
Figure 2.
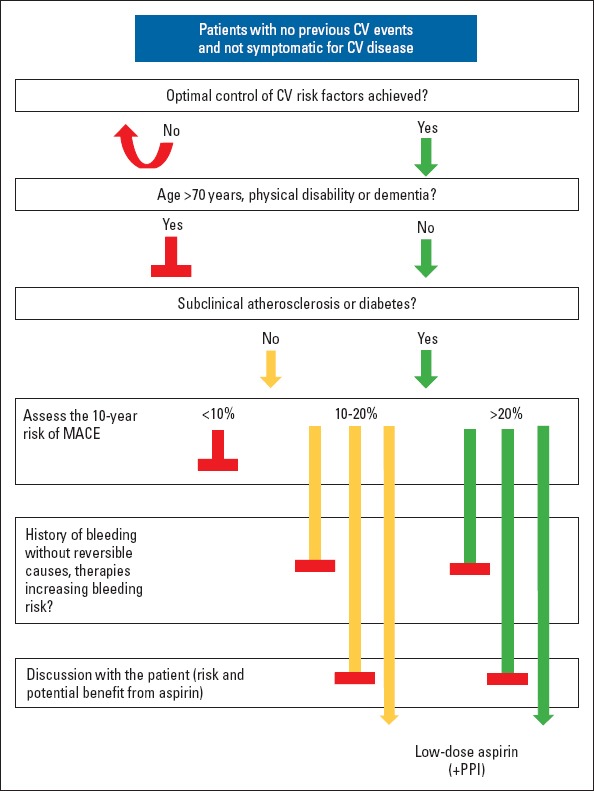
Proposed stepwise approach to prescribing aspirin for primary cardiovascular prevention
Patients undergoing primary cardiovascular (CV) prevention should achieve optimal control of CV risk factors. When patients are aged <70 years and are free from physical disability or dementia, they should undergo a CV risk stratification, especially when there is evidence of subclinical atherosclerosis or diabetes. When the 10-year risk of major adverse cardiovascular events (MACE) is >20%, it is recommended to start therapy with aspirin after discussing the risks and benefits of aspirin intake with the patients, particularly if there are no conditions of increased bleeding risk. Aspirin should be prescribed along with a proton-pump inhibitor (PPI) to reduce the risk of gastrointestinal bleeding. The commencement of aspirin therapy should be carefully evaluated when the 10-year risk is between 10% and 20%, and aspirin should not be prescribed when the 10-year risk is <10% Modified from De Caterina et al., 2019 (18)