
Figure 1.
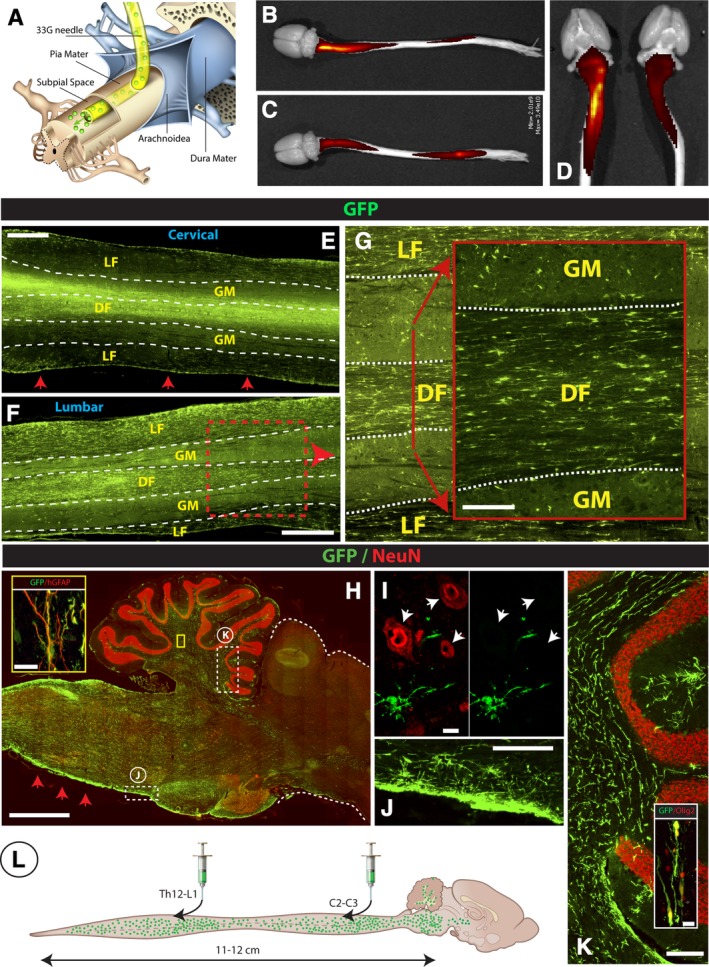
Spinal subpial injection of human GFP+ hNSCs leads to long‐term injected‐cell survival in the subpial space and intraparenchymal migration throughout the whole spinal cord, medulla, and white matter of the cerebellum in immunodeficient rats. A, Adult immunodeficient rats received a cervical and lumbar subpial injection of human fetal GFP+ hNSCs using a 33G subpial needle. At 6 months after cell delivery, animals were perfusion fixed, spinal cord and brain dissected, and imaged in situ using an IVIS Spectrum optical imaging system. After imaging, tissue was used for immunofluorescence staining of spinal cord and brain sections. B‐D, Surface GFP fluorescence seen in two individual rats (B, C) shows an intense GFP signal on the dorsal cervical and lumbar spinal cord. Similar GFP fluorescence on the ventral cervical spinal cord can be seen in the same animals (D). E‐G, A high density of GFP+ cells in the spinal cord parenchyma in horizontally cut spinal cord sections taken from the cervical (E) and lumbar (F) spinal cord can be identified. A relatively higher number GFP+ cells was seen in the white matter funiculi (LF, DF) if compared to gray matter (GM) (G). H‐K, Analysis of sagittal brain sections shows a high density of injected GFP+ cells in the medulla oblongata, in the vicinity of glia limitans (H‐red arrows; J) and the white matter tracts of the cerebellum (K). Similarly as seen in the spinal cord, the majority of GFP+ cells showed colocalization with Olig2 (K‐inset) and GFAP (H‐inset). 0.3 μm optical images showing no NeuN expression in injected GFP+ cells (I). L, Schematic drawing of spinal and brain GFP+ cell distribution at 6 months after cervical and lumbar subpial cell delivery. Scale bar: E, F, 1 mm; G, 150 μm; H, 2 mm; H‐inset, 15 μm; I, 10 μm; J, 200 μm; K, 200 μm; K‐inset, 15 μm, LF, DF‐lateral, and dorsal white matter funiculi, GM, gray matter