

Supplemental Digital Content is available in the text.
Abstract
Background:
Biomaterials derived from human adipose extracellular matrix have shown promise in vitro and in animal studies as an off-the-shelf adipogenic matrix for sustained volume replacement. Herein, we report the results of a randomized prospective study conducted with allograft adipose matrix (AAM) grafted into the pannus of presurgical abdominoplasty patients 3 or 6 months before scheduled surgery. This is the first report of a longitudinal histologic analysis of AAM in clinical use.
Methods:
Ten healthy patients undergoing elective abdominoplasty were recruited to receive AAM before surgery. Enrolled subjects were randomized into either a 3-month follow-up cohort or a 6-month follow-up cohort. Subjects were monitored for adverse events associated with AAM grafting in addition to undergoing serial biopsy. Following surgical excision of the pannus, representative samples from the AAM surgical sites were stained and evaluated with hematoxylin and eosin for tissue morphology, Masson’s trichrome for collagen, and perilipin for adipocytes.
Results:
All subjects tolerated AAM with no severe adverse events reported. At 3 months following implantation, AAM remained visible within the confines of the subjects’ native surrounding adipose tissue with sparse adipocytes apparent within the matrix. By 6 months, AAM had remodeled and was primarily composed of perilipin-positive adipocytes. Histologic analysis confirmed tissue remodeling (hematoxylin and eosin), adipogenesis (perilipin), and angiogenesis (Masson’s trichrome) occurred with the presence of AAM.
Conclusions:
AAM is a safe, allogeneic, off-the-shelf regenerative matrix that is adipogenic and noninflammatory and promotes angiogenesis.
INTRODUCTION
Autologous fat grafting is an established technique for addressing volume and contour abnormalities in plastic surgery, with substantial utility in both aesthetic and reconstructive procedures.1–7 However, fat grafting may not always be possible when lack of donor site precludes adipose harvest or when the volume of material required does not balance associated costs of an additional outpatient surgical procedure. Further, complications of fat grafting, including poor adipocyte survival under hypoxia, cell lysis, oil accumulation, and formation of oil cysts and calcifications, can limit efficacy. There is a significant clinical interest in developing an alternative, off-the-shelf product that eliminates the need for tissue harvesting and graft processing, overcomes fat grafting associated complications, and can be delivered outside of an operating room setting.
Extracellular matrix (ECM) scaffolds are commercially available for a wide variety of clinical applications and are useful for tissue regeneration and wound healing. Adipose tissue is an abundant source of cell-adhesive matrix proteins such as collagens, fibronectin, and laminin and when extracted, yield a biomaterial with favorable tissue regenerative properties. Preclinical studies by Kokai et al and Giatsidis et al have evaluated the safety and efficacy of allograft adipose matrix (AAM) processed by MTF Biologics (Edison, NJ), demonstrating the ability of the material to form new adipose tissue in immunocompromised and immunocompetent mouse models, respectively.8,9 Clinically, AAM safety has been assessed following implantation into the dorsum of the nondominant wrist in healthy human subjects and histologic analysis supported previous results in animal studies for matrix reorganization and adipose generation.8
Herein, we report the results of a randomized prospective clinical study conducted at the University of Pittsburgh where AAM (Renuva; MTF Biologics) was grafted into the pannus of presurgical abdominoplasty patients with longitudinal biopsies obtained to assess the cellular response. Renuva is regulated by the Food and Drug Administration and classified as a human cellular and tissue-based product. The primary objective of the study was to evaluate local tissue reaction, tissue architecture, and AAM remodeling after injecting into the subcutaneous tissues of the abdominal wall in subjects undergoing elective abdominoplasty surgery. The secondary objective was to assess the rate of complications of the AAM in human subjects undergoing elective abdominoplasty. This is the first such clinical study showing that AAM promotes soft tissue regeneration in an allograft setting and is a promising scaffold for regenerating adipose tissue.
METHODS
Subject Recruitment and Enrollment
An investigator-initiated, randomized, 2-cohort prospective Institutional Review Board-approved study [registration number/identifier of the trial (NCT02845180)] was conducted through the Center for Innovation in Restorative Medicine at the University of Pittsburgh with funding as well as AAM samples provided by MTF Biologics. Ten patients referred to the Department of Plastic Surgery for abdominoplasty were recruited for the study based on inclusion/exclusion criteria (Table 1). Subjects were randomized into 1 of 2 study cohorts. One study cohort consisted of 5 subjects who received injections of AAM to be followed clinically for 3-month duration, and the second cohort consisted of 5 subjects who received injections of AAM to be followed clinically for 6-month duration (Fig. 1). At 1 and 2 months post injection, excisional biopsies were obtained from unique injection sites. At the point of completion of each cohort (3 or 6 months post injection), the injected tissue was surgically removed as part of the panniculectomy procedure. Samples of the injected AAM and surrounding tissue were obtained and processed for histologic evaluation (described in further detail below). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Table 1.
Inclusion and Exclusion Criteria for the Study
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age >18 y | Subcutaneous tissue thickness <2 cm |
| BMI 23–35 | Prior liposuction |
| Panniculectomy candidate | Current immunosuppressive therapy |
| Subcutaneous tissue thickness >2 cm | Chronic anticoagulation |
| Pregnant or lactating | |
| Abnormal preoperative laboratories |
BMI, body mass index.
Before AAM injection, baseline subcutaneous tissue thickness was assessed with ultrasound. AAM was injected into the pannus, with 20 mL of rehydrated material injected into each of 6 areas within the confines of the planned surgical resection, for a total of 120-mL AAM per subject. In exchange for participation, subjects received abdominoplasty surgery at no cost to them in addition to being paid for regularly scheduled clinical visits.
Adipose Allograft Implantation Technique
On the day of surgery, subcutaneous adipose thickness was confirmed to be >2 cm in depth with ultrasound. A grid of six 4 cm × 6 cm areas were marked across the pannus within the confines of an abdominoplasty resection (Fig. 2), and topical 1% lidocaine jelly was then applied. After the injection of local anesthetic, 1 mL of 1% lidocaine with 1:100,000 epinephrine at each site, below the umbilicus and above the pubic symphysis, small stab incisions were made and dilute tumescent anesthesia was instilled to anesthetize the anterior abdominal wall. AAM (Renuva, MTF Biologics, Edison NJ) units reconstituted with normal saline solution according to manufacturer guidelines were injected in the subcutaneous tissue of the pannus, subdermally, in 4 cm× 6 cm areas, with a total of 20 mL injected at each of the 6 sites using a Coleman 19-G fat grafting cannula. A simple absorbable 4-0 fast gut suture was used to close the incisions. Each injection area was permanently marked with indelible ink and a 30-G hypodermic needle affixed to a 1-mL syringe. Sterile gauze dressing was applied over the incision sites and changed as needed until exudate from the wounds ceased.
Fig. 2.
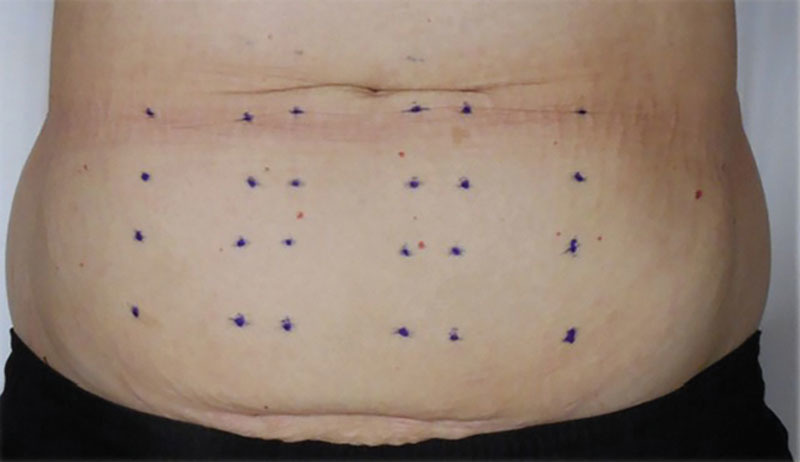
Abdominal wall grid utilized for injection.
Fig. 1.
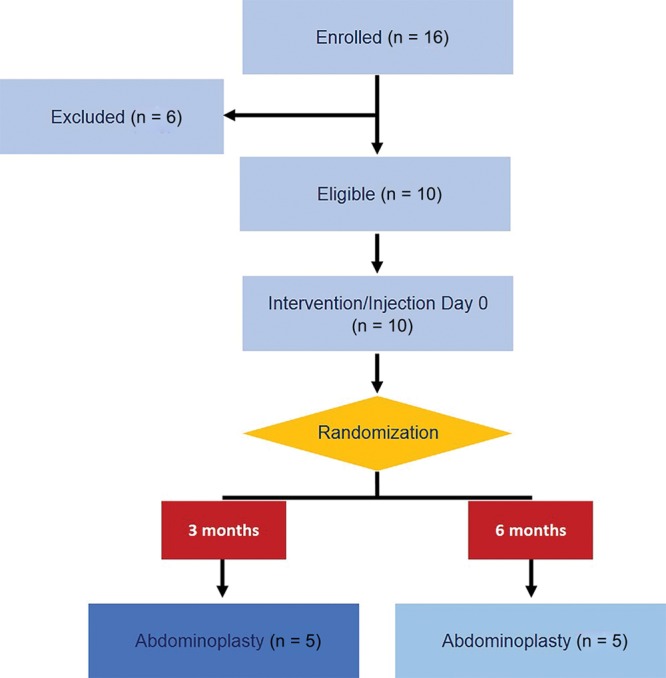
Clinical study enrollment and randomization design showing 16 enrolled subjects; of these, 10 met study inclusion criteria. Randomization into 1 of 2 cohorts occurred at the time of intervention yielding two cohorts, each with 5 subjects. Cohort 1 underwent abdominoplasty 3 months after intervention and cohort 2 at 6 months post intervention.
Clinical Assessment
At each study visit, a physical assessment of the injection site was performed where characteristics (ie, texture, position, etc.) of the material were noted based on palpation of the abdominal tissue. The Common Terminology Criteria for Adverse Events grading system was used to evaluate adverse events.
Histologic Analysis
Following abdominoplasty surgical excision, tissue samples were fixed en bloc, embedded in paraffin, and visualized with hematoxylin and eosin (H&E), Masson’s trichrome for collagen and overall tissue architecture, and perilipin immunohistochemistry for lipid accumulation. H&E slides were reviewed by AK (Division of Molecular & Genomic Pathology). Composite images of tissue sections visualized with Masson’s trichrome stain (for basic tissue architecture and angiogenesis) and perilipin antibodies (for adipogenesis) were obtained with a Keyence BZ-X microscope.
Pathology Review
Of the 10 enrolled study subjects, 9 consented to longitudinal biopsies. At each time point of 1, 2, 3, and 6 months, biopsies from the areas of AAM injection from each study time point were stained for H&E by the University of Pittsburgh Biospecimen Core. Histopathologic analyses were performed for 3–5 sites on each subject. All slides were reviewed by a licensed pathologist (AK) with respect to adipocytes (morphology and coverage), presence of AAM matrix or matrix-like substance, prevalence of spindled/interstitial/inflammatory cells in a fibrous or collagen-deposited stroma and/or collagenous banding, tissue vascularity, and presence of capsule. Approximate quantifications of percentage presence for each property were made for each parameter with the exception of encapsulation.
Statistical Analyses
JMP Pro 14 was used for all statistical analyses. Bivariate fits were modeled for percent adipocyte coverage against time in months and for percent adipocyte coverage against percent residual AAM as interpreted from the histopathologic read. For statistical interpretations of the regressions performed, P-values less than 0.05 were considered significant. The study’s primary endpoint of AAM efficiency was tested at 3 and 6 months by evaluated mature adipocytes; the study’s secondary endpoint of safety was not tested statistically.
RESULTS
Ten patients (7 women, 3 men, average age 40.3 ± 9.3 years) were enrolled in the IRB-approved study, and eligibility was determined. Ultrasound determined an average abdominal fat tissue thickness of 2.8 ± 0.4 cm at screening. The average body mass index of enrolled subjects was 29.5 ± 2.5 at screening. Subject weight remained stable over the study time course.
Overall, subjects tolerated AAM injections with minimal discomfort. There was 1 minor complication out of 60 injected sites (surgical site infection after open biopsy at 1 month treated with oral antibiotics) across all 10 subjects in the study. Several subjects experienced swelling and redness related to tattooing that was transient and resolved within 24 hours. Several subjects also experienced expected adverse events such as pain and bruising at the site of AAM injection. The material was initially palpable and softened over time such that it was difficult to discriminate with direct palpation at 3 months.
Upon biopsy at 1 and 3 months following implantation, AAM remained macroscopically distinct from native adipose tissue with distinct boundaries from the surrounding adipose tissue (Fig. 3A); however, by 6 months, AAM appeared visually similar to native adipose tissue (Fig. 3B).
Fig. 3.
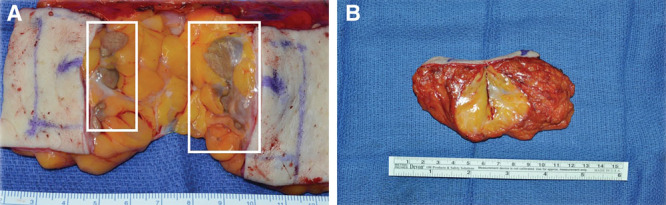
Gross appearance of the AAM at 3 (A) and 6 (B) months.
Cellular remodeling was observed across all histologic analyses of the material over time. Representative histopathologic results from 3 study subjects are presented in Table 2, and the histopathologic results from all subjects are presented in Supplemental Digital Content 1 (see figure, Supplemental Digital Content 1, which displays the descriptive and semiquantitative histopathologic results from all analyzed subjects, http://links.lww.com/PRSGO/B281).
Table 2.
Representative Histopathologic Results from 3 Subjects
| Patient ID | Month | Adipocyte Characteristics | Matrix or Matrix-like Substance | Fibrous or Collagenous Stroma | Capsule Description | |||
|---|---|---|---|---|---|---|---|---|
| Adipocyte Coverage (%) | Description | Residual AAM (%) | Description | Fibrous Coverage (%) | Description | |||
| 05 | 1 | 10 | Few, sparse adipocytes | 60 | Fragmented residual matrix | 25 | Compact stroma | No distinct capsule |
| 05 | 2 | 40 | Increased and variably sized adipocytes with increased capillaries | 30 | Fragmented residual matrix | 30 | Compact stroma | No distinct capsule |
| 05 | 3 | 30 | Increased and variably sized adipocyte distribution with increased capillaries | 30 | Most residual matrix evenly digested | 40 | Compact or globular stroma with hemosiderophages | No distinct capsule |
| 06 | 1 | 30 | Increased and variably sized adipocyte distribution with increased capillaries | 10 | Most residual matrix evenly digested and surrounded by inflammatory cells | 55 | Compact or globular stroma with foci of cellular fibroblastic reaction | Thick capsule or septa |
| 06 | 6 | 80 | Nearly normal adipose tissue | 0 | Absent | 10 | As septa and small globule with collagen and macrophages | Thickened fibrous septa |
| 12 | 1 | 30 | Some adipocyte distribution with increased capillaries throughout | 30 | Beginning fragmentation | 40 | Globular with some septa-like thickening | Thickened fibrous septa |
| 12 | 2 | 20 | Some adipocyte distribution with increased capillaries throughout | 50 | Continuing fragmentation | 30 | Globular with some septa-like thickening; mild presence of lymphocytic aggregates | Not applicable |
| 12 | 6 | 30 | Increased adipocyte distribution with increased capillaries throughout relative to 2-mo biopsy | 50 | Fragmented and cystic | 30 | Globular with some septa-like thickening; residual presence of lymphocytic aggregates | Thickened capsule |
Based on the semiquantitative histopathologic assessments, adipocyte coverage generally increased over the 3- and 6-month durations with capillaries appearing as early as the 1-month biopsy and then shrinking in size over the remainder of the study; concomitantly both residual AAM and the stroma deposition decreased (see figure, Supplemental Digital Content 2, which displays the pooling of semiquantitative histopathologic assessments across all analyzed subjects presenting increasing adipocyte coverage, whereas both residual AAM and the stroma deposition decreased; http://links.lww.com/PRSGO/B282). Bivariate modeling of percent adipocyte coverage against time (months) was shown to be significantly correlated (P < 0.01), where increasing adipocyte coverage was observed (Fig. 4). In addition, bivariate modeling of the percent adipocyte coverage against present residual AAM was also shown to be significantly correlated (P < 0.001), presenting inverse proportionality of adipocyte coverage and residual AAM (Fig. 5).
Fig. 4.
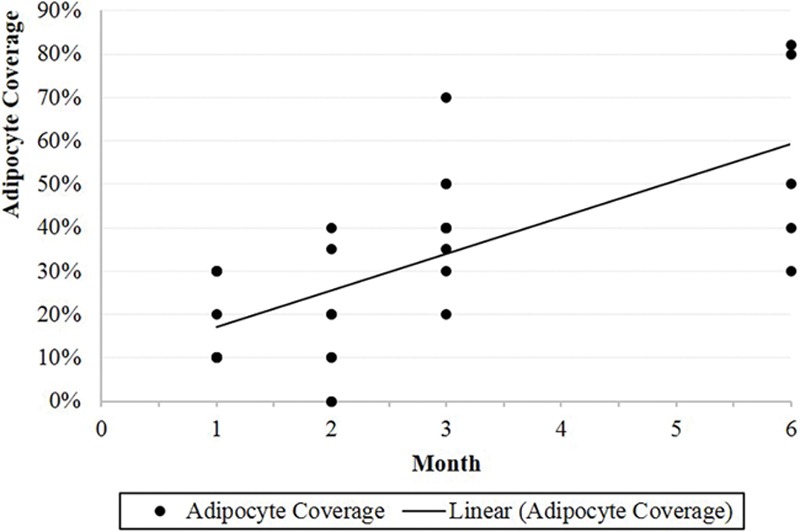
Bivariate modeling of percent adipocyte coverage against time (months).
Fig. 5.
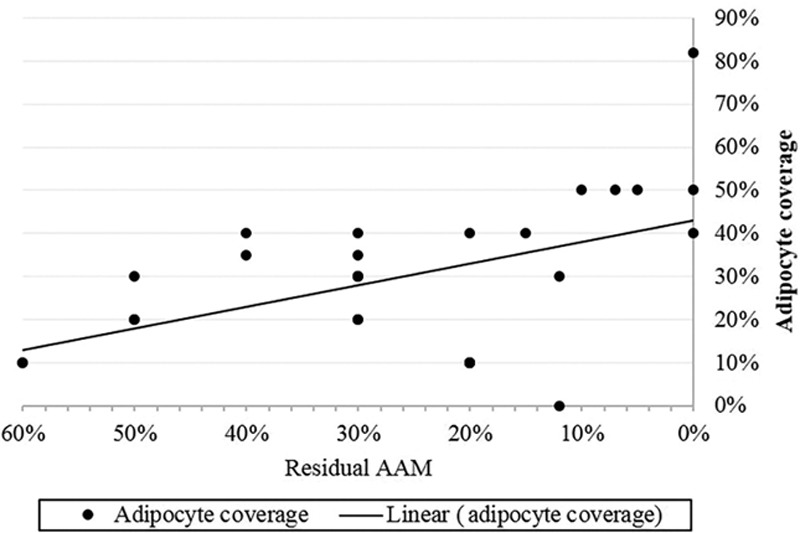
Bivariate modeling of the percent adipocyte coverage against present residual AAM.
Masson’s trichrome revealed the initial presence and then remodeling of collagen with increased vascularization (Figs. 6 and 7). At 1-month biopsy, analysis of the presence of perilipin revealed new fat cells within AAM, which increased at 2 months and either 3 (Fig. 8) or 6 months (Fig. 9). These tissue remodeling phenomena were corroborated by H&E staining, where representative histology from injection site neighboring adipose tissue is presented along with images from the 1-, 2-, 3-, and 6-month time points (Fig. 10).
Fig. 6.
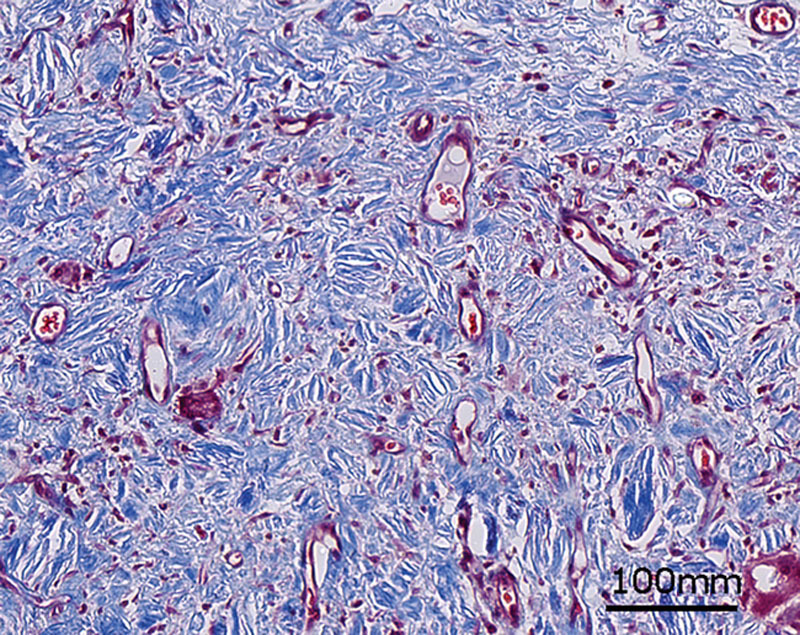
Representative biopsy of AAM obtained at 1 month stained with Masson’s trichrome.
Fig. 7.
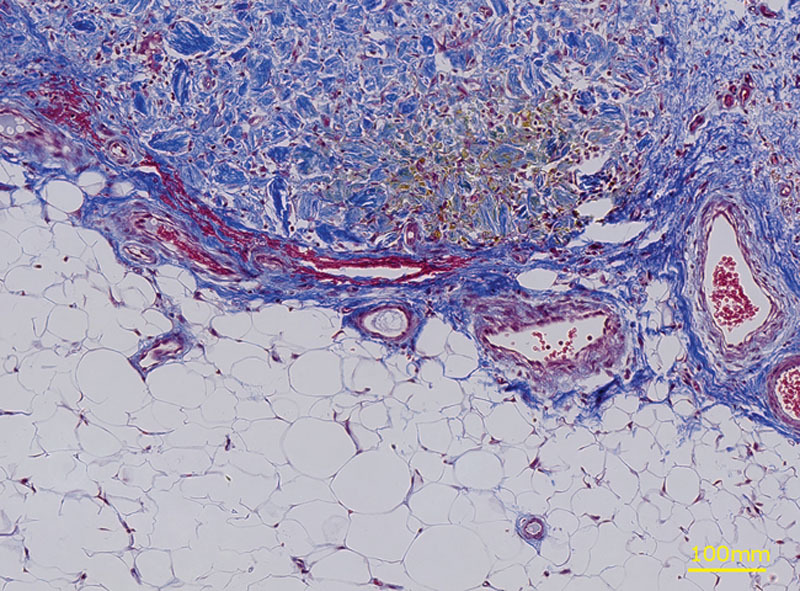
Representative biopsy of AAM obtained at 3 months stained with Masson’s trichrome.
Fig. 8.
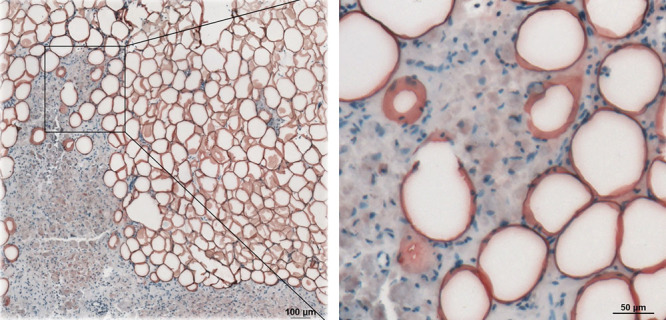
Representative biopsy of AAM obtained at 2 months observed with immunohistochemistry for perilipin. Low magnification, 10X (left) with area of interest at high magnification, 40X (right).
Fig. 9.
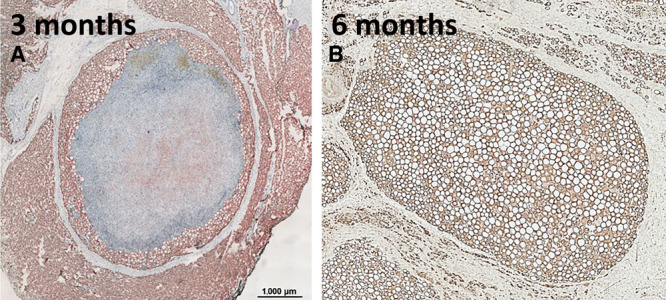
Representative biopsy of AAM obtained at 3 months (A) or 6 months (B) observed with immunohistochemistry for perilipin.
Fig. 10.
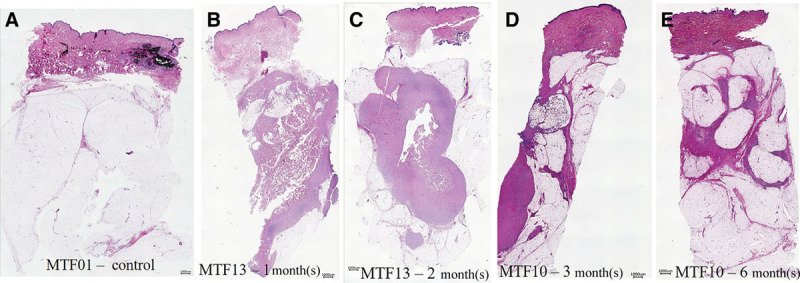
Representative H&E staining across all time points. A, Injection site neighboring adipose tissue. B, One-month biopsy. C, Two-month biopsy. D, Tissue segment removed post panniculectomy at 3 months. E, Tissue segment removed post panniculectomy at 3 months.
DISCUSSION
Previous in vitro and in vivo studies have reported that AAM is a regenerative matrix that promotes cellular infiltration, attachment, migration, and replacement with mature adipose cells. In our previous study, we showed that allogeneic adipose stem cells cultured on an adipose matrix produced by a similar decellularization process migrated throughout the matrix and differentiated to adipocytes without the addition of exogenous stimuli such as isobutylmethylxanthine, dexamethasone, or insulin. We also showed that implantation of AAM in the dorsum of immunocompromised mice resulted in de novo adipose tissue formation with sustained volume retention out to 24 weeks. Finally, in a pilot clinical study, up to 5 mL of AAM was injected into the wrist of 15 patients with satisfactory results in regard to material pliability and volume replacement. In this study, we increased the volume of AAM injected into abdominal adipose tissue (120 mL per patient divided evenly into 6 recipient sites) and obtained serial biopsies to longitudinally observe cellular interactions with the matrix, demonstrating material safety and cell compatibility. No severe adverse events were observed, and increasing amounts of infiltrating adipocytes were identified over time with concurrent turnover of the injected adipose matrix, indicating the regenerative nature of the allogeneic matrix.
Previous biochemical and immunohistological analysis of AAM by our group and others have described an abundant presence of matrix proteins supporting cell adhesion including collagen type I, III, IV, and VI, and laminin.10,11 Although the processes used to remove cellular components of adipose tissue vary across published studies, a proteomic analysis of AAM produced with 3 unique classifications of cell extraction by Thomas-Porch et al showed that the treatment of adipose tissue with detergents such as sodium dodecyl sulfate was superior to other methods for generating ECM scaffolds with both reduced genomic DNA and intact cell matrix proteins.12 In this study, the authors showed that matrices derived from detergent-based processing of adipose yielded cell scaffolds of intact fibrous networks primarily composed of collagen, including an abundance of type VI collagen and lower quantities of laminin and fibronectin. During maturation, adipose progenitor cells alter the extracellular microenvironment by reducing type I and III collagen production by 80%–90% and significantly increasing the secretion of type VI collagen13 to maintain their phenotype. Previous work in medical device coatings has shown that type VI collagen significantly improves adipocyte attachment and promoted adipogenesis compared to control coatings.14 Other ECM proteins shown by Thomas-Porch et al, as retained in acellular matrices, include laminin and collagen XV, which are also inherently adipogenic.15,16 Therefore, we hypothesize that ECM proteins contained in acellular adipose matrices support cell adhesion and migration of cells from the recipient tissue bed and permit adipogenesis through integrin signaling and positive regulation of adipogenic genes, which is corroborated by the decreasing presence of AAM proportional to the increase coverage of adipocytes here.
Although the type of ECM protein has a significant impact on cytoskeletal network rearrangement and can induce signal transduction that influences cell differentiation, our group and others have shown that various growth factors are bound to ECM components including fibroblast growth factor-1 and fibroblast growth factor-2, endothelial growth factor, bone morphogenetic growth factor-9, and vascular endothelial growth factor-A.17 Decellularized adipose tissue is rich in sulfated glycosaminoglycans, the principal element of ECM that sequesters endogenous growth factors.18,19,20 Therefore, in addition to containing adipogenic permissive adherence proteins, we further hypothesize that AAM contains sequestered growth factors and/or cytokines and through cell binding, can modulate the cellular response to such factors.
The current study has several limitations to consider. First, subject recruitment was limited to 10 subjects due to significant associated resources required for study completion and the study length was short, only 6 months. The limited study size may increase the statistical margin of error. Second, observation of material retention, cellular infiltration, and morphology in AAM was limited to histologic analysis, which is semiquantitative at best and restricts visualization of the material to thin 6-µm sections. Although care was taken to obtain cross-sections of biopsy midpoints, and longitudinal assessment of sample biopsies suggested increased accumulation of adipocytes over time, it remains impossible to definitely differentiate between de novo adipogenesis from tissue already present in the recipient bed.
Another study limitation is the use of the panniculectomy model for assessing inherent adipogenic qualities of AAM. Although an abundance of studies with ECM-derived scaffolds have suggested that donor sources of ECM are most important for determining cell behavior, the recipient tissue bed also impacts the ultimate outcome of grafted material due to the type of infiltrating cells from adjacent tissue as well as the density of local vasculature. In this study, AAM was implanted within a thick adipose tissue pannus and therefore the frequency of migrating adipose progenitor cells may have been higher than other potential tissue void applications. Further, study subjects were limited to patients already scheduled for body contouring procedures after substantial weight loss, indicating an inherent propensity to accumulate excess adipose tissue in this specific subject population. Therefore, it is difficult to predict how AAM will perform in very lean patients or in recipient beds lacking adipose tissue such as in craniofacial applications.
In summary, we have demonstrated that AAM injected into abdominal adipose tissue in clinically relevant volumes (20 mL per injection site, 6 sites per subject) can be achieved without significant adverse events and provides a cell scaffold that is reorganized over time. Immediately post injection, the material felt firmer than surrounding adipose tissue but became more pliable and similar to native adipose tissue within the 6-month time span of this study. Further, longitudinal analysis of material biopsies revealed material volume retention out to 6 months with increasing density of perilipin-expressing adipocytes at each sequential study time point. Although further analysis in more patients and additional applications are warranted, our results suggest that AAM retains critical ECM components that permit cell attachment and migration as well as adipogenic instructive cues.
CONCLUSIONs
To conclude, AAM is an easy to use, allogeneic off-the-shelf regenerative matrix that is safe, adipogenic, and noninflammatory and remodels into endogenous adipose tissue. With AAM, adipose replacement was achieved without adipose tissue harvesting and processing, saving time and cost.
Supplementary Material
Footnotes
Published online 17 January 2020.
Presented at the International Federation for Adipose Therapeutics and Science Meeting, 2017, 2018; Plastic Surgery The Meeting, Chicago, IL, October 2018; and 61st Annual Meeting of the Ohio Valley Society of Plastic Surgeons, Cleveland, OH, June 2018.
Supported by a sponsored research agreement between MTF and the University of Pittsburgh.
Disclosure: Dr. D’Amico is a paid consultant for the Musculoskeletal Transplant Foundation. The views expressed in this abstract and manuscript are those of the authors and do not necessarily reflect the official policy or position of the University of Pittsburgh or the University of Pittsburgh Medical Center. The University of Pittsburgh received grant funding in addition to allograft adipose matrix from MTF Biologics used in this project. None of the other authors has any financial disclosures.
Related Digital Media are available in the full-text version of the article on www.PRSGlobalOpen.com.
REFERENCES
- 1.Choi M, Small K, Levovitz C, et al. The volumetric analysis of fat graft survival in breast reconstruction. Plast Reconstr Surg. 2013;131:185–191. [DOI] [PubMed] [Google Scholar]
- 2.Clauser LC, Tieghi R, Galiè M, et al. Structural fat grafting: facial volumetric restoration in complex reconstructive surgery. J Craniofac Surg. 2011;22:1695–1701. [DOI] [PubMed] [Google Scholar]
- 3.Coleman SR. Structural fat grafts: the ideal filler? Clin Plast Surg. 2001;28:111–119. [PubMed] [Google Scholar]
- 4.Coleman SR. Structural fat grafting: more than a permanent filler. Plast Reconstr Surg. 2006;118:108S–120S. [DOI] [PubMed] [Google Scholar]
- 5.Gir P, Brown SA, Oni G, et al. Fat grafting: evidence-based review on autologous fat harvesting, processing, reinjection, and storage. Plast Reconstr Surg. 2012;130:249–258. [DOI] [PubMed] [Google Scholar]
- 6.Kaufman MR, Miller TA, Huang C, et al. Autologous fat transfer for facial recontouring: is there science behind the art? Plast Reconstr Surg. 2007;119:2287–2296. [DOI] [PubMed] [Google Scholar]
- 7.Wetterau M, Szpalski C, Hazen A, et al. Autologous fat grafting and facial reconstruction. J Craniofac Surg. 2012;23:315–318. [DOI] [PubMed] [Google Scholar]
- 8.Kokai LE, Schilling BK, Chnari E, et al. Injectable allograft adipose matrix supports adipogenic tissue remodeling in the nude mouse and human. Plast Reconstr Surg. 2019;143:299e–309e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Giatsidis G, Succar J, Haddad A, et al. Preclinical optimization of a shelf-ready, injectable, human-derived, decellularized allograft adipose matrix. Tissue Eng Part A. 2019;25:271–287. [DOI] [PubMed] [Google Scholar]
- 10.Flynn LE. The use of decellularized adipose tissue to provide an inductive microenvironment for the adipogenic differentiation of human adipose-derived stem cells. Biomaterials. 2010;31:4715–4724. [DOI] [PubMed] [Google Scholar]
- 11.Choi JS, Kim BS, Kim JY, et al. Decellularized extracellular matrix derived from human adipose tissue as a potential scaffold for allograft tissue engineering. J Biomed Mater Res A. 2011;97:292–299. [DOI] [PubMed] [Google Scholar]
- 12.Thomas-Porch C, Li J, Zanata F, et al. Comparative proteomic analyses of human adipose extracellular matrices decellularized using alternative procedures. J Biomed Mater Res A. 2018;106:2481–2493. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gregoire FM, Smas CM, Sul HS. Understanding adipocyte differentiation. Physiol Rev. 1998;78:783–809. [DOI] [PubMed] [Google Scholar]
- 14.Beringer LT, et al. Promoting adipogenesis using a collagen VI–heparin sulfate coating: applications in tissue engineering for wound healing. Industrial & Engineering Chemistry Research. 2016;55:12687–12692. [Google Scholar]
- 15.Liu G, Li M, Xu Y, et al. ColXV promotes adipocyte differentiation via inhibiting DNA methylation and camp/PKA pathway in mice. Oncotarget. 2017;8:60135–60148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lee J, Abdeen AA, Tang X, et al. Matrix directed adipogenesis and neurogenesis of mesenchymal stem cells derived from adipose tissue and bone marrow. Acta Biomater. 2016;42:46–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nimni ME, Han BO. Collagen and collagen-glycosaminoglycan matrices as carriers for growth factors. Proceedings of the Indian Academy of Sciences-Chemical Sciences. 1999;111:283–289. [Google Scholar]
- 18.Mhanna R, et al. Sulfated alginate as a mimic of sulfated glycosaminoglycans: binding of growth factors and effect on stem cell behavior. Advanced Biosystems. 2017;1:1700043. [DOI] [PubMed] [Google Scholar]
- 19.Sun C, Marcello M, Li Y, et al. Selectivity in glycosaminoglycan binding dictates the distribution and diffusion of fibroblast growth factors in the pericellular matrix. Open biology, 2016;6: 150277 doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Song M, Liu Y, Hui L. Preparation and characterization of acellular adipose tissue matrix using a combination of physical and chemical treatments. Mol Med Rep. 2018;17:138–146. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.