mizukami Y, Nonomura A, Matsubara F, Michigishi T, Ohmura K, Hashimoto T. Papillary carcinoma of the thyroid gland with fibromatosis-like stroma. Histopathology. 1992;20:355–357. doi: 10.1111/j.1365-2559.1992.tb00994.x. [DOI] [PubMed] [Google Scholar]
- 7.Siegel NS, Bradford CR. Fibromatosis of the head and neck: a challenging lesion. Otolaryngol Head Neck Surg. 2000;123:269–275. doi: 10.1067/mhn.2000.107456. [DOI] [PubMed] [Google Scholar]
- 8.Martinez Trufero J, Pajares Bernad I, Torres Ramon I, Hernando Cubero J, Pazo Cid R. Desmoid-type fibromatosis: Who, when, and how to treat. Curr Treat Options Oncol. 2017;18:29. doi: 10.1007/s11864-017-0474-0. [DOI] [PubMed] [Google Scholar]
- 9.Dahl I, Jarlstedt J. Nodular fasciitis in the head and neck. A clinicopathological study of 18 cases. Acta Otolaryngol. 1980;90:152–159. doi: 10.3109/00016488009131711. [DOI] [PubMed] [Google Scholar]
- 10.Lazar AJ, Tuvin D, Hajibashi S, Habeeb S, Bolshakov S, Mayordomo-Aranda E, Warneke CL, Lopez-Terrada D, Pollock RE, Lev D. Specific mutations in the beta-catenin gene (CTNNB1) correlate with local recurrence in sporadic desmoid tumors. Am J Pathol. 2008;173:1518–1527. doi: 10.2353/ajpath.2008.080475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Saito T, Oda Y, Kawaguchi K, Tanaka K, Matsuda S, Tamiya S, Iwamoto Y, Tsuneyoshi M. Possible association between higher beta-catenin mRNA expression and mutated beta-catenin in sporadic desmoid tumors: real-time semiquantitative assay by TaqMan polymerase chain reaction. Lab Invest. 2002;82:97–103. doi: 10.1038/labinvest.3780399. [DOI] [PubMed] [Google Scholar]
- 12.Na KY, Kim HS, Sung JY, Park WS, Kim YW. Papillary carcinoma of the thyroid gland with nodular fasciitis-like stroma. Korean J Pathol. 2013;47:167–171. doi: 10.4132/KoreanJPathol.2013.47.2.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fisher C, Thway K. Aggressive fibromatosis. Pathology. 2014;46:135–140. doi: 10.1097/PAT.0000000000000045. [DOI] [PubMed] [Google Scholar]
- 14.Toti P, Tanganelli P, Schurfeld K, Stumpo M, Barbagli L, Vatti R, Luzi P. Scarring in papillary carcinoma of the thyroid: report of two new cases with exuberant nodular fasciitis-like stroma. Histopathology. 1999;35:418–422. doi: 10.1046/j.1365-2559.1999.035005418.x. [DOI] [PubMed] [Google Scholar]
- 15.American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–1214. doi: 10.1089/thy.2009.0110. [DOI] [PubMed] [Google Scholar]
- 16.Kasper B, Baumgarten C, Bonvalot S, Haas R, Haller F, Hohenberger P, Moreau G, van der Graaf WT, Gronchi A Desmoid Working Group. Management of sporadic desmoid-type fibromatosis: a European consensus approach based on patients’ and professionals’ expertise - a sarcoma patients EuroNet and European Organisation for Research and Treatment of Cancer/Soft Tissue and Bone Sarcoma Group initiative. Eur J Cancer. 2015;51:127–136. doi: 10.1016/j.ejca.2014.11.005. [DOI] [PubMed] [Google Scholar]
- 17.Al-Jazrawe M, Au M, Alman B. Optimal therapy for desmoid tumors: current options and challenges for the future. Expert Rev Anticancer Ther. 2015;15:1443–1458. doi: 10.1586/14737140.2015.1096203. [DOI] [PubMed] [Google Scholar]