

Abstract
Age estimation is one of the essential factors in human identification. Teeth bestowed with features such as hardness and resilience to external factors such as chemicals, putrefaction, and fire explosions serve as a durable source in age estimation. Concurrently, they present with peculiar and comparable features of age-associated regressive changes along with dental procedures, which make them a mirror reflection of age changes from cradle to the grave of an individual. Age estimation in adults poses an enigma to the forensic dentists because as the age advances, the dentitions get influenced by numerous exogenous and endogenous factors which may lead to discrepancies between dental age and chronologic age. Since 1950, many authors have presented various methods for assessing age of individuals above 18 years. Here is an overview of the different methods with their application and limitations along with a mention of newer methods developed and tested with the formulation of population-specific formulas by Indian authors. The data have been sourced from different journal articles retrieved through Google Scholar and PubMed Central and articles received as study materials during the fellowship program in forensic odontology using keywords such as age estimation, adult dentitions, dentin translucency, and cementum annulations.
Keywords: Age estimation, dental pulp, dentitions, forensic odontology, regressive changes
Introduction
The first known attempts of using teeth as an age indicator stem from England, when the Factory Act of 1837 verboten a child without a second permanent molar from working in factories. Upto this time, height was used for age determination. The first scientific study was presented in 1837 by Edwin Saunders, who after examining 1049 children's teeth and height, proved in parliament that teeth were more reliable guide of age than height and hence can be used in jurisprudence.[1]
Growth is a complex and dynamic process through which different physiologic systems such as skeletal system and dentition pass through a series of changes, eventually arriving at maturity. These changes are reflected in the teeth.[2] Human dentition is considered a hard tissue analog to fingerprints, making it unique to a particular individual.[3] Forensic odontologists are often referred for age determination of the unknown deceased and living individuals. Age estimation plays a vital role in the identification of unknown corpses and skeletal remains of accidents, crimes, and disaster victims.[4] Teeth are one of the strongest structures in the human body and usually survive postmortem destruction, thereby playing a vital role in comparative as well as reconstructive identification.[5] With the global increase in migration movements in recent years, age estimation is becoming pertinent for living individuals devoid of valid identification documents (exiles and adoption cases) to ascribe a genuine age for the course of criminal, civil, asylum, or old-age pension proceedings.[6] The International and Interdisciplinary “Study Group on Forensic Age Diagnostics” was constituted in Berlin on March 10, 2000, with the aim to develop a consensus among scientists about the most appropriate methods to be used in specific situations, drawing up recommendations for age estimation and institutionalizing quality control in this area.[6,7]
Methods of Age Estimation in Adults
Three categories are: (1) morphohistological methods, (2) radiological methods, and (3) biochemical methods.
Morphohistological methods: Morphologic criteria are observed in sectioned or unsectioned teeth.
In this category, the methods included are summarized in Table 1.
Table 1.
Summarized morphohistological methods of age estimation in adults
| Method | Year |
|---|---|
| Gustafson method | 1950 |
| Dalitz | 1962 |
| Bang and Ramm | 1970 |
| Johanson | 1971 |
| Maples | 1978 |
| Solheim | 1993 |
Gustafson's method
The first technique for age estimation based on the assessment of certain regressive alterations in teeth was given by Gosta Gustafson in 1947 and 1950. This method is a morphohistological method and is applicable on single-rooted teeth. The age changes are:
Attrition of the enamel (A)
Secondary dentin deposit (S)
Alteration/recession of periodontal ligament (P)
Cementum apposition (C)
Root resorption (R)
Transparency/translucency of dentin (T).
In the method proposed, each of these criteria was scored (n) ranging from 0, 1, 2, and 3 [Figures 1 and 2].[8] The grade value of each of the age change is then added which gives a total score (Y). The error of estimation in this method was ±3.6 years as calculated by Gustafson (1947).[8]
Figure 1.

“Gustafson's method (1950) point values” – scoring for regressive changes namely: Attrition, secondary dentin, periodontitis, cementum apposition, and root resorption
Figure 2.
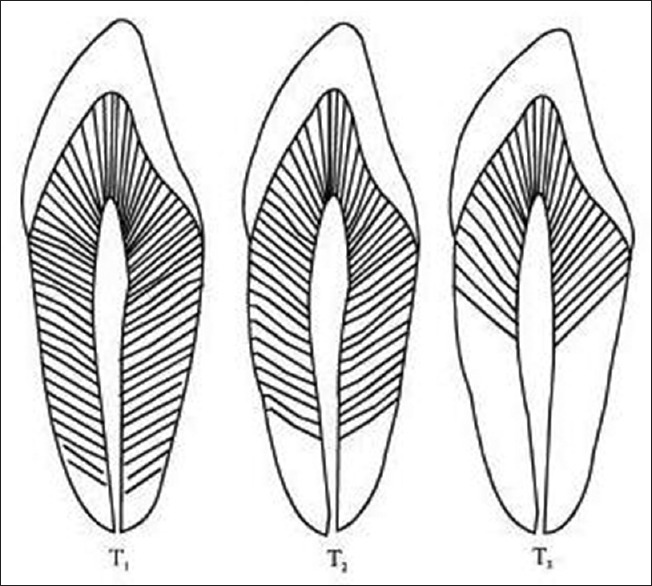
“Gustafson's method (1950)” – Scoring for root transparency where T1 = noticeable root transparency, T2 = root transparency extends over the apical third of the root, T3 = root transparency extends over the apical two-thirds of the root
An + Pn + Sn + Cn + Rn + Tn = total score (Y) (n = score of individual criteria)
An increase in total score (Y) corresponded linearly with increase in age. Age was estimated using the following equation:[8]
Age = 11.43 + 4.56 × Y (total score)
The limitations of Gustafson's method are:
It cannot be used in living individuals. The scoring is a subjective perception of the regressive changes. Multiple evaluations make it a time-consuming method. Periodontal ligament assessment is difficult in decomposed bodies. One regression line was given to all teeth irrespective of their eruption time and morphological differences. All the six criteria were given equal importance, ignoring any possibility of interrelationship between the criteria themselves. Training in dental histological techniques is essential.[7] In the Indian population, the age estimation error rate using Gustafson's method was found to be ±8.13 years.[9]
Dalitz improvised Gustafson's method with a 5-point system scoring from 0 to 4. Root resorption and secondary cementum criteria were discarded. The remaining four criteria for the 12 anterior teeth corresponded well with the age. This method excludes the use of posterior teeth. Use of upto four out of the 12 anterior teeth from one individual was recommended by Dalitz. The standard deviation in age estimated by this method is ±6 years. The limitation of Dalitz method is that it does not include premolars and molars which are more likely to be sustained in case of severe trauma or mass disasters.[10]
E’ =8.691 + 5.146A’ +5.338P’ + 1.866S’ + 8.411T’
Johanson proposed amendments in the Gustafson's method. He suggested seven grades (0, 0.5, 1, 1.5, 2, 2.5, and 3) for the same six criteria. A tooth section thickness of 0.25 mm was recommended for better evaluation of root transparency, and the following multiple regression formula was suggested:[11]
Age = 11.02 + (5.14 × A) + (2.3 × S) + (4.14 × P) + (3.71 × C) + (5.57 × R) + (8.98 × T)
Kashyap et al. amended Gustafson's technique by using objective measurements and omitted criteria such as gingival recession and root resorption.[12] However, Ajmal et al.'s[13] results suggest that method of Kashyap is inferior to that of Johanson. They attribute this to the difficulty in obtaining secondary dentin and cementum apposition measurements.
Maples suggested the use of only two criteria out of the original six Gustafson's criteria. These were secondary dentin deposit and root transparency. They eliminated the use of root resorption as it was found to be negatively correlated with age, periodontal status was excluded due to evaluation difficulties after soft-tissue decomposition, and varying influences of dietary and occlusal conditions led to elimination of enamel attrition. This exclusion enabled this method to be applied on teeth with broken crowns, populations of contemporary and prehistoric eras, and teeth with damaged cementum.[14]
Solheim studied 1000 teeth originating from diverse sources including cadavers and living individuals. He used five criteria suggested by Gustafson (attrition, secondary dentin, periodontal status, cementum apposition, and root translucency) and added three new criteria, namely surface roughness, tooth color, and sex. He recommended exclusion of mandibular canines and second premolars to avoid major errors in age estimation. The results also suggested cautious use of tooth color as a criterion for age estimation in deceased bodies because tooth color might get influenced by the change in environment post death. He proposed two sets of formulae, one including sex and color and the other without these criteria to be used in deceased individuals.[15]
Miles believed that root dentin translucency (DT) correlated most strongly with age among the six parameters used by Gustafson and when used alone, DT may serve as a single best parameter for age estimation.[1]
Bang and Ramm further developed Miles approach and presented it as a relatively simple, practical, inexpensive, and objective method. They found that as a response to any noxious stimuli, dentinal tubules started to become narrow and blocked due to the deposition of hydroxyapatite crystals and collagen fibers within the tubular lumen. The root dentin started becoming translucent during the third decade of life, beginning at the tip of the root and subsequently advancing coronally with age. The affected dentin appears translucent due to equalization of refractive indices between intratubular organic and extratubular inorganic material. This examination was carried out on both sectioned and unsectioned teeth. DT was measured using Vernier caliper. The results suggested a significant increase in DT with age. They also suggested that DT remains unaffected with the use of preservation media (e.g. formalin), extent of storage period, sex of individuals, or whether the source of teeth was a living or a dead individual. Contralateral teeth from the same individual showed very high correlation with age. However, they recommended exclusion of maxillary first premolars and all the molars for best age estimates. They presented two different equations, one for values of translucent length ≤9 mm and the other when this exceeds 9 mm.[16]
Stott et al. suggested that cemental annulations can serve as an accurate means of age determination in all nonhibernating mammals including humans. They suggested that these alternating light and dark lines were deposited in an annual rhythm, resembling annual rings of trees. These annulations could be studied on serial cross sections of stained human teeth under bright field microscope and the counted annulations provided a close estimate of age.[17] Renz and Radlanskim however, were very skeptical about the reliability of counting root cementum lines as a method of age estimation in humans.[18]
Tooth wear as a criterion for age estimation was used in living individuals by Kim et al. They proposed that a combined sum of area of tooth wear (horizontal factor) and extent of dentin exposure (vertical factor) could provide a better and reliable scoring system. Premolar and molar were used, and scoring was done from 0 to 8. However, the limitation of this method was the absolute necessity of sound and healthy teeth without any carious involvement or fractures for evaluation, which presents practical difficulty for its application in various populations. Overcoming these difficulties, the modified Kim's index was later introduced by Yun et al. who proposed a 10-point scoring scale (0–10) [Table 2]19 for all teeth except third molars, and this scoring could be done for decayed, filled, or missing teeth as well. The practical validity of this modified Kim's index was tested by Lu et al. in Chinese Malaysian adults and their results suggested good correlation between age and tooth wear with low standard error.[19]
Table 2.
Modified Kim’s index to score tooth wear
| Score | Premolar | Molar |
|---|---|---|
| 0 | No visible wear | |
| 1 | 1P/1L | 1P/1L/2P/2L |
| 2 | 2P/2L/1S/1B | 3P/3L/4P/4L/1S/1B/2S/2B |
| 3 | 2S/2B | 3S/3B/4S/4B |
| 4 | Wear on more than 2/3rd of occlusal surfaces | |
| 5 | 1Pc/1Lc | 1Pc/1Lc/2Pc/2Lc |
| 6 | 2Pc/2Lc/1Sc/1Bc | 3Pc/3Lc/4Pc/4Lc/1Sc/1Bc/2Sc/2Bc |
| 7 | 2Sc/2Bc | 3Sc/3Bc/4Sc/4Bc |
| 8 | Concavity on more than 2/3 of occlusal surfaces | |
| 9 | Filling, *caries, *crown (all teeth) | |
| 10 | Missing, stump of tooth, pontic, denture (all teeth) | |
*If the extent of the filling materials or caries does not exceed 1/3rd of the occlusal surface so that the degree of occlusal wear can be determined, the pertinent score should be given. c: Concavity, ca: Concavity area, P: Point-like wear facet less than ca. 1 mm in diameter, L: Linear wear facet less than ca. 1 mm in width, S: Surface-like wear facet greater than ca. 1 mm in diameter, B: Band-like wear facet greater than ca. 1 mm in width or wear facet involving more than two surface-like wear facets, Concavity: The wear of dentin; in the situation where a tooth has several different degrees of occlusal wear, the highest degree should be selected as the occlusal wear score
Li and Ji proposed a new clinical method of age estimation using permanent first and second molars. Attrition values of each molar cusp are recorded using the average stage of attrition (ASA) chart (stage 0–9) following which an average is calculated [Figure 3 and Table 3].[20] These values are substituted in a respective formula for first molar, second molar, and both the molars.[20]
Figure 3.
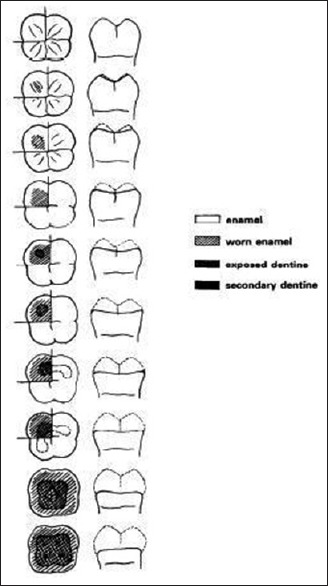
“Stages of crown attrition on molars from top to bottom: Stages 0–9” – the average stage of attrition is the average stage of the attrition on all cusps of a molar when evaluating the attrition degree from stages 0–7 for each cusp. The eighth and ninth stages of attrition are estimated from the attrition condition of the entire occlusal surface. The attrition degree is divided into ten stages
Table 3.
Average stage of attrition proposed by Li and Ji
| Stage | Inference |
|---|---|
| Stage 0 | No attrition. Cusp is sharp. Gullies and ridges are clear |
| Stage 1 | Slight attrition on the top and ridges of the cusp |
| Stage 2 | Cusp appears obtuse or a limited oblique facet appears on it |
| Stage 3 | The great part of cusp is worn away. The wear facet is depressed slightly or obviously and may connect with one or more other facets |
| Stage 4 | Dentine appears as a spot, in which the average diameter is ≤1 mm |
| Stage 5 | Dentine appears as a spot, in which the average diameter is >1 mm, and the attrition plane is level or sunk deeply |
| Stage 6 | One exposed dentine spot coalesces with another one and/or cusp is almost entirely worn away |
| Stage 7 | One exposed dentine spot coalesces with two others and/or cusp is entirely worn away |
| Stage 8 | Exposed dentine appears as a circle, and there is a small star-like island of enamel within it. The secondary dentine may also be exposed |
| Stage 9 | Dentine is exposed on the entire occlusal surface, and the secondary dentin has been exposed |
For maxillary molars:
Y = 11.42 + 6.32M1
Y = 14.44 + 7.44M2
-
Y = 12.23 + 4.11M1 +2.75M2
For mandibular molars:
Y = 12.76 + 6.30M1
Y = 15.31 + 7.27M2
Y = 13.63 + 3.98M1 +2.83M2.
In these equations, M is the attrition stage of the molar and Y is the estimated age. Ajmal et al. found ASA to be the best method for calculating age as compared to Johanson's and Kashyap's modified approach of Gustafson's method.[13]
Acharya described a new and comparatively simple method for capturing and quantifying refined measurements of dentinal translucency on sectioned teeth using commercially available hardware and software. The author also compared the results obtained by digital measurements with conventionally obtained measurements using a caliper. The results showed that the digital method could estimate age within ±5 years of actual age in 60% of age estimates as against 40% for caliper-based method, hence establishing the digital method to be more refined, better correlated to age, and producing superior age estimates. The author attributed these superior results to the improved measurements obtained under magnified view on digital images of thin tooth sections.[4]
Irregular junctions between translucent and nontranslucent zone pose a problem in determining actual translucency length. Lorentsen and Solheim found that translucency area correlated better with chronological age.[21] Acharya suggested a digital method for measuring area of root translucency in mm2, on tooth sections of 250-μm thickness. This method produced more accurate age estimates as compared with those of digital length measurements.[22]
Radiological methods
These nondestructive methods became popular because of their applicability in living and dead individuals as well as in archaeological studies or in certain judicial setups which prohibit tissue collection from human remains because they make use of dental radiographs, hence eliminating the requirement to extract or section the teeth. The size of dental pulp cavity gets reduced as a result of secondary dentin deposition, and measurement of this reduction could be used as an indicator of age.[23] Kvaal et al. proposed a method based on indirect measurement of secondary dentin deposition by measuring pulp radiolucency on periapical radiographs. Initially, only maxillary cuspids were used, but, later on, formulae for incisors, canines, and premolars were also developed. Pulp length and width along with root length and width were measured. The author proposed the number of length and width measurements of the tooth and pulp owing to magnification and angulation on the periapical radiograph.[24] This method is very useful in ascertaining whether a person in question is under 18 years of age or above. However, this method has its own limitations owing to its applicability in individuals having all the six teeth (maxillary central and lateral incisors, maxillary second premolars, mandibular lateral incisors, mandibular premolar, and mandibular canine). In addition, it cannot be applied if the teeth are rotated, attrited, carious, or associated with any periapical pathosis.[25]
Cameriere et al. put forth Italian formulae for the estimation of age using pulp and tooth area ratio (PTR) on maxillary and mandibular canines. They obtained high levels of accuracy in age prediction (mean error between 3 and 4.5 years) and advocated the effect of race and culture in model parameters.[26] Babshet et al. presented a customized formula for age estimation in Indian population using PTR. They used mandibular canine and measured PTR using commercially available software program. The Indian formula was: age = 64.413 – 195.265 × PTR. Their results ascertained the notion of Camerier et al. that population-specific formula markedly improves age prediction.[27]
The Coronal Pulp Cavity Index was introduced by Ikeda et al. in 1985. This method calculates the tooth coronal index (TCI) by measuring the length of coronal pulp cavity and length of tooth crown on the radiographs of incisors and molars using the following formula:
TCI = length of coronal pulp cavity height (CPCH) × 100/crown length (CL).
CPCH was measured vertically from cervical line to the tip of the highest pulp horn, and CL/height was measured from cervical line to the highest cusp tip. Using linear regression analysis, pulp cavity length was regressed on the real age.[28,29]
Radiographic assessment of developing third molars could provide a method of age assessment in individuals above 17 years of age. Harris and Nortje suggested five stages for root development in third molars along with analogous mean age and root length. The development of mesial root of third molar on panoramic radiographs was considered to estimate age by Van Heerden. The authors suggested five stages for this purpose.[30]
Yang et al. developed a new technique using cone-beam computed tomography (CT) scans to acquire the three-dimensional (3D) images of teeth in living individuals. Using these 3D images, the pulp/tooth area ratio could be calculated with promising results for age estimation.[31]
Cone-beam CT (CBCT) images of maxillary and mandibular canine were examined by Kazmi et al. on a homogenous sample (even distribution of age) of Pakistani population. Their results suggested mandibular canine pulp volumes as a good predictor for chronologic age estimation.[32]
A relatively simple, quicker, and reproducible method based on the analysis of narrowing of pulp chamber due to continued secondary dentin deposition on the CBCT images of maxillary central incisors was studied by Pinchi et al. They considered the ratio between pulp volume and the hard tissues volume (PHr) using the following formula:
PHr = VPulp/Vht
The ratio of dental volumes (PHr) was found to be a statistically significant predictor of chronological age estimation.[33] Their result was similar to the results reported by Gulsahi et al.[34] CBCT thus can be considered to be more convenient, cost-effective, and with lesser radiation exposure (45 μSv) as compared to the conventional multislice CT scans (429,7-1066 μSv).[33]
Recently, an automatic software program Dental Age Estimation® was developed which comprises of the most accurate and referable morphologic and radiological techniques, which have been reported in literature.[35] This software gives quick results in age estimation and has the advantage of automatic selection of the borders of pulp and tooth, hence reducing the time lapse and has less subjective error. It also allows application of different methods in a given case, thus providing a more reliable result.[36]
Spalding et al. suggested that the amount of radiocarbon present in tooth enamel is a remarkably accurate predictor of age. Before 1955, the amount of atmospheric C14 was static. It increased dramatically following the above-ground nuclear bomb test. Since the test Ban Treaty in 1963, atmospheric C14 has been dropping exponentially due to its incorporation in living tissues in the form of CO2 through food chain, and thus its concentration in human body closely parallels that in the atmosphere at any point of time. Enamel is a metabolically static tissue containing 0.4% carbon, and it forms at a distinct time for each tooth during childhood. The measured C14 content of enamel can be related to its known concentrations in the atmosphere in different years to establish the year of tooth formation, indirectly reflecting birth year of an individual. Although very sensitive, this technique, however, is not very popular yet, owing to restrained access to the instruments and need of expertise for exploring this field.[37]
Biochemical methods
These are based on racemization of aminoacids at a rapid rate in metabolically stable proteins such as enamel, dentin, and cementum. L-aspartic acid undergoes racemization to be stored as D-aspartic acid in increasing amounts during aging.[38]
Helfman and Bada proposed that ratio of D/L enantiomers in aspartic acid from the enamel and coronal dentin could be used to deduce the age of any stable protein from a long-lived mammal and thus the age of the organism itself.[39] Ohtani et al. were of a view that aspartic acid in dentin increases linearly with aging.[40]
Ritz et al. used racemization method in dentinal biopsy specimens (1 mm × 1 mm) obtained from molars of living individuals. The results showed a close relationship between the extent of aspartic acid racemization in dentinal biopsy specimens and age.[41]
Conclusion
Age estimation is an important and relatively recent area of forensic research. Numerous methods and studies have been put forward so far, each one having different applications, accuracy, and reliability. However, it must be considered that age estimates based on dental findings will be a representation of most likely age as compared with actual chronologic age. Ongoing research projects using the existing methods and formulae should be closely scrutinized, and new population-specific formulae must be derived in order to reduce the mean error rates in forensic workup. Interdisciplinary approach also must be practiced while approaching a case with questionable identity, which will enhance the contribution of forensic medicine and dentistry in legal jurisdiction.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors are grateful to Dr. Ashith B. Acharya for providing with the relevant literature for this article and for his able guidance.
References
- 1.Stavrianos C, Mastagas D, Stavrianou I, Karaiskou O. Dental age estimation of adults: A review of methods and principals. Res J Med Sci. 2008;2:258–68. [Google Scholar]
- 2.Miles AE. Dentition in the estimation of age. JDent Res. 1963;42:255–263. [Google Scholar]
- 3.Bowers CM. Forensic Dental Evidence-An Investigator's Handbook. San Diego, California: Elsevier Academic Press; 2004. p. 7. [Google Scholar]
- 4.Willems G, Moulin-Romsee C, Solheim T. Non-destructive dental-age calculation methods in adults: Intra- and inter-observer effects. Forensic Sci Int. 2002;126:221–6. doi: 10.1016/s0379-0738(02)00081-6. [DOI] [PubMed] [Google Scholar]
- 5.Acharya AB. A new digital approach for measuring dentin translucency in forensic age estimation. Am J Forensic Med Pathol. 2010;31:133–7. doi: 10.1097/PAF.0b013e3181cf328d. [DOI] [PubMed] [Google Scholar]
- 6.Schmeling A, Geserick G, Reisinger W, Olze A. Age estimation. Forensic Sci Int. 2007;165:178–81. doi: 10.1016/j.forsciint.2006.05.016. [DOI] [PubMed] [Google Scholar]
- 7.Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, et al. Criteria for age estimation in living individuals. Int J Legal Med. 2008;122:457–60. doi: 10.1007/s00414-008-0254-2. [DOI] [PubMed] [Google Scholar]
- 8.Gustafson G. Age determination on teeth. J Am Dent Assoc. 1950;41:45–54. doi: 10.14219/jada.archive.1950.0132. [DOI] [PubMed] [Google Scholar]
- 9.Pillai PS, Bhaskar GR. Age estimation from teeth using Gustafson's method – A study in India. Forensic Sci. 1974;3:135–41. doi: 10.1016/0300-9432(74)90022-3. [DOI] [PubMed] [Google Scholar]
- 10.Dalitz GD. Age determination of adult human remains by teeth examination. J Forensic Sci Soc. 1962;3:11–21. [Google Scholar]
- 11.Johanson G. Age determination from teeth. Odontol Rev. 1971;22:1–126. [Google Scholar]
- 12.Kashyap VK, Koteswara Rao NR. A modified Gustafson method of age estimation from teeth. Forensic Sci Int. 1990;47:237–47. doi: 10.1016/0379-0738(90)90293-8. [DOI] [PubMed] [Google Scholar]
- 13.Ajmal M, Mody B, Kumar G. Age estimation using three established methods. A study on Indian population. Forensic Sci Int. 2001;122:150–4. doi: 10.1016/s0379-0738(01)00501-1. [DOI] [PubMed] [Google Scholar]
- 14.Maples WR. An improved technique using dental histology for estimation of adult age. J Forensic Sci. 1978;23:764–70. [PubMed] [Google Scholar]
- 15.Solheim T. A new method for dental age estimation in adults. Forensic Sci Int. 1993;59:137–47. doi: 10.1016/0379-0738(93)90152-z. [DOI] [PubMed] [Google Scholar]
- 16.Bang G, Ramm E. Determination of age in humans from root dentin transparency. Acta Odontol Scand. 1970;28:3–5. doi: 10.3109/00016357009033130. [DOI] [PubMed] [Google Scholar]
- 17.Stott GG, Sis RF, Levy BM. Cemental annulation as an age criterion in forensic dentistry. J Dent Res. 1982;61:814–7. doi: 10.1177/00220345820610063401. [DOI] [PubMed] [Google Scholar]
- 18.Renz H, Radlanski RJ. Incremental lines in root cementum of human teeth – A reliable age marker? Homo. 2006;57:29–50. doi: 10.1016/j.jchb.2005.09.002. [DOI] [PubMed] [Google Scholar]
- 19.Lu CK, Yee MCS, Ravi SB, Pandurangappa R. Forensic age estimation of Chinese Malaysian adults by evaluating occlusal tooth wear using modified Kim's index. Int J Dent. 2017;2017:1–10. doi: 10.1155/2017/4265753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Li C, Ji G. Age estimation from the permanent molar in northeast China by the method of average stage of attrition. Forensic Sci Int. 1995;75:189–96. doi: 10.1016/0379-0738(95)01791-7. [DOI] [PubMed] [Google Scholar]
- 21.Lorentsen M, Solheim T. Age assessment based on translucent dentine. J Forensic Odontostomatol. 1989;7:3–9. [PubMed] [Google Scholar]
- 22.Acharya AB. Forensic dental age estimation by measuring root dentin translucency area using a new digital technique. J Forensic Sci. 2014;59:763–8. doi: 10.1111/1556-4029.12385. [DOI] [PubMed] [Google Scholar]
- 23.Kvaal S, Solheim T. A non-destructive dental method for age estimation. J Forensic Odontostomatol. 1994;12:6–11. [PubMed] [Google Scholar]
- 24.Kvaal SI, Kolltveit KM, Thomsen IO, Solheim T. Age estimation of adults from dental radiographs. Forensic Sci Int. 1995;74:175–85. doi: 10.1016/0379-0738(95)01760-g. [DOI] [PubMed] [Google Scholar]
- 25.Uzuner FD, Kaygisiz E, Darendeliler N. Defining Dental Age for Chronological Age Determination. [Last accessed on 2019 Oct 29]. Available from: http://dx.doi.org/10.5772/intechopen.71699 .
- 26.Cameriere R, Ferrante L, Cingolani M. Variations in pulp/tooth area ratio as an indicator of age: A preliminary study. J Forensic Sci. 2004;49:317–9. [PubMed] [Google Scholar]
- 27.Babshet M, Acharya AB, Naikmasur VG. Age estimation in Indians from pulp/tooth area ratio of mandibular canines. Forensic Sci Int. 2010;197:125.e1–4. doi: 10.1016/j.forsciint.2009.12.065. [DOI] [PubMed] [Google Scholar]
- 28.Jeon HM, Jang SM, Kim KH, Heo JY, Ok SM, Jeong SH, et al. Dental age estimation in adults: A review of the commonly used radiological methods. J Oral Med Pain. 2014;39:119–26. [Google Scholar]
- 29.Nayyar AS, Babu BA, Krishnaveni B, Devi MV, Gayatri HC. Age estimation: Current state and research challenges. J Med Sci. 2016;36:209–16. [Google Scholar]
- 30.Priyadarshini C, Puranik MP, Uma SR. Dental age estimation methods: A review. IJAHS. 2015;1:19–25. [Google Scholar]
- 31.Yang F, Jacobs R, Willems G. Dental age estimation through volume matching of teeth imaged by cone-beam CT. Forensic Sci Int. 2006;159(Suppl 1):S78–83. doi: 10.1016/j.forsciint.2006.02.031. [DOI] [PubMed] [Google Scholar]
- 32.Kazmi S, Mânica S, Revie G, Shepherd S, Hector M. Age estimation using canine pulp volumes in adults: A CBCT image analysis. Int J Legal Med. 2019;133:1967–76. doi: 10.1007/s00414-019-02147-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pinchi V, Pradella F, Buti J, Baldinotti C, Focardi M, Norelli GA. A new age estimation procedure based on the 3D CBCT study of the pulp cavity and hard tissues of the teeth for forensic purposes: A pilot study. J Forensic Leg Med. 2015;36:150–7. doi: 10.1016/j.jflm.2015.09.015. [DOI] [PubMed] [Google Scholar]
- 34.Gulsahi A, Kulah CK, Bakirarar B, Gulen O, Kamburoglu K. Age estimation based on pulp/tooth volume ratio measured on cone-beam CT images. Dentomaxillofac Radiol. 2018;47:1–7. doi: 10.1259/dmfr.20170239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Willems G. Proceedings of the European IOFOS Millienium Meeting Leuven. Leuven, Belgium: Forensic Odontology; 2000. Dental age estimation and computers; pp. 161–75. [Google Scholar]
- 36.Marroquin TY, Karkhanis S, Kvaal SI, Vasudavan S, Kruger E, Tennant M. Age estimation in adults by dental imaging assessment systematic review. Forensic Sci Int. 2017;275:203–11. doi: 10.1016/j.forsciint.2017.03.007. [DOI] [PubMed] [Google Scholar]
- 37.Spalding KL, Buchholz BA, Bergman LE, Druid H, Frisén J. Forensics: Age written in teeth by nuclear tests. Nature. 2005;437:333–4. doi: 10.1038/437333a. [DOI] [PubMed] [Google Scholar]
- 38.Donni S, Haslinda R, Phrabhakaran N, Aspalilah A. Dental age estimation: A review. J Dent Maxillofacial Res. 2018;1:1–3. [Google Scholar]
- 39.Helfman PM, Bada JL. Aspartic acid racemisation in dentine as a measure of ageing. Nature. 1976;262:279–81. doi: 10.1038/262279b0. [DOI] [PubMed] [Google Scholar]
- 40.Ohtani S. Estimation of age from dentin by using the racemization reaction of aspartic acid. Am J Forensic Med Pathol. 1995;16:158–61. doi: 10.1097/00000433-199506000-00017. [DOI] [PubMed] [Google Scholar]
- 41.Ritz S, Stock R, Schütz HW, Kaatsch HJ. Age estimation in biopsy specimens of dentin. Int J Legal Med. 1995;108:135–9. doi: 10.1007/BF01844824. [DOI] [PubMed] [Google Scholar]