
Table 3.
Sarcopenia assessment and clinical outcomes (n = 3,146 patients)
| Author [reference], year, country | n | Sarcopenia definition [reference] | Use of hand grip and/or physical performance | BIA equipment | Percent sarcopenia | Associations of sarcopenia with clinical outcomes | Age, years |
|---|---|---|---|---|---|---|---|
| Perez Camargo 42, 2017, Mexico | 628 |
SMI: Men <8.87 kg/m2 Women <6.42 kg/m2 71 |
No | InBody 720 (Biospace, Tokyo, Japan) Multi‐frequency | 46% | Sarcopenic patients had worse survival (HR 1.4; 95% CI 1.1–1.8; p = .001). Also, more fatigue (p < .0001), pain (p = .008), insomnia (p = .032), and constipation (p = .041). |
Median: 57 Range: 19–89 |
| Otten 27, 2019, Germany | 439 |
SMI: Men <10.75 kg/m2 Women <6.75 kg/m2 2 |
No | Nutriguard M (Data‐Input GmbH) Multi‐frequency | 27.1% |
Observational: Sarcopenia was associated with lower 1‐year overall mortality (HR 1.53; 95% CI 1.034–2.25; p < .05). Sarcopenia was nearly as predictive of 1‐year mortality from advanced disease. |
Mean: 69.6 SD: 6.2 |
| Oflazoglu 43, 2019, Turkey | 461 |
SMI: Men <10.76 kg/m2 Women <6.76 kg/m2 2 |
Yes |
TANITA SC 330 (Tanita Corp., Japan) Single frequency |
16.7% |
Observational: Identified the prevalence of sarcopenia in newly diagnosed patients with cancer. Sarcopenia was more prevalent in patients who were older (p = .03) and who had a higher ECOG score (p = .02). |
Mean: 58.2 SD: (11.1) |
| Harter 28, 2017, Brazil | 60 |
SMI: Men <7.0 kg/m2 Women <6.0 kg/m2 2 |
Yes |
Quantum II (RJL Systems) Multi‐frequency |
18.6% | Observational: No difference in sarcopenic patients with regard to severe postoperative (grade 3, 4, 5) complications (18.2% vs. 12.5%, p = .635). |
18–39 (18%) 40–59 (36%) >60 (45%) |
| Gonzalez 29, 2014, Brazil | 175 |
FFMI (kg/m2) 72 Men <17.4 kg/m2 Women <15.0 kg/m2 |
No |
Quantum 101 (RJL Systems) Single‐frequency |
10.2% |
Observational: Patients with cancer with high mortality risk (HR 6.39; 95% CI 3.54–11.54) can be identified through body composition assessment, even with adjustment for possible confounding variables (HR 4.35; 95% CI 2.11–8.99; p < .0001). Sarcopenia was related with shorter median survival (p < .001). Over 6 months, 50% of sarcopenic patients had died. |
Mean: 56.9 SD: (12.8) |
| Harter 46, 2017, Brazil | 59 |
SMI: Men <7.0 kg/m2 Women <6.0 kg/m2 2 |
Yes |
Quantum II (RJL Systems) Multi‐frequency |
17% | Observational: Physical activity was decreased in all the sarcopenic patients, and nutritional and functional status was impaired. | Not shared |
| Fukuda 47, 2015, Japan | 99 |
SMI: Men <10.75 kg/m2 Women <6.75 kg/m2 2 |
Yes |
InBody 720 (Biospace, Tokyo, Japan) Multi‐frequency |
21.2% |
Observational: Preoperative sarcopenia is a risk factor for severe postoperative complications (4.76; 95% CI 1.03–24.3; p = .046) in patients with cancer undergoing gastrectomy. No difference in overall complications. |
Median: 76 Range: 66–91 |
| Sato 31, 2016, Japan | 293 |
FFMI: Each cut‐point was determined as the gender‐specific lowest 20% of the distribution for each measure based on previously published studies 73, 74 Men <17 kg/m2 Women <14.8 kg/m2 |
Yes |
MC‐180 (Tanita, Tokyo, Japan) Multi‐frequency |
19.7% | Observational: Sarcopenia was not a risk factor for mortality (OR 1.048; p = .99). Hand grip strength (OR 2.254; p = .044) was a risk factor for morbidity in patients with gastric cancer. |
Median: 66 Range: 33–85 |
| Tamura 32, 2019, Japan | 153 |
SMI: Sarcopenia was defined as SMI value of one standard deviation below the gender‐specific mean in the group 75 Men <15.44 kg/m2 Women <13.33 kg/m2 |
No | InBody 3.0 (Biospace, Tokyo, Japan) Multi‐frequency | 15.7% | Observational: Sarcopenic patients had more grade 2 or more general complications (37.5% vs. 16.3%; p = .024), higher laparotomy rate (70.8 % vs. 44.2%; p = .015) and infection complications (29.2% vs. 10%; p = .021) than nonsarcopenic. |
Median sarcopenia: 74 Range: 38–83 Nonsarcopenia: 68 Range: 32–83 |
| Yamamoto 33, 2017, Japan | 90 |
SMI: Men <10.75 kg/m2 Women <6.75 kg/m2 2 |
Yes | Not shared | 24.4% | Interventional: Sarcopenic patients submitted to 3 weeks of exercise and modified diet had increased lean muscle mass (p = .02) and no changes in surgical complications, e.g., pneumonia, leakage, fistula, abscess, bleeding, heart failure, and severe grade > 3 complications. |
Mean: 75 SD: 5 |
| Blake 33, 2017, USA | 125 |
SMI The last quartile of the group |
No |
Maltron Bioscan 920 Multi‐frequency |
25% | Observational: Sarcopenic patients had worse overall survival (HR 1.072; 95% CI 1.01–1.13; p = .009). Sarcopenia was also associated with preoperative anaerobic threshold (R = .277), postoperative morbidity and mortality (p = .005 and p = .031). |
Median: 66 Range: 24–86 |
| Miyata 35, 2017, Japan | 94 |
SMM: <90% lower limit SMM given by the BIA |
No | InBody 720 (Biospace, Tokyo, Japan) Multi‐frequency | 46.8% | Observational: Sarcopenia at baseline is not associated with toxicity (p > .05). Patients who had a larger relative decrease in SMM had higher toxicity (p = .013). |
Mean: 64.7 SD: 8.8 |
| Matsunaga 34, 2019, Japan | 163 | SMM: <90% lower limit | No |
InBody 720 (Biospace, Tokyo, Japan) Multi‐frequency |
50.3% | Observational: Sarcopenia is prognostic for overall survival and is associated with systemic inflammatory response. Sarcopenic patients had higher inflammatory markers; CRP/albumin ratio (p = .046), mGPS (p = .041), and platelet count (p = .016). Sarcopenic patients had worse 2‐year OS (73.1% vs. 85.1%; p = .025) and poor 2‐year RFS (62.8% vs. 76.3%; p = .065). |
Mean: 64.7 SD: 8 |
| Ota 36, 2019, Japan | 31 |
SMI: Men <7 kg/m2 Women <5.7 kg/m2 12 |
No |
InBody 720 (Biospace, Tokyo, Japan) Multi‐frequency |
51.6% |
Observational: Sarcopenia is an independent predictor of poor pathological response (p = .038) but not therapeutic response (p = .103). In multivariate analysis, sarcopenia was an independent risk factor for poor therapeutic response (OR 8.02; 95% CI 1.12–165.41; p = .037). Toxicities were not different between both groups. |
Median: 66 Range: 41–75 |
| Ida 37, 2015, Japan | 138 | SMM: <90% lower limit | No | InBody 720 (Biospace, Tokyo, Japan) Multi‐frequency | 44.2% | Observational: Sarcopenic patients had more pulmonary complications after esophagectomy compared with nonsarcopenic patients (15.2% vs. 6.5%; p < .01). |
Mean sarcopenic: 67.8 SD: 1 Nonsarcopenic: 63.1 SD: 0.9 |
| Makiura 30, 2016, Japan | 104 |
SMI: Men <7 kg/m2 Women <5.7 kg/m2 12 |
Yes |
DF‐860 (Yamato, Hyogo, Japan) Multi‐frequency |
27.9% | Observational: Sarcopenia is associated with more pulmonary complications (37.9% vs. 17.3%; p = .04). Also, greater blood loss (p < .001) and longer hospitalizations (p < .001). No differences with other complications or perioperative functional changes. |
Median sarcopenic: 69 Range: 66–76 Nonsarcopenic: 64 61–71 |
| Ishikawa 38, 2016, Japan | 33 |
SMI: Men <7.0 kg/m2 Women <5.7 kg/m2 2 |
No | InBody 720 (Biospace Tokyo, Japan)Multi‐frequency | 60.6% |
Intervention: Elental nutrition can counteract sarcopenia development during chemoradiotherapy for esophageal cancer (p = .007). It did not affect chemotoxicity. |
Median: 68 Range: 50–76 |
| Collins 39, 2017, U.K. | 62 |
SMI: Men <7.26 kg/m2 Women <5.45 kg/m2 |
No |
Tanita BC‐418 Single frequency |
19.4% | Observational: No difference in sarcopenic patients regarding completion of chemotherapy or adverse events. BIA overestimates muscle mass compared with DXA scan. |
Mean: 68.2 SD: 9.6 |
| Miyake 50, 2017, Japan | 35 |
SMI: Men <7.0 kg/m2 Women <6.0 kg/m2 68 |
No | InBody S20 (Biospace, Tokyo, Japan) Multi‐frequency | 20% |
Observational: BIA has similar findings to CT scans for assessing sarcopenia in metastatic urothelial carcinoma. Sarcopenia was present in five patients using CT and in seven using BIA; three patients were sarcopenic according to both methods. |
Median: 73 Range: 64–77 |
| Dos Reis 45, 2018, Brazil | 40 |
SMI: Men <10.75 kg/m2 Women <6.75 kg/m2 |
Yes | Not shared | 62.5% | Observational: Sarcopenic patients have no differences in health‐related quality of life. | Mean: 62 |
| Hopanci Bicakli 40, 2019, Turkey | 153 |
SMI: Men <10.75 kg/m2 Women <6.75 kg/m2 |
Yes |
Tanita MC 718 Multi‐frequency |
80% (30% sarcopenic obese) | Observational: BIA assessed sarcopenia correlates with calf circumference (r = .598, p < .001). |
Mean: 70.5 SD: 5.6 |
| Gibson 49, 2017, U.S. | 43 | FFMI: <1 SD from the young adult norm | No |
Bodystat 1500 Dual‐frequency |
18.6% | Observational: BIA has a high correlation with CT scan for screening sarcopenia (r = .711, p < .001); however, the incidence was higher with BIA. |
Mean: 69.5 SD: 12 |
| Barbosa 44, 2018, Brazil | 73 |
SMI: Men <10.75 kg/m2 Women <6.75 kg/m2 |
No | Not shared | 46% | Observational: Sarcopenic patients have no differences in health‐related quality of life. |
Mean: 63.9 SD: 11.3 |
| Kamyia 53, 2018, Japan | 56 |
SMI: Men <7.0 kg/m2 Women <5.7 kg/m2 2 |
Yes |
InBody 720 (Biospace, Tokyo, Japan) Multi‐frequency |
36% | Observational: Sarcopenic patients had significantly lower levels of serum dehydroepiandrosterone‐sulfate and a higher CCI score than patients who were not sarcopenic. More sarcopenic patients failed to complete the treatment planned as compared with nonsarcopenic patients (p = .001). |
Median: 77 Range: 60–93 |
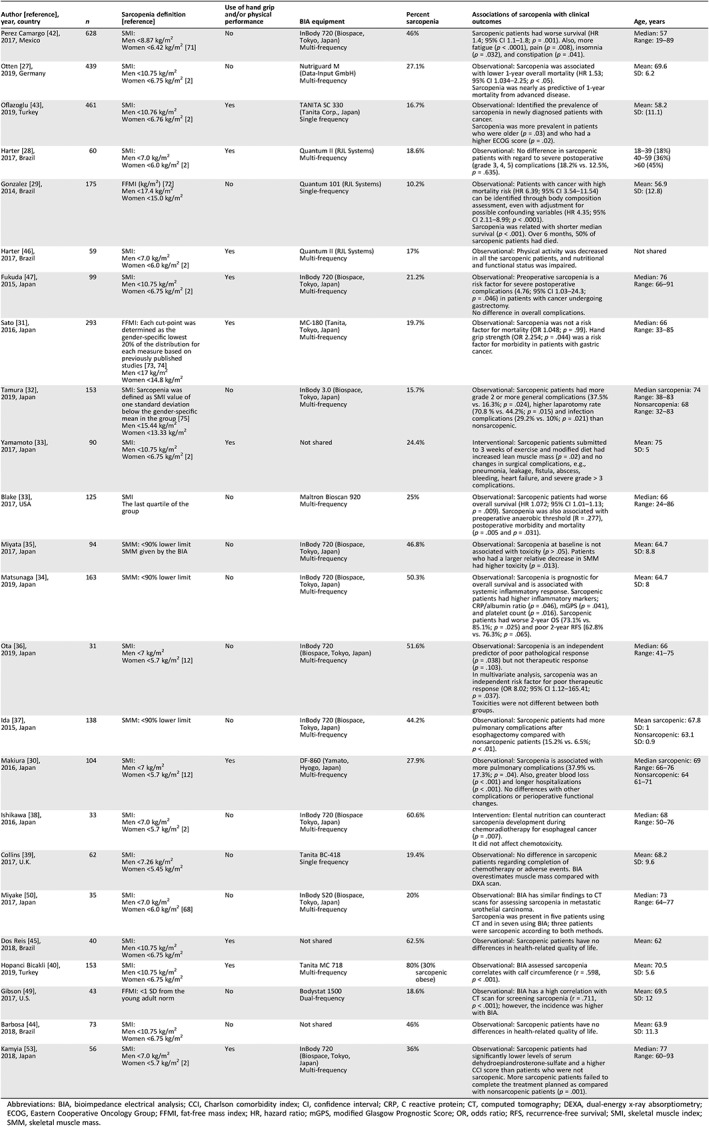
Abbreviations: BIA, bioimpedance electrical analysis; CCI, Charlson comorbidity index; CI, confidence interval; CRP, C reactive protein; CT, computed tomography; DEXA, dual‐energy x‐ray absorptiometry; ECOG, Eastern Cooperative Oncology Group; FFMI, fat‐free mass index; HR, hazard ratio; mGPS, modified Glasgow Prognostic Score; OR, odds ratio; RFS, recurrence‐free survival; SMI, skeletal muscle index; SMM, skeletal muscle mass.