
Figure 1.
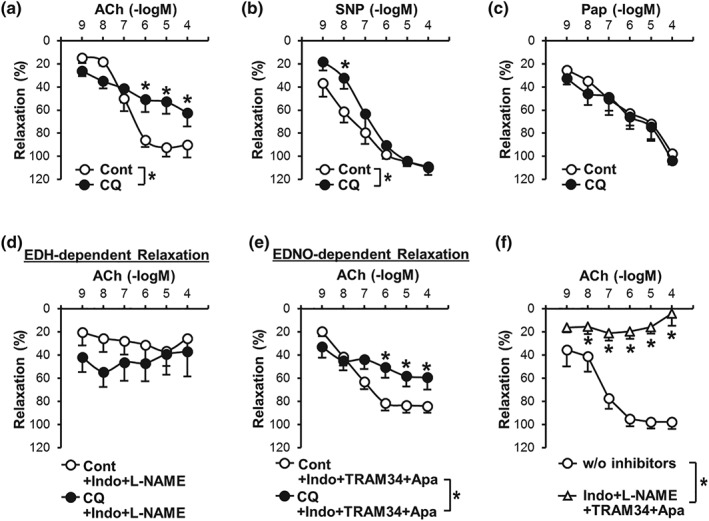
Endothelium‐dependent relaxation in coronary artery is attenuated by chloroquine. (a) Endothelium‐dependent relaxation (EDR) induced by ACh in the absence (Cont, open circle) or presence (CQ, closed circle) of chloroquine (CQ, 10 μM). n mice = 6 in each group. Data are mean ± SE. *P < .05 versus Cont. (b) Smooth muscle (SM)‐dependent relaxation induced by sodium nitroprusside (SNP, an NO donor) in the absence (Cont) or presence (CQ) of CQ. n mice = 7 in each group. (c) SM‐dependent relaxation induced by papaverine (Pap, a PDE inhibitor) in the absence (Cont) or presence (CQ) of CQ. n mice = 6 in each group. (d)Endothelium‐derived hyperpolarization (EDH)‐dependent relaxation in the absence (Cont) or presence (CQ) of CQ. EDH‐dependent relaxation was conducted by ACh administration in the presence of indomethacin (Indo, a COX inhibitor, 10 μM) and L‐NAME (an eNOS inhibitor, 100 μM). n mice = 8 in each group. (e) Endothelium‐derived NO (EDNO)‐dependent relaxation in the absence (Cont) or presence (CQ) of CQ. EDNO‐dependent relaxation was accessed by ACh administration in the presence of Indo, TRAM34 (an inhibitor of intermediate‐conductance Ca2+‐activated K+ channel, 100 nM), and apamin (an inhibitor of small conductance Ca2+ activated K+ channel, 100 nM). n mice = 13 in each group. (f) Pretreatment with Indo (to inhibit PGI2), L‐NAME (to inhibit NO), and TRAM34 and apamin (to inhibit EDH) abolishes ACh‐induced relaxation in coronary artery (CA). n mice = 8 in each group. *P < .05 compared to control (i.e., w/o inhibitors). Statistical comparison between dose–response curves was made by two‐way ANOVA with Bonferroni post hoc test