
Figure 5. Hypoxia-Induced Increase in APD Mediated by SUMO Modulation of ILATE.
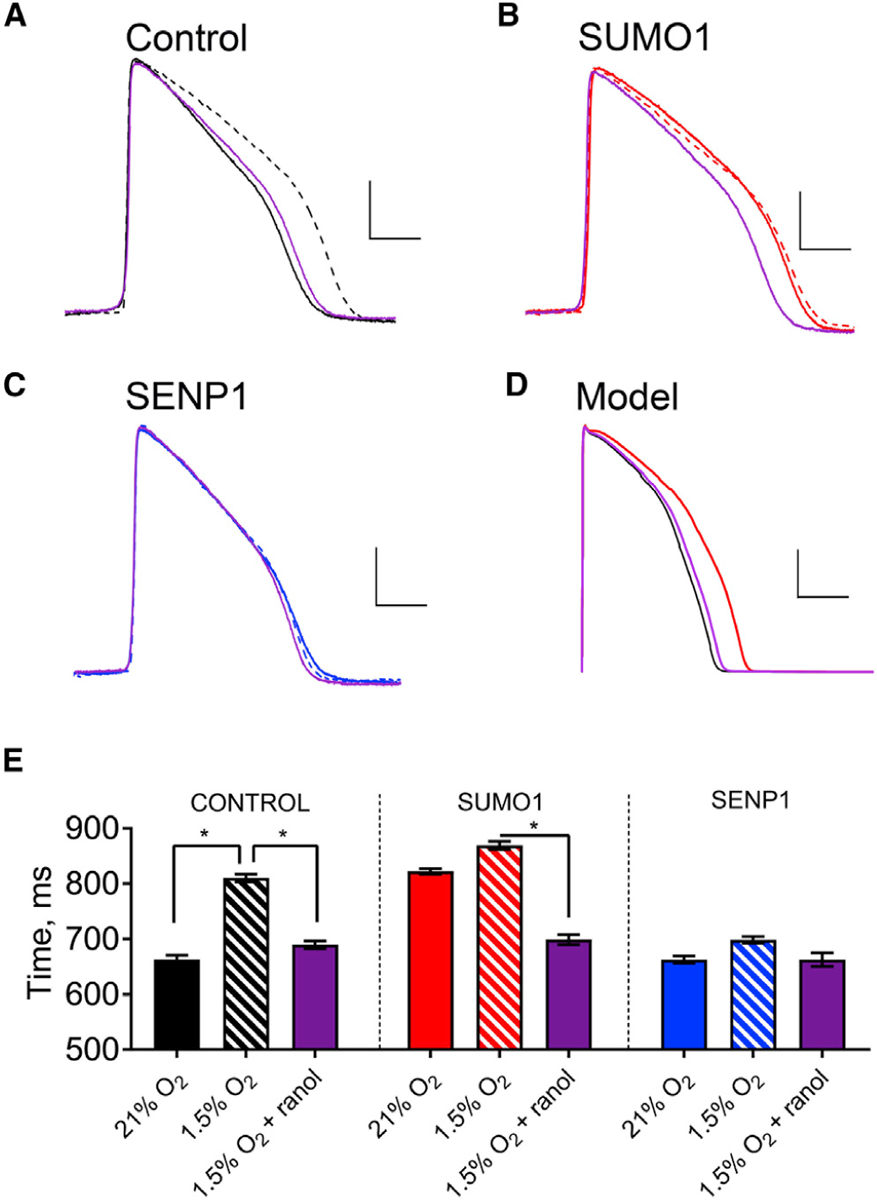
Spontaneous action potentials from human iPS-CMs were recorded in current-clamp mode with the same sequence of perfusates: normoxic (21% O2, solid line), hypoxic (1.5% O2, dashed line), and then hypoxia with 1 μM ranolazine (purple). Action potentials were studied with control intracellular solution (black) or with 1 nM SUMO1 (red) or SENP1 (blue) in the recording pipette. APD50 was determined by calculating the time required for the membrane potential to return to 50% of the resting value from the peak deflection of the action potential. Hypoxia was induced as described in the STAR Methods. Data are means ± SEM for 6–9 cells studied per group (*p < 0.01, two-way paired t test). The O’Hara-Rudy model for human action potentials was applied as described in the STAR Methods and Table S3. Scale bars represent 25 mV and 250 ms in (A)–(C) and 30 mV and 150 ms in panel (D).
(A) Examplar spontaneous action potentials recorded from iPS-CMs studied with control pipette solution under normoxic conditions and hypoxia with and without ranolazine. The APD50 increased with hypoxia by 22%, from 663 ± 2 ms to 810 ± 2 ms, and application of ranolazine restored the APD50 to 689 ± 2 ms.
(B) When SUMO1 was included in the pipette solution, APD50 was 822 ± 2 ms, and this increased to 870 ± 2 ms with hypoxia; ranolazine with hypoxia produced an APD50 of 699 ± 3 ms like that observed without SUMO1 in the pipette under normoxic conditions.
(C) APD50 was 663 ± 2 ms when cells were studied with SENP1 in the recording pipette, and the APD50 increased only to 698 ± 2 ms with hypoxia and was returned to 663 ± 4 ms with ranolazine.
(D) When a 5-fold increase in ILATE (half the maximal effect observed with hypoxia/SUMOylation), was simulated using the O’Hara-Rudy model, the APD50 increased by 27%, from 205 ms in normoxia to 260 ms.
(E) Histograms summarizing the mean APD50 of iPS-CMs under the conditions described in (A)–(C).