

Abstract
Background
Measles is the leading killer among vaccine‐preventable diseases; it is responsible for an estimated 44% of the 1.7 million vaccine‐preventable deaths among children annually.
Objectives
To assess the effects of antibiotics given to children with measles to prevent complications and reduce pneumonia, other morbidities and mortality.
Search methods
We searched CENTRAL 2013, Issue 4, MEDLINE (1966 to May week 4, 2013) and EMBASE (1980 to May 2013).
Selection criteria
Randomised controlled trials (RCTs) and quasi‐RCTs comparing antibiotics with placebo or no treatment, to prevent complications in children with measles.
Data collection and analysis
Two review authors independently extracted data and assessed trial quality.
Main results
Seven trials with 1263 children were included. The methodological quality of most studies was poor. Only two studies were randomized, double‐blind trials. There was variation in antibiotics used, their doses, schedule and evaluation of outcome. Pooled study data showed that the incidence of pneumonia was lower in the treatment group compared to the control group. However, the difference was not statistically significant. Of the 654 children who received antibiotics, 27 (4.1%) developed pneumonia; while out of 609 children in the control group, 59 (9.6%) developed pneumonia (odds ratio (OR) 0.35; 95% confidence interval (0.12 to 1.01). The one trial that showed an increase in the rate of pneumonia with antibiotics was conducted in 1942 and compared oral sulfathiazole with symptomatic treatment. If the results of this trial are removed from the meta‐analysis, there is a statistically significant reduction in the incidence of pneumonia in children receiving antibiotics (OR 0.26; 95% CI 0.12 to 0.60). The incidence of other complications was significantly lower in children receiving antibiotics: purulent otitis media (OR 0.34; 95% CI 0.16 to 0.73) and tonsillitis (OR 0.08; 95% CI 0.01 to 0.72). There was no difference in the incidence of conjunctivitis (OR 0.39; 95% CI 0.15 to 1.0), diarrhea (OR 0.53; 95% CI 0.23 to 1.22) or croup (OR 0.16; 95% CI 0.01 to 4.06). No major adverse effects attributable to antibiotics were reported.
Authors' conclusions
The studies reviewed were of poor quality and used older antibiotics. This review suggests a beneficial effect of antibiotics in preventing complications such as pneumonia, purulent otitis media and tonsillitis in children with measles. On the basis of this review, it is not possible to recommend definitive guidelines on the type of antibiotic, duration or the day of initiation. There is a need for more evidence from high‐quality RCTs to answer these questions.
Keywords: Child; Humans; Anti‐Bacterial Agents; Anti‐Bacterial Agents/therapeutic use; Conjunctivitis, Bacterial; Conjunctivitis, Bacterial/prevention & control; Croup; Croup/prevention & control; Diarrhea; Diarrhea/prevention & control; Measles; Measles/complications; Otitis Media; Otitis Media/prevention & control; Pneumonia; Pneumonia/drug therapy; Pneumonia/prevention & control; Randomized Controlled Trials as Topic; Tonsillitis; Tonsillitis/prevention & control
Plain language summary
Antibiotics for preventing complications in children with measles
Measles is an infectious disease caused by a virus. There is an effective vaccine which can prevent measles, nevertheless 30 to 40 million people worldwide still develop measles annually. Each year measles causes more than half a million deaths and is responsible for an estimated 44% of the 1.7 million vaccine‐preventable deaths among children. Measles is associated with complications such as pneumonia, ear infections, throat infections, diarrhea and conjunctivitis.
Currently, the administration of two doses of vitamin A is recommended for the prevention of these complications in children below two years of age. Another method to prevent post‐measles complications is to give antibiotics to children. The objective of this review was to assess the effects of antibiotics given to children with measles to reduce pneumonia, other morbidities and mortality. This review contains search results from May 2013 and included seven controlled clinical trials (1263 children), showed that children with measles who were given antibiotics had a lower incidence of pneumonia, ear infections and tonsillitis. However, there were no benefits for conjunctivitis or gastroenteritis. No major side effects attributable to administration of the study drugs were observed. As many of the studies were performed five decades ago with weak methodology using old antibiotics, there is a need for randomized controlled trials using newer antibiotics.
Background
Measles is an acute viral infection that is spread by respiratory secretions and is highly contagious. It is responsible for very high morbidity and mortality due to serious complications such as diarrhea, otitis media, pneumonia or encephalitis. It was the leading killer among vaccine‐preventable diseases, causing an estimated 44% of the 1.7 million vaccine‐preventable deaths among children each year (Anonymous 2002). Although it is well‐controlled in industrialised countries, intermittent outbreaks occur wherever vaccination coverage is low (Curtale 2010; Muscat 2009; Nmor 2011). The death rate from measles has declined sharply in the past decades, largely as a result of intensive vaccination efforts (Wolfson 2009). Despite this, periodic outbreaks continue to occur and may result in morbidity and mortality (Mishra 2009). Over past few years major outbreaks of measles have been reported from different parts of world (Anonymous 2013; Antona 2013; Bandyopadhyay 2013; Corbin 2013; Delaporte 2013; De Serres 2013; Ghebrehewet 2013; Grout 2013; le Roux 2012; Mishra 2012; Ntshoe 2013; Pezzotti 2013; Tricou 2013) with significant morbidity.
Description of the condition
At the beginning of 2000, it was estimated that each year measles infected 30 to 40 million people worldwide (Anonymous 2006). The annual reported incidence of measles decreased between 2000 and 2011 from 146 cases per million population to 52 per million population: a decline of 65%. Estimated measles deaths decreased from 548,300 to 157,700, amounting to a 71% decline. However, it is disturbing that between 2010 and 2011 widespread measles outbreaks have been reported in Africa, Europe, the Middle East and South East Asia (Anonymous 2013). In 2008, reported worldwide cases were at their lowest (278,417 cases). Since then reported cases have increased from 10,072 to 35,932 in the Middle East, from 186,675 to 194,364 in the South East Asian region and from 30,625 to 37,073 in European countries (Anonymous 2013). In France, over a period of four years, 22% of patients with measles required hospitalization and 12% developed complications, which included pneumonia (6.2%), acute otitis media (1.4%) hepatitis or pancreatitis (1.1%). Diarrhoea was reported in 100 cases (0.4%) (Antona 2013).
In South Africa almost 30% required hospitalization and the most common reason was pneumonia (68% of patients) (Ntshoe 2013). Case‐fatality rates of up to 20% have been documented in community studies in West Africa (Aaby 1984). Current estimates of case‐fatality rates used by the World Health Organization (WHO) in endemic countries range between 0.05% and 6% (Cairns 2010). There are reports that severe measles worsens the nutritional status of the patient for several months following the acute episode (Bhaskaram 1984; Reddy 1986) and increases morbidity and mortality (Kouadio 2010).
Description of the intervention
There is evidence that pneumonia in children with measles is often caused by bacterial infections. Histological features of bacterial pneumonia were found at autopsy in five out of 21 children in South Africa (Kaschula 1983). Bacterial pathogens as a cause of pneumonia have been isolated from lung puncture and tracheal aspirates (Dover 1975; Ellison 1931; Gremillion 1981; Morton 1986; Olson 1975; Wesley 1971). Observations at the Kingston Avenue Hospital, New York, suggested that 2.63% of 3611 children with measles died between 1935 and 1940, before antibiotics were administered, compared with only 0.74% of 1213 children in 1941, when sulfathiazole was first used (Gibel 1942). A two‐fold decline in measles‐related case fatality was documented in Niakhar, a rural area of Senegal, when all children below three years of age were treated with a one‐week course of cotrimoxazole if they were seen within two weeks of onset of illness (Samb 1995). The WHO subsequently proposed a randomized, double‐blind, placebo‐controlled trial of prophylactic antibiotics in measles as a priority for its research agenda (WHO 1995).
The risk factors associated with complications of measles and mortality include under nutrition (Caulfield 2004), young age, immune deficiency disorders, malnutrition, vitamin A deficiency, intense exposures to measles, lack of previous measles vaccination (Deivanayagam 1994; Perry 2004) and overcrowding (Burström 1999).
How the intervention might work
The evidence that pneumonia in children with measles is often caused by bacteria suggests that in countries with high case‐mortality it might be appropriate to give antibiotics to all children with measles. However, a systematic review showed no evidence for such a policy (Shann 1997). A previous review found no evidence that routine prophylaxis prevents pneumonia developing in children with upper respiratory tract infections caused by other viruses (Gadomski 1993).
Why it is important to do this review
There have been multiple reports of outbreaks of measles in different parts of the world. In this context, it is important to review the role of prophylactic antibiotics in measles to prevent complications. The last update of this review in 2011 (Kabra 2011) did not identify studies other than those included in the 2008 review (Kabra 2008). However, in the 2011 review, the data were extracted again and the quality of all the included studies was assessed using The Cochrane Collaboration's 'Risk of bias' tool (Higgins 2011).
Objectives
To assess the effects of antibiotics given to children with measles to prevent complications and reduce pneumonia, other morbidities and mortality.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) and quasi‐RCTs comparing antibiotics with placebo or no treatment, to prevent complications in children with measles. Trials had to include the development of pneumonia as one of the outcome measures.
Types of participants
We included people younger than 18 years of age of either gender.
Types of interventions
Oral or injectable antibiotics compared with no treatment or placebo.
Types of outcome measures
Primary outcomes
Incidence of pneumonia.
The definition of pneumonia was based on either clinical or radiological criteria. The clinical criteria included rapid respiration, with or without auscultatory findings. Radiological criteria included features suggestive of infiltration, with or without consolidation, and with or without pleural effusion.
Secondary outcomes
Complications such as acute gastroenteritis, diarrhea, otitis media, tonsillitis and croup. Acute gastroenteritis was defined as the occurrence of loose stools with or without vomiting and with or without dehydration. Otitis media was diagnosed on the basis of otoscopic findings of an inflamed ear drum, with or without ear discharge. Tonsillitis was diagnosed on the findings of tonsillar enlargement with or without tender cervical adenitis. Croup was diagnosed as a sudden onset of hoarseness of the voice and a dry hacking cough, or a diagnosis of croup was mentioned by the authors.
Mortality.
Search methods for identification of studies
Electronic searches
For this 2013 update we searched the Cochrane Central Register of Controlled Trials (CENTRAL) 2013, Issue 4, part of The Cochrane Library, www.thecochranelibrary.com (accessed 24 May 2013), which includes the Cochrane Acute Respiratory Infections (ARI) Group's Specialised Register, MEDLINE (2011 to May week 3, 2013) and EMBASE (2011 to May 2013). Details of previous searches are in Appendix 1.
We searched MEDLINE using keywords and MeSH terms in conjunction with the Cochrane Highly Sensitive Search Strategy for identifying randomized trials in MEDLINE: sensitivity‐ and precision‐maximising version (2008 revision); Ovid format (Lefebvre 2011) (Appendix 2). We used the same strategy to search CENTRAL and adapted it to search EMBASE (Appendix 3). We did not use any publication, language or date limitations.
Searching other resources
We searched ClinicalTrials.gov and WHO ICTRP for new and ongoing trials (24 March 2013). We checked all relevant cross‐references of studies included in the review.
Data collection and analysis
We obtained full‐text articles with the help of the Cochrane Acute Respiratory Infections (ARI) Group. We gave the papers a serial number. Two review authors (SKK, RL) independently reviewed the results for inclusion in the analysis. We resolved differences about study quality through discussion. We recorded data on a pre‐structured data extraction form. We collected data on the primary outcome (development of pneumonia) and secondary outcomes (development of acute gastroenteritis, diarrhea, otitis media, tonsillitis and croup, as well as mortality). We performed sensitivity analysis to check the importance of each study in order to see the effect of the inclusion and exclusion criteria. We computed both the effect size and summary measures with 95% confidence intervals (CIs) using RevMan 5.2 (RevMan 2012) software. We used a random‐effects model to combine the study results for all the outcome variables.
Selection of studies
Two authors (SKK, RL) checked the abstracts of all the relevant studies. The authors independently read the full texts of those suggestive of a RCT using antibiotic prophylaxis. We selected studies in children below 18 years of age, using post‐measles antibiotic prophylaxis and describing pneumonia as one of the outcomes. There was no disagreement between the authors on selection of the studies.
Data extraction and management
We prepared a form for data extraction. Two authors (RL, SKK) independently extracted data from full‐text articles. We obtained details of unclear data from authors of recent reports. One author (SKK) entered data into RevMan 5.2. Some of the data were unclear from one study; after resolving the differences by discussion, we entered the data.
Assessment of risk of bias in included studies
We assessed publication bias using The Cochrane Collaboration's 'Risk of bias' tool (Higgins 2011). We attempted to assess risk of bias by checking for adequate sequence generation, allocation concealment, blinding, incomplete outcome data addressed, and whether free of selective reporting and other bias.
1. Sequence generation: assessed as high risk, low risk or unclear
Low risk: when the study described the method used to generate the allocation sequence in sufficient detail. High risk: sequence not generated. Unclear: when it was not described or incompletely described.
2. Allocation concealment: assessed as high risk, low risk or unclear
Low risk: when the study described the method used to conceal the allocation sequence in sufficient detail. High risk: described where allocation concealment was not done. Unclear: when it was not described or incompletely described.
3. Blinding of participants, personnel and outcome assessors: assessed as high risk, low risk or unclear
Low risk: when it was a double‐blind study. High risk: when it was an unblinded study. Unclear: not clearly described.
4. Incomplete outcome data: assessed as high risk, low risk or unclear
Low risk: describe the completeness of outcome data for each main outcome, including attrition and exclusions from the analysis. High risk: not described. Unclear: incompletely described.
5. Free of selective outcome reporting: assessed as high risk, low risk or unclear
Low risk: results of study free of selective reporting. Details of all the patients enrolled in the study are included in the paper. High risk: details of all the enrolled patients not given in the paper. Unclear: details of all the enrolled patients incompletely described.
6. Other sources of bias
Among the other sources of potential bias we considered was funding agencies and their role in the study. We recorded funding agencies or pharmaceutical companies. We considered studies supported by pharmaceutical companies to be unclear unless the study defined the role of the pharmaceutical companies. We also considered studies not mentioning the source of funding as unclear under this heading.
Measures of treatment effect
The primary outcome variable was development of pneumonia in children with measles. We calculated the odds ratio (OR) for assessing risk for development of pneumonia.
Unit of analysis issues
We included only randomized controlled trials (RCTs) and quasi‐RCTs comparing antibiotics with placebo or no treatment, to prevent complications of measles in children. For studies having multiple treatment groups, we combined all those receiving antibiotics in one arm and those receiving placebo or no treatment in another arm, when the outcome assessed was similar.
Dealing with missing data
We attempted to contact the trial authors for missing data. However, we were successful for only one study (Garly 2006). This study included all age groups (children and adults) and, on request, the trial authors provided details of patients below 18 years of age. We were unable to contact the trial authors of six very old studies (Anderson 1939; Gibel 1942; Hogarth 1939; Karelitz 1951; Karelitz 1954; Prasad 1967).
Assessment of heterogeneity
We examined the homogeneity of effect sizes between pooled studies with the I2 statistic, using 25% or more as a cut‐off for exploring possible causes of heterogeneity (Higgins 2011). We used a two‐by‐two table for each study and performed Breslow's test of homogeneity to determine variation in study results for each of the outcome variables. In case of heterogeneity between the studies, we made efforts to explore the causes. We described the intervention effects using a random‐effects model throughout as there was significant heterogeneity between the studies for some of the outcomes (as evaluated by the I2 statistic).
Assessment of reporting biases
We assessed reporting biases for the studies by using funnel plots.
Data synthesis
We described the intervention effects using a random‐effects model throughout as there was significant heterogeneity between the studies for some of the outcomes (as evaluated by the I2 statistic).
Subgroup analysis and investigation of heterogeneity
None.
Sensitivity analysis
We performed a sensitivity analysis to check the importance of each study in order to see the effect of inclusion and exclusion criteria. We computed both the effect size and summary measures with 95% confidence intervals (CI).
Results
Description of studies
Results of the search
Our searches were updated in May 2013 but we did not identify any new trials for inclusion.
Included studies
We included seven controlled clinical trials on the use of antibiotics to prevent complications in children with measles. Five studies were conducted in Glasgow, London and New York between 1939 and 1954. One study was conducted in India in the 1960s and a more recent one in Bissau, Guinea‐Bissau, West Africa, was published in 2006.
The details of studies included in the review are as follows and also shown in Characteristics of included studies.
The Anderson 1939 study included 125 children (62 in the control group and 63 in the intervention group) under six years of age. The intervention included administration of sulphanilamide for 10 days or no drug to alternate patients. This was a hospital‐based study. Some of the patients already had complications such as pneumonia, otitis media etc. However, separate data for those without complications were not available in the paper. The total number of patients allocated to each group was computed by subtracting the numbers who already had complications at enrolment. Therefore, for pneumonia the number of children who were allocated to antibiotics was counted as 47 (as 16 had pneumonia at the time of enrolment) and in the control group the total enrolled without pneumonia was 49. There was no allocation concealment.
The Hogarth 1939 study included 329 children (170 in the intervention group and 159 in the control group). The intervention included administration of para‐benzylaminobenzenesulphonamide for 10 days or no treatment to alternate patients. The groups were comparable and there was no allocation concealment.
The Gibel 1942 study included 354 children below six years of age (201 in the control group and 153 in the intervention group). The intervention included administration of oral sulfathiazole until discharge or symptomatic treatment but no antibiotics. The participants were divided into two groups at the time of admission to hospital. The precise methods of randomization and allocation concealment were not mentioned in the trial. Separate data for those who already had pneumonia were not mentioned in the paper. However, the numbers of uncomplicated cases (we presume children without pneumonia) in the intervention and control groups at the time of enrolment were 82 and 148, respectively.
The Karelitz 1951 study enrolled 132 children below nine years of age admitted to hospital. The intervention included administration of chlortetracycline (Aureomycin) (45 children), penicillin (44 children) and no active treatment (43 children). The first 15 participants received antibiotics followed by alternate allocation to receive no active intervention. The method of randomization or allocation concealment was not described by the trial authors. For the purpose of comparison, we analyzed the penicillin and chlortetracycline groups together. No patients in either group had pneumonia at time of enrolment therefore the total number of patients available for assessment of the primary outcome (pneumonia) was 89 for the intervention group and 43 for the control group.
The Karelitz 1954 study enrolled 256 children below 10 years of age. The intervention included the administration of a single dose of Benzethacil (61 participants), aqueous procaine penicillin (67 participants) for four days or aqueous procaine penicillin on day 0, 3 and day 6 (47 participants). The control group (81 participants) did not receive any antibiotics. There was no allocation concealment. For the purpose of analysis, children receiving benzathine penicillin (61) and four doses of aqueous procaine penicillin (67) and those receiving three doses of aqueous procaine penicillin (47 participants) were analyzed together to form the intervention group (175). In the intervention group 19 patients already had pneumonia. Therefore the number of children available for assessment of the primary outcome (pneumonia) was 156 in the intervention group and 81 in the control group.
The Prasad 1967 study enrolled 158 children (80 in the control group and 78 in the intervention group). Intervention included administration of placebo or tetracycline for seven days. The study included participants admitted to hospital as well as ambulatory participants. There was no mention of loss to follow‐up.
We obtained additional data on children less than 18 years of age from the authors of the Garly 2006 study as the published study gave data for participants less than 25 years of age. The Garly study enrolled 81 participants with measles below 18 years of age during a measles epidemic in Bissau in 1998. Interventions included sulfamethoxazole‐trimethoprim (co‐trimoxazole (N = 44)) or placebo for seven days (N = 37). This was a randomized, double‐blind, placebo‐controlled trial; this is the only methodologically sound trial.
None of the included studies used vitamin A in children with measles.
Excluded studies
Three published studies were excluded from the review because they were not controlled trials. Thompson 1938 reported that 1.7% of 352 children treated with an antibiotic and 4.8% of 762 controls developed bronchopneumonia. On the other hand, Weinstein 1955 found pneumonia at the time of admission to hospital in 21.5% of 130 children who had been treated with an antibiotic and 8.1% of 298 children who had not had an antibiotic. In Senegal the case‐mortality from measles fell substantially after an increase in measles immunisation and administration of co‐trimoxazole to all children less than three years of age who had measles (Samb 1995). See Characteristics of excluded studies.
Risk of bias in included studies
All but two studies were unblinded (Garly 2006; Prasad 1967) and only two studies mentioned withdrawals from the trial (Anderson 1939; Garly 2006). Only one study (Garly 2006) provided information about antibiotic treatment given before randomization and these children were not enrolled in the study. We assessed the quality of studies using The Cochrane Collaboration's 'Risk of bias' tool (Higgins 2011). The overall risk of bias is presented graphically in Figure 1 and summarised in Figure 2.
1.
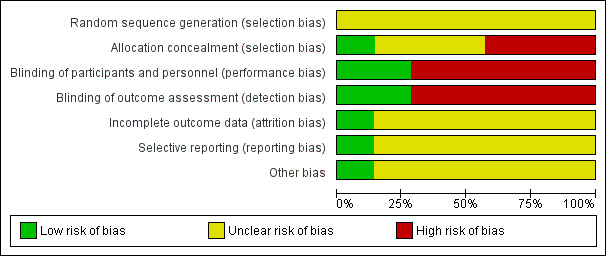
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
2.
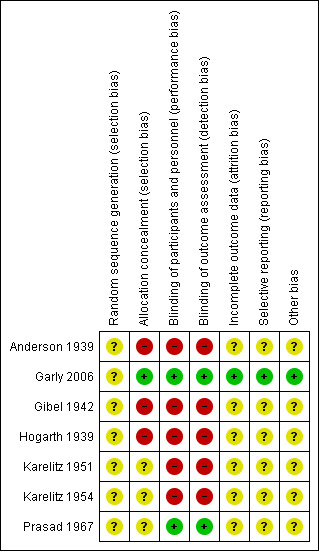
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Generation of allocation sequence and concealment was described in two studies (Garly 2006; Prasad 1967). In the remaining five studies (Anderson 1939; Gibel 1942; Hogarth 1939; Karelitz 1951; Karelitz 1954) it was not very clear.
Blinding
Blinding was done in two studies only (Garly 2006; Prasad 1967). All other studies were not blinded.
Incomplete outcome data
Outcome data on all the patients who did not have pneumonia at time of enrolment were available in one study (Garly 2006). In other studies, data were extracted from available information. They randomized children with complications. Separate data for those who did not have complications and those who had complications were not clearly defined in six studies.
Selective reporting
All but one study reported outcomes completely (Garly 2006).
Other potential sources of bias
One study received support for blood analysis from the Medical Research Council Laboratory in Gambia (Garly 2006). Two studies (Hogarth 1939; Prasad 1967) received support in the form of drugs from pharmaceutical companies. However, the role in the trials is not clearly defined. Funding sources could not be identified in the rest of the studies (Anderson 1939; Gibel 1942; Karelitz 1951; Karelitz 1954).
Effects of interventions
Primary outcome
1. Incidence of pneumonia
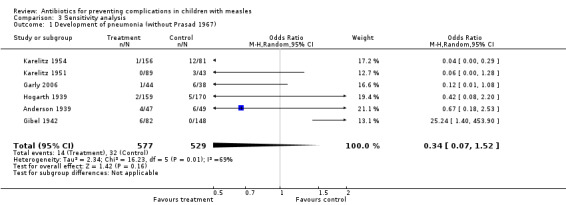
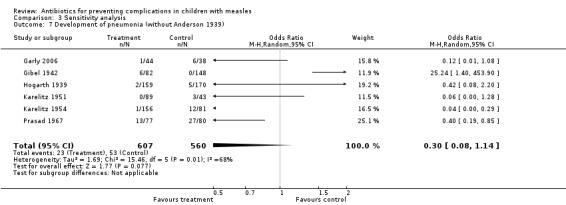
A total of seven studies including 1263 children (654 in the intervention group and 609 in the control group) were included in the study. A total of 86 children (27 in the intervention group and 59 in the control group) developed pneumonia. Two studies (Karelitz 1954; Prasad 1967) showed a significant reduction in the incidence of pneumonia, while one study (Gibel 1942) showed an increased incidence. In four studies (Anderson 1939; Garly 2006; Hogarth 1939; Karelitz 1951) there was a decrease in the incidence of pneumonia but it did not reach statistical significance. Pooled study data showed that the incidence of pneumonia was lower in the treatment group compared to the control group. Out of 654 children who received antibiotics, 27 (4.1%) developed pneumonia, while out of 609 children in the control group, 59 (9.6%) developed pneumonia (odds ratio (OR) 0.35; 95% confidence interval (CI) 0.12 to 1.01) (Analysis 1.1). All the studies showed a decrease in the incidence of pneumonia with the use of antibiotics, except one study (Gibel 1942). This study included 230 children (82 in the intervention group and 148 in the control group). Six children out of 82 developed pneumonia in the intervention group as compared to no pneumonia in 148 children who received only supportive care. If the results of this study (Gibel 1942) are dropped from the analysis, there is a significant reduction in the occurrence of pneumonia in children receiving antibiotics (OR 0.26; 95% CI 0.12 to 0.60) (Analysis 3.5)
1.1. Analysis.
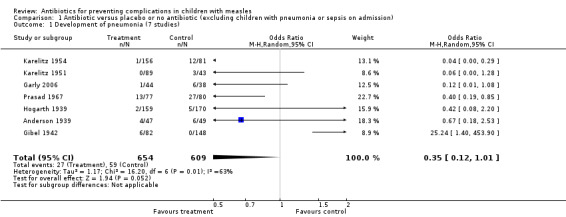
Comparison 1 Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission), Outcome 1 Development of pneumonia (7 studies).
3.5. Analysis.
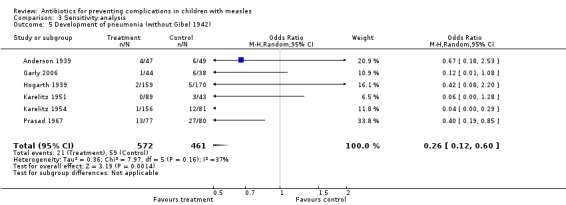
Comparison 3 Sensitivity analysis, Outcome 5 Development of pneumonia (without Gibel 1942).
Secondary outcomes
1. Complications
Diarrhoea
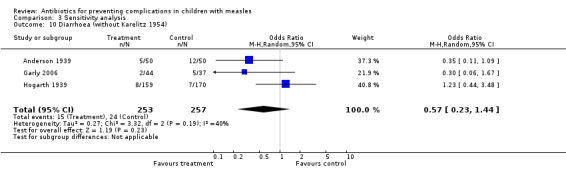
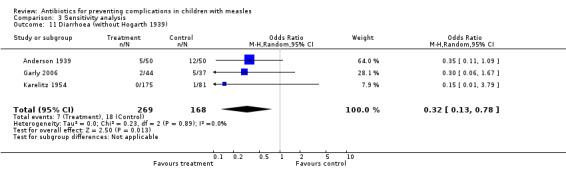
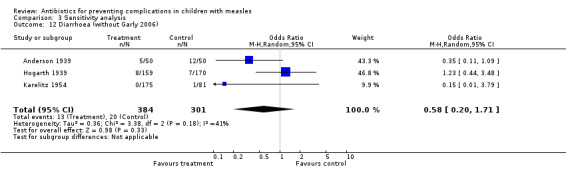
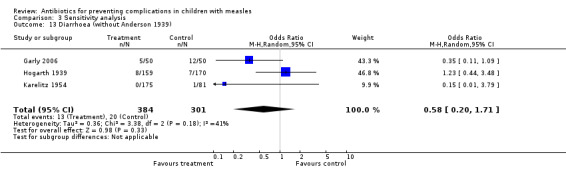
Data on the development of diarrhea were available in four studies (Anderson 1939; Garly 2006; Hogarth 1939; Karelitz 1954). There was no significant effect on the development of diarrhea with antibiotics (OR 0.53; 95% CI 0.23 to 1.22) (Analysis 1.2). In the Garly 2006 study, two children in the antibiotic group developed diarrhea compared with five children in the placebo group.
1.2. Analysis.
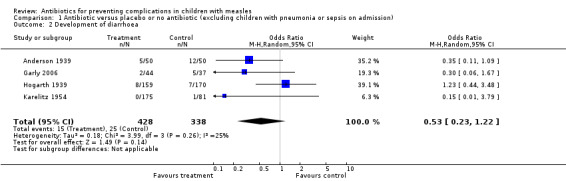
Comparison 1 Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission), Outcome 2 Development of diarrhoea.
Conjunctivitis
Data on the development of conjunctivitis were available in two studies (Garly 2006; Karelitz 1951). There was no significant difference in the development of conjunctivitis in the two groups (OR 0.39; 95% CI 0.15 to 1.0) (Analysis 1.3). In the Garly 2006 study, 11 children in the antibiotic group developed conjunctivitis compared to 17 children in the placebo group.
1.3. Analysis.
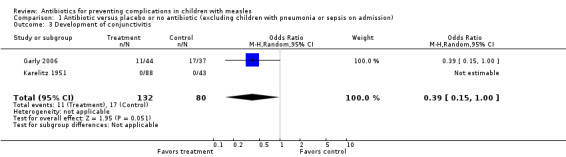
Comparison 1 Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission), Outcome 3 Development of conjunctivitis.
Otitis media
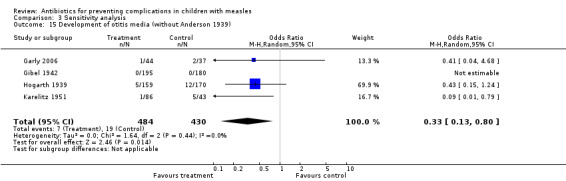
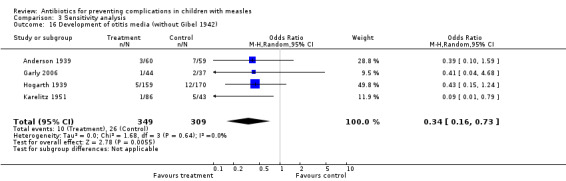
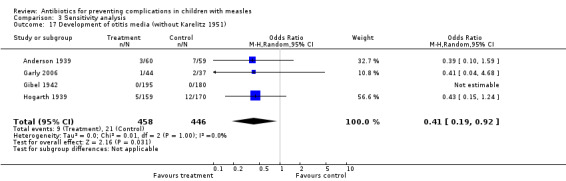
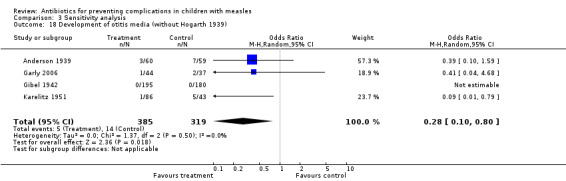
Data on purulent otitis media were available in five studies (Anderson 1939; Garly 2006; Gibel 1942; Hogarth 1939; Karelitz 1951). Two studies reported catarrhal otitis media; these data were not included in the analysis. The incidence of otitis media was lower in children treated with antibiotics (OR 0.34; 95% CI 0.16 to 0.73) (Analysis 1.4). Of the 1.8% of children who received antibiotics, 5.3% developed purulent otitis media. None of the studies were found to alter the results in the other direction when the analysis was done by dropping one study at a time. In the Garly 2006 study one child in the antibiotic group developed otitis media compared with two children in the placebo group.
1.4. Analysis.
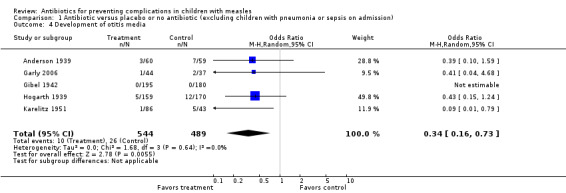
Comparison 1 Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission), Outcome 4 Development of otitis media.
Croup
Data on the development of croup were available in one study (Karelitz 1951) and there was no significant difference between the two groups (OR 0.16; 95% CI 0.01 to 4.06) (Analysis 1.5).
1.5. Analysis.
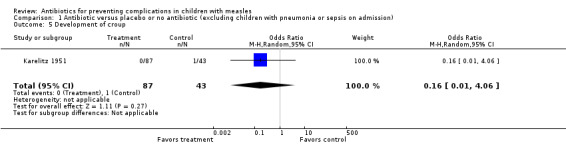
Comparison 1 Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission), Outcome 5 Development of croup.
Tonsillitis and pharyngitis
Data on the development of tonsillitis or pharyngitis were available in two studies (Anderson 1939; Karelitz 1951) and showed a reduction in the incidence of tonsillitis in children receiving antibiotics (OR 0.08; 95% CI 0.01 to 0.72) (Analysis 1.6).
1.6. Analysis.
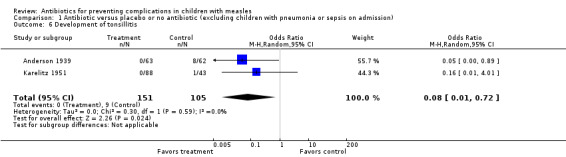
Comparison 1 Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission), Outcome 6 Development of tonsillitis.
2. Mortality
The mortality rate was 0.49% in children receiving antibiotics compared to 0.14% in the control group. The difference was not significant (OR 3.04; 95% CI 0.47 to 19.63) (Analysis 1.7). In the Garly 2006 study, no deaths were reported.
1.7. Analysis.
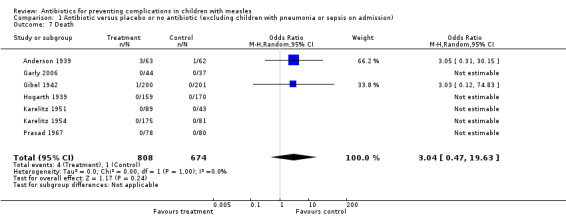
Comparison 1 Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission), Outcome 7 Death.
Baseline characteristics of participants
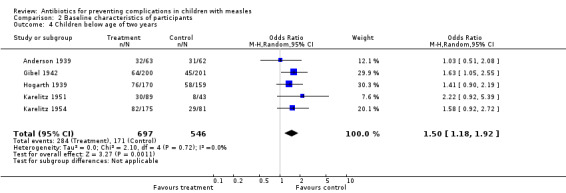
The median age of participants in the control and intervention groups was not provided in all of the studies. The number of children below two years of age was available in five studies (Anderson 1939; Gibel 1942; Hogarth 1939; Karelitz 1951; Karelitz 1954). The groups were not equally distributed ‐ in the intervention group there were more children below two years of age (OR 1.50; 95% CI 1.18 to 1.92).
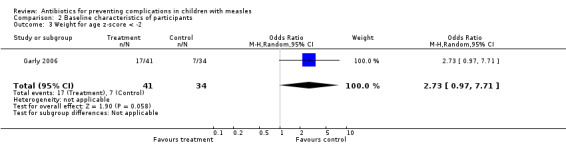
Gender distribution was described separately for the two groups in three studies (Anderson 1939; Garly 2006; Gibel 1942) and was comparable in two groups (OR 1.15; 95% CI 0.69 to 1.91). The nutritional status was available in one study (Garly 2006) and it was comparable (OR 2.73; 95% CI 0.97 to 7.71) in the two groups.
Side effects of antibiotics
Side effects attributable to the study drugs were specifically reported in two studies (Gibel 1942; Karelitz 1951). Two children developed erythema nodosum after receiving sulfathiazole (Gibel 1942). In the other study (Karelitz 1951), 13 children developed vomiting after administration of chlortetracycline two to three days after initiation of treatment and three children developed diarrhea; both side effects were self limiting and did not require discontinuation of therapy. Five studies (Anderson 1939; Garly 2006; Hogarth 1939; Karelitz 1954; Prasad 1967) did not report any specific side effects attributable to the study drugs.
Discussion
This systematic review suggests that antibiotics administered to children with measles decrease the incidence of otitis media and tonsillitis and show a trend towards decreasing the incidence of pneumonia (OR 0.35; 95% CI 0.12 to 1.01). One study (Gibel 1942) that showed an increase in pneumonia was removed in a sensitivity analysis which resulted in a statistically significant reduction in the rate of pneumonia.
Given the overall results, however, this result cannot be relied upon and further trials are necessary to confirm the beneficial effects seen, particularly in the latest and most rigorous trial. Similarly, to prevent one case of otitis media, we need to treat 24 patients. Antibiotics did not affect the development of diarrhea, conjunctivitis, croup or mortality. Only one study (Garly 2006) was a well‐conducted randomized controlled trial (RCT); the remaining six studies scored poorly in quality assessment. In a pooled analysis, all the studies favoured the treatment group for prevention of pneumonia except for the Gibel 1942 study; the effect size reached significance when the Gibel 1942 study was dropped from the analysis. In the Gibel study, a total of 153 children were enrolled in the treatment group compared to 201 in the no treatment group; however, the numbers of uncomplicated cases (we presume children without pneumonia) in the intervention and control groups at the time of enrolment were 82 and 148, respectively. The number of children below two years of age was higher in the treatment group compared to the no treatment group (64 versus 45). Separate data for the development of pneumonia in children below two years of age were not available. Age is one of the risk factors for pneumonia; as the participants were young, age may have affected the results in this study.
Of the seven studies included in the review, only one (Garly 2006) provided data on malnutrition. In this study, the number of children with a weight for age z‐score of below ‐2 was higher in the intervention group compared to the control group. However, the incidence of pneumonia was higher in the control group, suggesting a benefit from cotrimoxazole in malnourished children. In other studies, data on the distribution of malnourished children in the two groups were not available.
Children who develop measles below two years of age have a higher incidence of diarrhea, pneumonia and otitis media (Deivanayagam 1994; Perry 2004). The number of children below two years of age was higher in the antibiotics group compared to the control group in this review. Although we could not find an analysis of children below two years of age and above two years for the development of different morbidities, the incidence of pneumonia and otitis media was significantly lower in the treatment group compared to the control group, indirectly suggesting benefits from antibiotics in the younger age group.
Data on immune deficiency, vitamin A deficiency, intense exposure to measles and a lack of measles vaccination were not available in the included studies and therefore could not be compared in this review.
The only other intervention that may improve the outcome in children with measles is the supplementation of two doses of vitamin A (200,000 IU) on consecutive days. This was associated with a reduction in the risk of mortality in children under the age of two years (risk ratio (RR) 0.21; 95% CI 0.07 to 0.66) and a reduction in the risk of pneumonia‐specific mortality (RR 0.57; 95% CI 0.24 to 1.37) (Yang 2011).
The main limitation of this review was that the seven controlled trials included a total of 1385 children with a relatively low number of complications (54 cases of pneumonia, 40 of diarrhea, 28 of conjunctivitis, 36 of otitis media and five deaths). Only one trial was of good quality and the other six trials were poorly designed; randomization was not described or was by alternate allocation, all but two were unblinded and little information was provided about withdrawals. Only one of the trials (Anderson 1939) had a mortality of 1% or more, although two others (Gibel 1942; Hogarth 1939) were conducted in communities where the mortality had been more than 1% in the immediately preceding years, when antibiotics were not available. The selection of cases for antibiotics in these trials was not very strict. Even though we tried to include only those children without complications at the time of study enrolment, we cannot be absolutely sure about the 'contamination' of groups. It appears that the children were observed only for a limited period of time, for example, during the hospital stay; only one study observed children up to one month (Garly 2006). The other important limitation of the review is that most of the studies were carried out before the introduction of vitamin A. Since vitamin A may influence the outcome of measles, including the development of morbidities, more studies are needed to evaluate the efficacy of antibiotics in association with vitamin A.
The diagnosis of measles was made on a clinical basis in the majority of patients analyzed in the review. Serological diagnostic confirmation of measles was attempted in one study (Garly 2006). The use of clinical criteria only to diagnose measles may have lead to the inclusion of bacterial infections that mimic measles.
A variety of antibiotics such as sulphonamide, penicillin, tetracycline and co‐trimoxazole were used. All the studies except one were conducted before 1970. The effect of antibiotics will depend on the organisms and their sensitivity patterns. Whether newer antibiotics will give similar results remains to be seen. Also, there was variability in the time antibiotics were started and the duration of treatments. Most studies used antibiotics for a duration of up to 10 days or until discharge from hospital. These observations prevent the review authors from recommending a particular antibiotic regimen to prevent complications of measles. The most recent study included in the review (Garly 2006) used co‐trimoxazole and found it to be effective. Among the antibiotics used in earlier studies that are still used in clinical practice, penicillin was also effective.
The studies reviewed here provide evidence that administration of antibiotics in children with measles reduces the incidence of pneumonia, otitis media and tonsillitis. There was no effect on death rates, conjunctivitis, croup or diarrhea.
Summary of main results
In this review, we included seven clinical trials; studies were of poor quality except for one RCT. All the studies used less effective antimicrobial agents. The time and schedule of administration of antibiotics was variable. Results suggest that antibiotics after development of measles may reduce the incidence of otitis media and tonsillitis. However, the reduction in incidence of pneumonia is not significant. From the present evidence it is difficult to suggest drug, dose and timings of administration of antibiotics for children with measles.
Overall completeness and applicability of evidence
The present set of evidence is not sufficient for recommending the use of antibiotics for reducing complications in children with measles.
Quality of the evidence
The quality of evidence is poor and only two studies were randomized, double‐blind trials. There was variation in the antibiotics used, their doses, schedule and evaluation of outcome. Therefore, no recommendations can be made from the current evidence.
Potential biases in the review process
All the available studies were included for review. We tried to search published literature as completely as possible; we retrieved full‐text articles for studies published in the 1930s and 1940s. There was significant heterogeneity. We tried to check for publication bias using a funnel plot. We performed a sensitivity analysis to see the effect of each study on the main outcome. The studies included children who had already developed complications before enrolment in the study. We tried to exclude children who had pneumonia at the time of enrolment from analysis of the primary outcome. Clarification about the data or incomplete data could not be obtained from authors, except in one study, as most studies were carried out before 1960. The quality of reporting and analysis was poor by today's standard.
Agreements and disagreements with other studies or reviews
The findings are in agreement with the other reviews on the subject (Shann 1997)
Authors' conclusions
Implications for practice.
Measles is a public health problem in some parts of the world. This review suggests that there is a beneficial effect of antibiotic administration for children with measles in reducing the incidence of complications such as pneumonia, otitis media and tonsillitis. There is no consensus as to the type of antibiotics, duration, time of antibiotic initiation or dosage in this review, although penicillin and co‐trimoxazole were found to be effective. There is a need to generate more data from well‐planned randomized controlled trials (RCTs) to answer these questions.
Implications for research.
This review suggests a benefit in giving antibiotics to children with measles to reduce complications. In view of the heterogeneity of the interventions and the poor methodological quality of most of the included studies (conducted more than five decades ago), there is a need for well‐designed RCTs to evaluate the effect of antibiotics in reducing pneumonia and other morbidities. Further trials are needed to evaluate the type and duration of antibiotics which are known to be effective. Available evidence suggests that two doses of vitamin A given to children below two years of age with measles may reduce mortality. However, none of the studies in this review gave vitamin A to children with measles. Vitamin A may modify the course of the illness and therefore there is a need to include vitamin A administration while conducting clinical trials for post‐measles complications.
What's new
| Date | Event | Description |
|---|---|---|
| 24 May 2013 | New citation required but conclusions have not changed | Additional information on measles outbreaks included in the update. |
| 24 May 2013 | New search has been performed | Searches updated; no new trials were included in the update. |
History
Protocol first published: Issue 2, 1999 Review first published: Issue 1, 2010
| Date | Event | Description |
|---|---|---|
| 7 April 2011 | New search has been performed | Searches conducted. No new trials were identified in this updated review. |
| 5 August 2010 | Amended | Contact details updated. |
| 21 January 2010 | Amended | Contact details updated. |
| 16 January 2008 | Amended | Converted to new review format. |
| 4 January 2008 | New citation required and conclusions have changed | Change in authors. |
| 4 January 2008 | New search has been performed | Searches conducted. |
| 27 February 2001 | New search has been performed | Searches conducted. |
| 17 August 1999 | New search has been performed | Searches conducted. Feedback added. |
| 9 December 1998 | New search has been performed | Searches conducted. |
Notes
This review, formerly titled 'Antibiotics for preventing pneumonia in children with measles' was withdrawn from The Cochrane Library, 2006, Issue 3 as the review authors could no longer update it. It was taken over by a new team of authors in 2006 and completed in March 2008. In this update the title of the review was changed to 'Antibiotics for preventing complications in children with measles', as complications other than pneumonia were also evaluated.
Acknowledgements
We acknowledge the authors of the original Cochrane Review: Frank Shann, Rennie D'Souza and Ron D'Souza; the help provided by the All India Institute of Medical Sciences, New Delhi, in providing access to the Internet; help provided by Liz Dooley (Managing Editor) and Sarah Thorning (Trials Search Co‐ordinator) with conducting the EMBASE search and obtaining full‐text articles; and Dr RM Pandey, Department of Biostatistics, All India Institute of Medical Sciences, New Delhi for statistical advice. We acknowledge the contributions of Deborah J Hilton in the last update of this review (Kabra 2008).
We acknowledge Sarah Thorning (Trial Search Co‐ordinator for the ARI Group) for doing the EMBASE search for this latest update. Thanks also to the following for commenting on previous drafts: Irénée Domkam Kammogne, Cheryl Flynn, Mark Jones and Jenny Doust.
Appendices
Appendix 1. Details of previous searches
For the 2011 update we searched the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2011, Issue 1), which includes the Cochrane Acute Respiratory Infections (ARI) Group's Specialised Register, MEDLINE (January 2008 to March week 4, 2011) and EMBASE (December 2007 to April 2011).
In the 2007 update we searched the Cochrane Central Register of Controlled Trials (The Cochrane Library 2008, Issue 1) which includes the Cochrane Acute Respiratory Infections (ARI) Group's Specialised Register, MEDLINE (1966 to January week 1, 2008), EMBASE (1980 to December 2007) and the National Research Register (Issue 3, 2007).
We searched MEDLINE using the following keywords and MeSH terms in conjunction with the highly sensitive search strategy designed by The Cochrane Collaboration for identifying controlled trials (Dickersin 1994). We used the same strategy to search CENTRAL and adapted it to search EMBASE.
MEDLINE (OVID) #1. exp MEASLES/ #2. exp MEASLES VIRUS/ #3. measles.mp. #4. or/1‐3 #5. exp Anti‐Bacterial Agents/ #6. antibiotic$.mp. #7. exp QUINOLONES/ #8. quinolone$.mp. #9. exp SULFONAMIDES/ #10. sulfonamide$.mp. #11. exp PENICILLINS #12. penicillin$.mp. #13. exp MACROLIDES #14. macrolide$.mp. #15. 0r/5‐14 #16. 4 and 15
EMBASE (EMBASE.Com) #1. 'measles'/exp AND [embase]/lim #2. 'measles virus'/exp AND [embase]/lim #3. measles:ti,ab AND [embase]/lim #4. #1 OR #2 OR #3 #5. 'antibiotic agent'/exp AND [embase]/lim #6. antibiotic*:ti,ab AND [embase]/lim #7. 'quinolone derivative'/exp AND [embase]/lim #8. quinolone*:ti,ab AND [embase]/lim #9. 'sulfonamide'/exp AND [embase]/lim #10. sulfonamide*:ti,ab AND [embase]/lim #11. 'penicillin derivative'/exp AND [embase]/lim #12. penicillin*:ti,ab AND [embase]/lim #13. 'macrolide'/exp AND [embase]/lim #14. macrolide*:ti,ab AND [embase]/lim #15. #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 #16. #4 AND #15
Appendix 2. MEDLINE search strategy
1 exp Measles/ 2 exp Measles virus/ 3 measles*.tw. 4 or/1‐3 5 exp Anti‐Bacterial Agents/ 6 Antibiotic Prophylaxis/ 7 antibiotic*.tw. 8 exp Quinolones/ 9 quinolone*.tw,nm. 10 exp Sulfonamides/ 11 sulfonamide*.tw,nm. 12 exp Penicillins/ 13 penicillin*.tw,nm. 14 exp Macrolides/ 15 macrolide*.tw,nm. 16 or/5‐15 17 4 and 16
Appendix 3. Embase.com search strategy
#19 #11 AND #18 #18 #14 NOT #17 #17 #16 NOT #15 #16 [animals]/lim #15 'human'/exp #14 #12 OR #13 #13 random*:ab,ti OR placebo*:ab,ti OR crossover*:ab,ti OR 'cross over':ab,ti OR allocat*:ab,ti OR (singl* OR doubl*) NEAR/1 blind* OR trial:ti #12 'randomized controlled trial'/exp OR 'single blind procedure'/exp OR 'double blind procedure'/exp OR 'crossover procedure'/exp #11 #4 AND #10 #10 #5 OR #6 OR #7 OR #8 OR #9 #9 quinolone*:ab,ti OR sulfonamide*:ab,ti OR penicillin*:ab,ti OR macrolide*:ab,ti #8 'quinolone derivative'/exp OR 'sulfonamide'/exp OR 'penicillin derivative'/exp OR 'macrolide'/exp #7 'antibiotic prophylaxis'/de #6 antibiotic*:ab,ti #5 'antibiotic agent'/exp #4 #1 OR #2 OR #3 #3 measles:ab,ti OR rubeola:ab,ti OR rubeolla:ab,ti OR morbilli*:ab,ti #2 'measles virus'/de #1 'measles'/de
Data and analyses
Comparison 1. Antibiotic versus placebo or no antibiotic (excluding children with pneumonia or sepsis on admission).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Development of pneumonia (7 studies) | 7 | 1263 | Odds Ratio (M‐H, Random, 95% CI) | 0.35 [0.12, 1.01] |
| 2 Development of diarrhoea | 4 | 766 | Odds Ratio (M‐H, Random, 95% CI) | 0.53 [0.23, 1.22] |
| 3 Development of conjunctivitis | 2 | 212 | Odds Ratio (M‐H, Random, 95% CI) | 0.39 [0.15, 1.00] |
| 4 Development of otitis media | 5 | 1033 | Odds Ratio (M‐H, Random, 95% CI) | 0.34 [0.16, 0.73] |
| 5 Development of croup | 1 | 130 | Odds Ratio (M‐H, Random, 95% CI) | 0.16 [0.01, 4.06] |
| 6 Development of tonsillitis | 2 | 256 | Odds Ratio (M‐H, Random, 95% CI) | 0.08 [0.01, 0.72] |
| 7 Death | 7 | 1482 | Odds Ratio (M‐H, Random, 95% CI) | 3.04 [0.47, 19.63] |
Comparison 2. Baseline characteristics of participants.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Median age | 1 | 84 | Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Male sex | 3 | 607 | Odds Ratio (M‐H, Random, 95% CI) | 1.15 [0.69, 1.91] |
| 3 Weight for age z‐score < ‐2 | 1 | 75 | Odds Ratio (M‐H, Random, 95% CI) | 2.73 [0.97, 7.71] |
| 4 Children below age of two years | 5 | 1243 | Odds Ratio (M‐H, Random, 95% CI) | 1.50 [1.18, 1.92] |
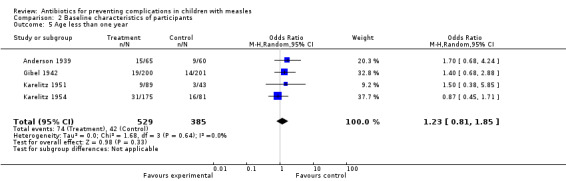
| 5 Age less than one year | 4 | 914 | Odds Ratio (M‐H, Random, 95% CI) | 1.23 [0.81, 1.85] |
2.1. Analysis.
Comparison 2 Baseline characteristics of participants, Outcome 1 Median age.
2.2. Analysis.
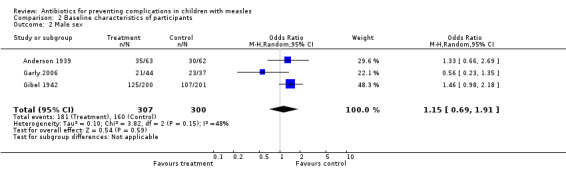
Comparison 2 Baseline characteristics of participants, Outcome 2 Male sex.
2.3. Analysis.
Comparison 2 Baseline characteristics of participants, Outcome 3 Weight for age z‐score < ‐2.
2.4. Analysis.
Comparison 2 Baseline characteristics of participants, Outcome 4 Children below age of two years.
2.5. Analysis.
Comparison 2 Baseline characteristics of participants, Outcome 5 Age less than one year.
Comparison 3. Sensitivity analysis.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Development of pneumonia (without Prasad 1967) | 6 | 1106 | Odds Ratio (M‐H, Random, 95% CI) | 0.34 [0.07, 1.52] |
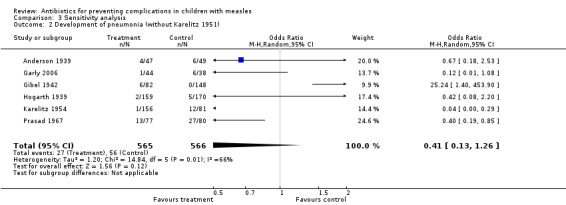
| 2 Development of pneumonia (without Karelitz 1951) | 6 | 1131 | Odds Ratio (M‐H, Random, 95% CI) | 0.41 [0.13, 1.26] |
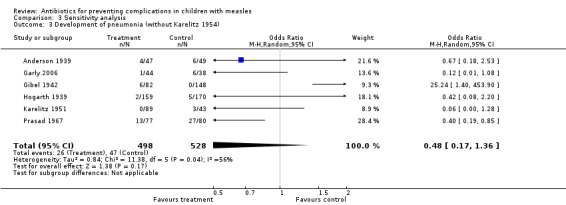
| 3 Development of pneumonia (without Karelitz 1954) | 6 | 1026 | Odds Ratio (M‐H, Random, 95% CI) | 0.48 [0.17, 1.36] |
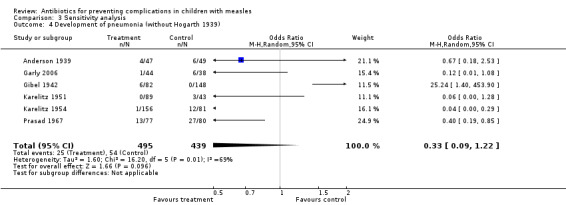
| 4 Development of pneumonia (without Hogarth 1939) | 6 | 934 | Odds Ratio (M‐H, Random, 95% CI) | 0.33 [0.09, 1.22] |
| 5 Development of pneumonia (without Gibel 1942) | 6 | 1033 | Odds Ratio (M‐H, Random, 95% CI) | 0.26 [0.12, 0.60] |
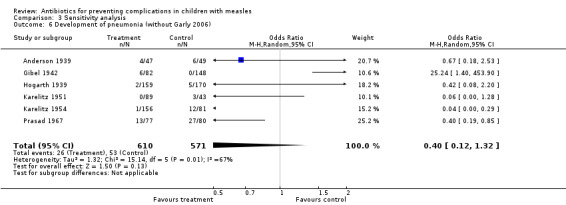
| 6 Development of pneumonia (without Garly 2006) | 6 | 1181 | Odds Ratio (M‐H, Random, 95% CI) | 0.40 [0.12, 1.32] |
| 7 Development of pneumonia (without Anderson 1939) | 6 | 1167 | Odds Ratio (M‐H, Random, 95% CI) | 0.30 [0.08, 1.14] |
| 8 Death (without Gibel 1942) | 6 | 1021 | Odds Ratio (M‐H, Random, 95% CI) | 3.05 [0.31, 30.15] |
| 9 Death (without Anderson 1939) | 6 | 1357 | Odds Ratio (M‐H, Random, 95% CI) | 2.06 [0.21, 19.94] |
| 10 Diarrhoea (without Karelitz 1954) | 3 | 510 | Odds Ratio (M‐H, Random, 95% CI) | 0.57 [0.23, 1.44] |
| 11 Diarrhoea (without Hogarth 1939) | 3 | 437 | Odds Ratio (M‐H, Random, 95% CI) | 0.32 [0.13, 0.78] |
| 12 Diarrhoea (without Garly 2006) | 3 | 685 | Odds Ratio (M‐H, Random, 95% CI) | 0.58 [0.20, 1.71] |
| 13 Diarrhoea (without Anderson 1939) | 3 | 685 | Odds Ratio (M‐H, Random, 95% CI) | 0.58 [0.20, 1.71] |
| 14 Development of otitis media (without Garly 2006) | 4 | 952 | Odds Ratio (M‐H, Random, 95% CI) | 0.34 [0.15, 0.75] |
| 15 Development of otitis media (without Anderson 1939) | 4 | 914 | Odds Ratio (M‐H, Random, 95% CI) | 0.33 [0.13, 0.80] |
| 16 Development of otitis media (without Gibel 1942) | 4 | 658 | Odds Ratio (M‐H, Random, 95% CI) | 0.34 [0.16, 0.73] |
| 17 Development of otitis media (without Karelitz 1951) | 4 | 904 | Odds Ratio (M‐H, Random, 95% CI) | 0.41 [0.19, 0.92] |
| 18 Development of otitis media (without Hogarth 1939) | 4 | 704 | Odds Ratio (M‐H, Random, 95% CI) | 0.28 [0.10, 0.80] |
3.1. Analysis.
Comparison 3 Sensitivity analysis, Outcome 1 Development of pneumonia (without Prasad 1967).
3.2. Analysis.
Comparison 3 Sensitivity analysis, Outcome 2 Development of pneumonia (without Karelitz 1951).
3.3. Analysis.
Comparison 3 Sensitivity analysis, Outcome 3 Development of pneumonia (without Karelitz 1954).
3.4. Analysis.
Comparison 3 Sensitivity analysis, Outcome 4 Development of pneumonia (without Hogarth 1939).
3.6. Analysis.
Comparison 3 Sensitivity analysis, Outcome 6 Development of pneumonia (without Garly 2006).
3.7. Analysis.
Comparison 3 Sensitivity analysis, Outcome 7 Development of pneumonia (without Anderson 1939).
3.8. Analysis.
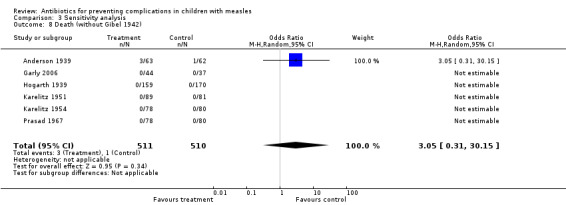
Comparison 3 Sensitivity analysis, Outcome 8 Death (without Gibel 1942).
3.9. Analysis.
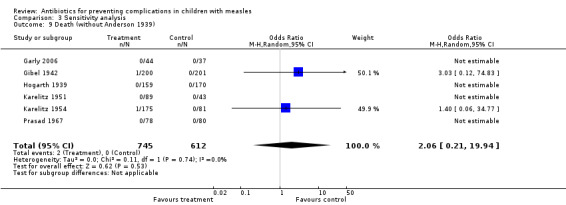
Comparison 3 Sensitivity analysis, Outcome 9 Death (without Anderson 1939).
3.10. Analysis.
Comparison 3 Sensitivity analysis, Outcome 10 Diarrhoea (without Karelitz 1954).
3.11. Analysis.
Comparison 3 Sensitivity analysis, Outcome 11 Diarrhoea (without Hogarth 1939).
3.12. Analysis.
Comparison 3 Sensitivity analysis, Outcome 12 Diarrhoea (without Garly 2006).
3.13. Analysis.
Comparison 3 Sensitivity analysis, Outcome 13 Diarrhoea (without Anderson 1939).
3.14. Analysis.

Comparison 3 Sensitivity analysis, Outcome 14 Development of otitis media (without Garly 2006).
3.15. Analysis.
Comparison 3 Sensitivity analysis, Outcome 15 Development of otitis media (without Anderson 1939).
3.16. Analysis.
Comparison 3 Sensitivity analysis, Outcome 16 Development of otitis media (without Gibel 1942).
3.17. Analysis.
Comparison 3 Sensitivity analysis, Outcome 17 Development of otitis media (without Karelitz 1951).
3.18. Analysis.
Comparison 3 Sensitivity analysis, Outcome 18 Development of otitis media (without Hogarth 1939).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Anderson 1939.
| Methods | Alternate participants were allocated to control or treatment groups | |
| Participants | 125 children with measles admitted to a hospital in Glasgow. 86% were under 6 years. Control group: 62 + 1 (withdrawn ‐ measles not confirmed). Intervention group: 63. However, 13 participants in the control group and 16 participants in the intervention group already had pneumonia or empyema at the time of enrolment, therefore participants available for analysis of primary outcome (pneumonia) in the 2 groups were 49 and 47 patients respectively
On admission participants were:
‐ given diphtheria antitoxin 4000 units
‐ assessed for complications Appearance of rash was considered first day of illness Evaluation done by 1 person Evenly balanced by age, sex and duration of illness before admission |
|
| Interventions | The treatment group was given sulphanilamide 0.25 g to those under 5 and 0.5 g to those over 5 Children under 5 years were given 0.25 g 4‐hourly for 10 days, followed by 0.25 g 3 times a day until discharge Children over 5 years were given 0.5 g hourly for 10 days, followed by 0.25 g 3 times a day until discharge All participants received the same nursing and general care |
|
| Outcomes | The duration in days of primary pyrexia The duration in days until clinical cure of complications noted on admission The incidence and nature of complications arising in hospital The duration in days of clinical complications arising in hospital The duration in days of residence in hospital. There were more complications in the sulphanilamide group | |
| Notes | 1 control withdrawn (measles not confirmed) Conclusion: sulphanilamide decreases duration of bronchopneumonia, but has no effect on other complications | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Alternate participants were allocated to 2 groups |
| Allocation concealment (selection bias) | High risk | Alternate participants received study drug with supportive care or only supportive care |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Details of all the participants not mentioned in the text |
| Selective reporting (reporting bias) | Unclear risk | Not clear from paper |
| Other bias | Unclear risk | No details about supporting agency |
Garly 2006.
| Methods | Randomised, double‐blind, placebo‐controlled trial | |
| Participants | 84 children (age range 0.49 to 24.8 years) with measles. Separate data for children below 18 years (81 children) were obtained from trial authors | |
| Interventions | The treatment group received co‐trimoxazole. Children below 5 years of age and weighing < 18 kg received paediatric cotrimoxazole tablets 3 times a day and those above 5 years or > 18 kg received adult cotrimoxazole tablets twice a day. Control group received a placebo twice a day | |
| Outcomes | Treatment failure due to pneumonia, admission to hospital or both. Other morbidities | |
| Notes | 2 participants in the treatment group and 1 patient in the control group received the wrong dose of the trial drug. A total of 87 participants were enrolled in the study. Follow‐up of 1 and 2 participants, respectively, was not available in the treatment and control groups and these participants were not included in the intention‐to‐treat analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not clear from paper |
| Allocation concealment (selection bias) | Low risk | Double‐blind RCT |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind randomized controlled trial |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind randomized controlled trial |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All data shown |
| Selective reporting (reporting bias) | Low risk | None |
| Other bias | Low risk | None |
Gibel 1942.
| Methods | Participants were divided into 2 groups on admission | |
| Participants | 401 children with measles admitted to King's Avenue Hospital, New York from December 1940 to June 1941. Separate data for those who already had pneumonia were not mentioned in the paper. However, data on uncomplicated cases (we presume children without pneumonia) in intervention and control groups at time of enrolment were 82 and 148 respectively. All aged under 6 years Control group: 201 participants Treatment group: 153 participants Duration of illness similar at the time of admission | |
| Interventions | The treatment group received sulfathiazole according to body weight Dose 215 mg/kg for the first 24 hours, then 143 mg/kg daily until discharge Controls were treated symptomatically Otherwise the participants received the same nursing care and were admitted to the same ward | |
| Outcomes | Duration in days of primary pyrexia Duration in days until clinical cure of complications noted on admission Incidence and nature of complications arising in hospital Duration in days of clinical complications arising in hospital Duration in days of residence in hospital Death rate of measles complicated by bronchopneumonia as compared to previous years A comparison of the death rate in this hospital in previous years and the death rate this year with sulfathiazole | |
| Notes | One case of bronchopneumonia and 1 case of otitis media were excluded | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned in the text |
| Allocation concealment (selection bias) | High risk | Participants who had pneumonia were not allocated to the no antibiotics group |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label trial |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open‐label trial |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participants who had pneumonia and other complications were allocated to intervention and control groups. Outcome of those who did not have pneumonia at time of enrolment are not very clearly mentioned |
| Selective reporting (reporting bias) | Unclear risk | Details of all the enrolled participants are not very clear |
| Other bias | Unclear risk | No mention of supporting agency |
Hogarth 1939.
| Methods | Alternate participants were assigned to treatment and control groups | |
| Participants | 329 children admitted to a hospital with measles from December 1937 to July 1938 74% were under 4 years of age. No withdrawals 158 received proseptasine Cases were graded into mild, moderate and severe on admission The participants were stratified in the 2 groups by degree of severity (toxemia, intensity of rash, condition of the mouth) Prophylactic dose of diphtheria antitoxin given at the time of admission The control group had more younger children These differences were considered slight and did not preclude comparison All participants assessed by 1 person at the time of admission | |
| Interventions | The treatment group received para‐benzylaminobenzenesulphonamide (proseptasine) for a period of 10 days after admission to hospital:
< 1 year, 0.5 g 3 times a day for 5 days, then 0.5 g twice a day for 5 days
1 to 5 years, 1 g 3 times a day for 5 days, then 0.5 g 3 times a day for 5 days
> 5 years, 1 g 4 times a day for 5 days, then 0.5 g 4 times a day for 5 days Duration of treatment 10 days Controls received no antibiotic or placebo but got the same nursing care |
|
| Outcomes | Complications observed for 12 days after admission Bronchopneumonia ‐ clinical or X‐ray Acute otitis media Cervical adenitis Enteritis Other complications (tonsillitis, conjunctivitis, boils, styes) |
|
| Notes | Conclusion: proseptasine is of value in reducing the incidence of complications such as bronchopneumonia, acute otitis media and cervical adenitis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Alternate participants received intervention or no treatment |
| Allocation concealment (selection bias) | High risk | Alternate participants were assigned to intervention and control group |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label trial |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open‐label trial |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Details of all the enrolled participants available |
| Selective reporting (reporting bias) | Unclear risk | Not clear from data |
| Other bias | Unclear risk | No mention of financial support |
Karelitz 1951.
| Methods | First 15 participants were given chlortetracycline, then subsequent participants were treated with chlortetracycline or penicillin or remained untreated | |
| Participants | Children all aged under 9 years admitted from 15 February to 15 May 1950 to the Willard Parker Hospital, New York Chlortetracycline: 45 participants Penicillin: 44 participants No therapy: 43 Onset of illness: appearance of rash All seen by trial author soon after admission Seen daily for severity and complications Chest X‐ray done in 35 cases assigned penicillin or chlortetracycline groups | |
| Interventions | Chlortetracycline, procaine penicillin First 15 cases were treated with chlortetracycline, later alternate cases were given chlortetracycline or penicillin or left untreated Dose: chlortetracycline: oral 60 mg/kg 4 times a day Penicillin: IM 300,000 units 3/4 of the chlortetracycline treated participants started therapy in the pre‐eruptive period or at the beginning of the rash 3/5 of the penicillin treated participants were given their first dose of penicillin at the beginning of the rash |
|
| Outcomes | Duration and intensity of the rash, temperature, rhinorrhea, photophobia, cough and complications
Pneumonia
Death None of the participants developed complications in the chlortetracycline group, 1 in the penicillin group and 10 in the untreated group |
|
| Notes | Conclusion: very few of the untreated control cases were observed by the trial authors. Information was obtained from hospital records. There were problems with ascertaining duration of cough, photophobia and rhinorrhea The main difference was in the complications that developed in the untreated group and the prolonged course in these cases Children receiving chlortetracycline or penicillin had reduced fever duration Neither chlortetracycline nor penicillin given to children with pre‐eruptive rubeola or begun on the first day of rash seem to have had any definite therapeutic effect on the course of the primary disease Temperature from appearance of rash lasted 2.2, 2.8 and 4.4 days in the chlortetracycline, penicillin and control groups, respectively An earlier drop in temperature in the treated cases was statistically significant Chlortetracycline and penicillin were effective against otitis media and pneumonia present on admission, and for the complications which developed during the course of the disease Chlortetracycline and penicillin are useful in the prevention and cure of secondary infection in measles | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | First 15 participants were given chlortetracycline, then subsequent participants were treated with chlortetracycline or penicillin or remained untreated |
| Allocation concealment (selection bias) | Unclear risk | No details about allocation concealment mentioned in the paper |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open‐label |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not clear from data |
| Selective reporting (reporting bias) | Unclear risk | Not clear from data |
| Other bias | Unclear risk | Not clear from paper |
Karelitz 1954.
| Methods | Consecutive inpatients; children with complications were alternated into the 2 penicillin groups while children without complications were left untreated | |
| Participants | Children with measles admitted to William Parker Hospital, New York
98% aged < 10 years Benzethacil: 61 participants Procaine penicillin: 67 participants No treatment : 41 participants Additional 87 participants were observed in April and May 1953 Ages of the 2 groups were well‐balanced |
|
| Interventions | Aqueous benzethacil 600,000 units single injection in children under 5 years Aqueous procaine penicillin 300,000 units on admission and daily for a total of 4 doses Aqueous procaine penicillin 600,000 units on admission and repeated on the third and sixth days | |
| Outcomes | Pneumonia ‐ diagnosed clinically and also confirmed by X‐ray Discharged within 2 to 3 days. Could not observe late complications |
|
| Notes | Fever in treatment groups was of a shorter duration No complications observed in the group receiving 4 doses of aqueous penicillin 2 children developed bacterial complications in the benzathine penicillin group | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Not used |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open‐label |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not clear from paper |
| Selective reporting (reporting bias) | Unclear risk | Not clear from paper |
| Other bias | Unclear risk | Unclear |
Prasad 1967.
| Methods | Participants were given placebo or tetracycline. Patient allocation not clear | |
| Participants | Inpatients and outpatients at SN Medical College, Agra, India
90% < 5 years
27 cases > 5 years of age 158 children were randomized: ‐ 78 to tetracycline ‐ 80 to placebo |
|
| Interventions | Tetracycline 33 mg/kg for 7 days or placebo | |
| Outcomes | Complications
Clinical improvement, i.e. temperature, cough and general condition 216 cases had an X‐ray examination. 16 were Mantoux‐positive and showed radiological changes ‐ hilar gland enlargement, infiltration, increased lung marking. These participants were excluded from the study |
|
| Notes | Radiological changes were 50% less with tetracycline and serious complications like bronchopneumonia and lobar type were completely absent Use of tetracycline reduces the incidence of serious complications like consolidation and lung collapse and perhaps subsequent sequelae like bronchiectasis and pulmonary fibrosis 81 cases were followed for 6 to 7 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not mentioned |
| Allocation concealment (selection bias) | Unclear risk | Double‐blind randomized trial |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind randomized trial |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | All enrolled participants accounted for |
| Selective reporting (reporting bias) | Unclear risk | All enrolled participants accounted for |
| Other bias | Unclear risk | Funding not mentioned |
IM: intramuscular RCT: randomized controlled trial
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Samb 1995 | Cohort study comparing the development of respiratory symptoms and case‐fatality rates with historical controls. Not a controlled trial |
| Thompson 1938 | Children hospitalised with severe measles treated with sulphonamide or benzyl sulphonamide were compared to children with a milder form of measles (who did not receive antibiotics) for development of bronchopneumonia, otitis media, laryngitis, rhinitis and skin infections. Not a controlled trial |
| Weinstein 1955 | Children with measles without obvious secondary infections. Compared children who received antibiotics prescribed by their primary care physicians and those who did not receive antibiotics for development of pneumonia, otitis media, laryngitis and laryngotracheobronchitis. Not a controlled trial |
Differences between protocol and review
No differences.
Contributions of authors
This review was updated by SK Kabra and R Lodha. SK Kabra (SKK) and R Lodha (RL) conducted the literature searches and reviewed and compiled data from the studies included in the update of this review. SKK and RL wrote the review update.
Sources of support
Internal sources
All India Institute of Medical Sciences, New Delhi, India.
External sources
No sources of support supplied
Declarations of interest
None of the review authors have any conflicts of interest to declare in this review.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Anderson 1939 {published data only}
- Anderson T. Sulphanilamide in the treatment of measles. British Medical Journal 1939;i:716‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Garly 2006 {published data only}
- Garly M, Balé C, Martins LC, Whittle HC, Nielsen J, Lisse IM, et al. Prophylactic antibiotics to prevent pneumonia and other complications after measles: community based randomised double blind placebo controlled trial in Guinea‐Bissau. BMJ 2006;333(7581):1245. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gibel 1942 {published data only}
- Gibel H, Litvak AM. Sulfathiazole in the treatment of measles and its complications. Journal of Pediatrics 1942;21:315‐20. [Google Scholar]
Hogarth 1939 {published data only}
- Hogarth JC. Para‐benzylaminobenzenesulphonamide in the prevention of measles complications. British Medical Journal 1939;i:718‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Karelitz 1951 {published data only}
- Karelitz S, King H, Curtis B, Wechsel M. Use of aureomycin and penicillin in the treatment of rubeola in the pre‐eruptive and early eruptive phase. Pediatrics 1951;7:193‐9. [PubMed] [Google Scholar]
Karelitz 1954 {published data only}
- Karelitz S, Chang C, Matthews ZE. The prophylaxis and treatment of bacterial complications of measles with benzethacil and aqueous procaine penicillin G. Journal of Pediatrics 1954;44:357‐63. [DOI] [PubMed] [Google Scholar]
Prasad 1967 {published data only}
- Prasad R, Mathur GP, Trehan OP, Mehrotra ML, Dayal RS. A clinical and radiological study of measles. Indian Pediatrics 1967;4:243‐50. [PubMed] [Google Scholar]
References to studies excluded from this review
Samb 1995 {published data only}
- Samb B, Simondon F, Aaby P, Whittle H, Seck AM. Prophylactic use of antibiotics and reduced case fatality in measles infection. Pediatric Infectious Disease Journal 1995;14:695‐6. [DOI] [PubMed] [Google Scholar]
Thompson 1938 {published data only}
- Thompson AR, Greenfield CRM. Chemotherapy in measles and whooping‐cough: prophylaxis and treatment of complications. Lancet 1938;2:991‐4. [Google Scholar]
Weinstein 1955 {published data only}
- Weinstein L. Failure of chemotherapy to prevent the bacterial complications of measles. New England Journal of Medicine 1955;253:679‐82. [DOI] [PubMed] [Google Scholar]
Additional references
Aaby 1984
- Aaby P, Bukh J, Lisse IM, Smits AJ. Overcrowding and intensive exposure as determinants of measles mortality. American Journal of Epidemiology 1984;120:49‐63. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Anonymous 2002
- Anonymous. Global measles mortality reduction and regional elimination, 2000‐2001: part I. Weekly Epidemiologic Records 2002;77:50‐5. [Google Scholar]
Anonymous 2006
- Anonymous. Progress in reducing global measles deaths: 1999‐2004. Weekly Epidemiologic Records 2006;10:90‐4. [Google Scholar]
Anonymous 2013
- Anonymous. Progress in global control and regional elimination of measles, 2000–2011. Weekly Epidemiology Records 2013;88:29‐36. [Google Scholar]
Antona 2013
- Antona D, Lévy‐Bruhl D, Baudon C, Freymuth F, Lamy M, Maine C, et al. Measles elimination efforts and 2008‐2011 outbreak, France. Emerging Infectious Diseases 2013;19:357‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bandyopadhyay 2013
- Bandyopadhyay AS, Bandy U. Emerging global epidemiology of measles and public health response to confirmed case in Rhode island. Rhode Island Medical Journal 2013;96:41‐4. [PubMed] [Google Scholar]
Bhaskaram 1984
- Bhaskaram P, Reddy V, Raj S, Bhatnagar RC. Effect of measles on the nutritional status of preschool children. Journal of Tropical Medicine and Hygiene 1984;87:21‐5. [PubMed] [Google Scholar]
Burström 1999
- Burström B, Diderichsen F, Smedman L. Child mortality in Stockholm during 1885‐1910: the impact of household size and number of children in the family on the risk of death from measles. American Journal of Epidemiology 1999;149:1134‐41. [DOI] [PubMed] [Google Scholar]
Cairns 2010
- Cairns KL, Nandy R, Grais RF. Challenges in measuring measles case fatality ratios in settings without vital registration. Emerging Themes in Epidemiology 2010;7(1):4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Caulfield 2004
- Caulfield LE, Onis M, Blössner M, Black RE. Undernutrition as an underlying cause of child deaths associated with diarrhea, pneumonia, malaria, and measles. American Journal of Clinical Nutrition 2004;80:193‐8. [DOI] [PubMed] [Google Scholar]
Corbin 2013
Curtale 2010
- Curtale F, Perrelli F, Mantovani J, Ciofi degli Atti M, Filia A, Nicoletti L, et al. Description of two measles outbreaks in the Lazio Region, Italy (2006‐2007). Importance of pockets of low vaccine coverage in sustaining the infection. BMC Infectious Diseases 2010;10:62. [DOI] [PMC free article] [PubMed] [Google Scholar]
De Serres 2013
- Serres G, Markowski F, Toth E, Landry M, Auger D, Mercier M, et al. Largest measles epidemic in North America in a decade‐‐Quebec, Canada, 2011: contribution of susceptibility, serendipity, and superspreading events. Journal of Infectious Disease 2013;207:990‐8. [DOI] [PubMed] [Google Scholar]
Deivanayagam 1994
- Deivanayagam N, Mala N, Ahamed SS, Shankar VJ. Measles associated diarrhea and pneumonia in south India. Indian Pediatrics 1994;31:35‐40. [PubMed] [Google Scholar]
Delaporte 2013
- Delaporte E, Wyler Lazarevic CA, Iten A, Sudre P. Large measles outbreak in Geneva, Switzerland, January to August 2011: descriptive epidemiology and demonstration of quarantine effectiveness. Euro Surveillance 2013;18(6):20395. [PubMed] [Google Scholar]
Dickersin 1994
- Dickersin K, Scherer R, Lefebvre C. Identifying relevant studies for systematic reviews. BMJ 1994;309:1286‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dover 1975
- Dover AS, Escobar JA, Duenas AL, Leal EC. Pneumonia associated with measles. JAMA 1975;234(6):612‐4. [PubMed] [Google Scholar]
Ellison 1931
- Ellison JB. Pneumonia in measles. Archives of Disease in Childhood 1931;6:37‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gadomski 1993
- Gadomski AM. Potential interventions for preventing pneumonia among young children: lack of effect of antibiotic treatment for upper respiratory infections. Pediatric Infectious Disease Journal 1993;12:115‐20. [DOI] [PubMed] [Google Scholar]
Ghebrehewet 2013
- Ghebrehewet S, Hayhurst G, Keenan A, Moore H. Outbreak of measles in Central and Eastern Cheshire, UK, October 2008‐February 2009. Epidemiology and Infection 2012;9:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gremillion 1981
- Gremillion DH, Crawford GE. Measles pneumonia in young adults. An analysis of 106 cases. American Journal of Medicine 1981;71(4):539‐42. [DOI] [PubMed] [Google Scholar]
Grout 2013
- Grout L, Minetti A, Hurtado N, François G, Fermon F, Chatelain A, et al. Measles in Democratic Republic of Congo: an outbreak description from Katanga, 2010‐‐2011. BMC Infectious Disease 2013;13:232. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Available from www.cochrane‐handbook.org.
Kaschula 1983
- Kaschula RO, Druker J, Kipps A. Late morphologic consequences of measles: a lethal and debilitating lung disease among the poor. Reviews of Infectious Diseases 1983;5(3):395‐404. [DOI] [PubMed] [Google Scholar]
Kouadio 2010
- Kouadio IK, Kamigaki T, Oshitani H. Measles outbreaks in displaced populations: a review of transmission, morbidity and mortality associated factors. BMC International Health Human Rights 2010;10:5. [DOI] [PMC free article] [PubMed] [Google Scholar]
le Roux 2012
- Roux DM, Roux SM, Nuttall JJ, Eley BS. South African measles outbreak 2009 ‐ 2010 as experienced by a paediatric hospital. South African Medical Journal 2012;102(9):760‐4. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Available from www.cochrane‐handbook.org. Chichester: Wiley‐Blackwell, 2011. [Google Scholar]
Mishra 2009
- Mishra A, Mishra S, Lahariya C, Jain P, Bhadoriya RS, Shrivastav D, et al. Practical observations from an epidemiological investigation of a measles outbreak in a district of India. Indian Journal of Community Medicine 2009;34(2):117‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mishra 2012
- Mishra PP, Chauhan NT. Double outbreak of measles in the talaja block of bhavnagar district, gujarat, India 2011: a need for improving the vaccine coverage and the community participation. Journal of Clinical and Diagnostic Research 2012;6:1713‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Morton 1986
- Morton R, Mee J. Measles pneumonia: lung puncture findings in 56 cases related to chest X‐ray changes and clinical features. Annals of Tropical Paediatrics 1986;6:41‐5. [DOI] [PubMed] [Google Scholar]
Muscat 2009
- Muscat M, Bang H, Wohlfahrt J, Glismann S, Mølbak K, EUVAC.NET Group. Measles in Europe: an epidemiological assessment. Lancet 2009;373:383‐9. [DOI] [PubMed] [Google Scholar]
Nmor 2011
- Nmor JC, Thanh HT, Goto K. Recurring measles epidemic in Vietnam 2005‐2009: implication for strengthened control strategies. International Journal of Biological Sciences 2011;7(2):138‐46. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ntshoe 2013
- Ntshoe GM, McAnerney JM, Archer BN, Smit SB, Harris BN, Tempia S, et al. Measles outbreak in South Africa: epidemiology of laboratory‐confirmed measles cases and assessment of intervention, 2009‐2011. PLoS One 2013;8(2):e55682. [DOI] [PMC free article] [PubMed] [Google Scholar]
Olson 1975
- Olson RW, Hodges GR. Measles pneumonia. Bacterial suprainfection as a complicating factor. JAMA 1975;232(4):363‐5. [DOI] [PubMed] [Google Scholar]
Perry 2004
- Perry RT, Halsey NA. The clinical significance of measles: a review. Journal of Infectious Diseases 2004;89(Suppl):4‐16. [DOI] [PubMed] [Google Scholar]
Pezzotti 2013
- Pezzotti P, Valle S, Perrelli F, Guerra MP, Pozzato S, Chini F, et al. Measles outbreak in the Lazio region of Italy: surveillance and impact on Emergency Departments and hospitalizations. Annali di Lgiene 2013;25:299‐309. [DOI] [PubMed] [Google Scholar]
Reddy 1986
- Reddy V, Bhaskaram P, Raghuramulu N, Milton RC, Rao V, Madhusudan J, et al. Relation between measles, malnutrition and blindness; a prospective study in Indian children. American Journal of Clinical Nutrition 1986;44:925‐30. [DOI] [PubMed] [Google Scholar]
RevMan 2012 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Tricou 2013
- Tricou V, Pagonendji M, Manengu C, Mutombo J, Mabo RO, Gouandjika‐Vasilache I. Measles outbreak in Northern Central African Republic 3 years after the last national immunization campaign. BMC Infectious Disease 2013;13:103. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wesley 1971
- Wesley AG, Sutton JB, Widrich AJ. The aetiology of pneumonia associated with measles in Bantu children. South African Medical Journal 1971;45(48):1402‐4. [PubMed] [Google Scholar]
WHO 1995
- World Health Organization. Clinical research on treatment of measles: report of a meeting (WHO/CDR/95.15). Geneva: WHO, 1995. [Google Scholar]
Wolfson 2009
- Wolfson LJ, Grais RF, Luquero FJ, Birmingham ME, Strebel PM. Estimates of measles case fatality ratios: a comprehensive review of community‐based studies. International Journal of Epidemiology 2009;38:192‐205. [DOI] [PubMed] [Google Scholar]
Yang 2011
- Yang HM, Mao M, Wan C. Vitamin A for treating measles in children. Cochrane Database of Systematic Reviews 2011, Issue 7. [DOI: 10.1002/14651858.CD001479.pub3] [DOI] [Google Scholar]
References to other published versions of this review
Kabra 2008
- Kabra SK, Lodha R, Hilton DJ. Antibiotics for preventing complications in children with measles. Cochrane Database of Systematic Reviews 2008, Issue 3. [DOI: 10.1002/14651858.CD001477.pub3] [DOI] [PubMed] [Google Scholar]
Kabra 2011
- Kabra SK, Lodha R, Hilton DJ. Antibiotics for preventing complications in children with measles. Cochrane Database of Systematic Reviews 2011, Issue 9. [DOI: 10.1002/14651858.CD001477.pub3] [DOI] [PubMed] [Google Scholar]
Shann 1997
- Shann F. Meta‐analysis of trials of prophylactic antibiotics for children with measles: inadequate evidence. BMJ 1997;314:334‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shann 1999
- Shann F, D'Souza RM, D'Souza R. Antibiotics for preventing pneumonia in children with measles. Cochrane Database of Systematic Reviews 1999, Issue 2. [DOI: 10.1002/14651858.CD001477.pub2] [DOI] [PubMed] [Google Scholar]
Shann 2000
- Antibiotics for preventing pneumonia in children with measles. Shann F, D'Souza RM, D'Souza R. Cochrane Database of Systematic Reviews 2000, Issue 3. [DOI: 10.1002/14651858.CD001477.pub2] [DOI] [PubMed] [Google Scholar]