
Figure 5.
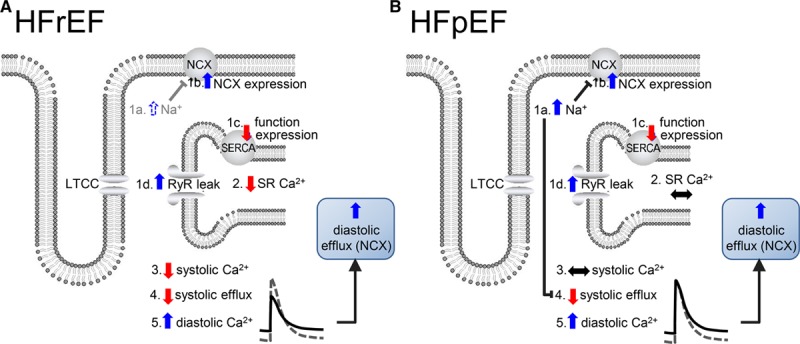
Speculative hypothesis to account for the difference in Ca2+ handling between heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF). A, HFrEF. B, HFpEF. In both panels, heart failure results in an increase in intracellular Na+ concentration ([Na+]i), 1a; increase in sodium-calcium exchange (NCX) expression, 1b; decrease in sarcoplasmic reticulum Ca-ATPase (SERCA) function or expression, 1c; increase in Ca2+ leak through ryanodine receptor (RyR), 1d. We assume that in A (HFrEF) 1b–1d dominate over 1a with the net result being a decrease of sarcoplasmic reticulum (SR) Ca2+ content (2) and systolic intracellular Ca2+ concentration ([Ca2+]I; 3), systolic efflux (4) and a consequent increase in diastolic [Ca2+]i (5), which (via NCX) raises diastolic efflux. In B (HFpEF), the increase in [Na+]i (1a) dominates over 1b-d so that SR Ca2+ content (2) and systolic [Ca2+]i (3) are unchanged. The increase in [Na+]i decreases NCX activity so that diastolic [Ca2+]i (5) has to increase to maintain systolic efflux (4) and flux balance. LTCC indicates L-type Ca channel.