
Figure 2.
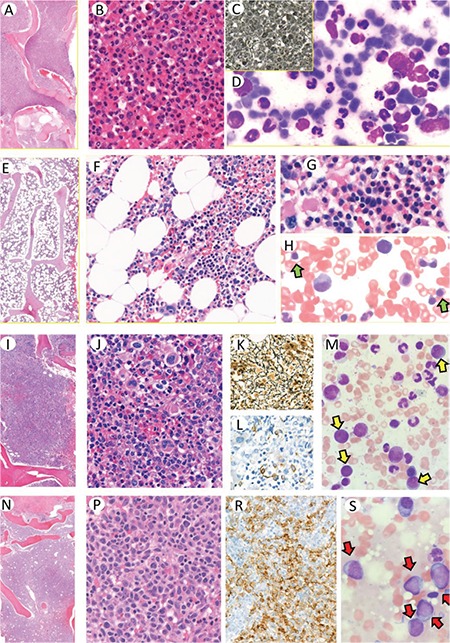
Bone marrow biopsy in chronic phase (CP) CML is usually hypercellular with 100% cellularity (A). The bone marrow cells are almost all composed of mature granulocytes and their precursors (B). Reticulin could be seen, especially in the cases with increased megakaryocytes, but usually does not increase (C). Bone marrow aspirate is hypercellular, composed of maturing granulocytic precursors with striking decrease in other precursors (D). Cellularity decreases in the bone marrow of responders to TKI treatment (E, F). The islands of erythroid precursors and megakaryocytes as well as the granulocytic series reflect the normal composition (G). Aspirate smears can also reflect the normal cellular composition with erythroid precursors (H; green arrows). Accelerated phase (AP) CML is characterized by increased blasts of <10%-19% and/or megakaryocytes (I, J). Increase in megakaryocyte population promotes reticulin fibrosis (K). Immunohistochemistry is helpful, especially for demonstrating blasts by CD34 staining (L). Blasts on bone marrow aspirates are scattered between myeloid precursors (M; yellow arrows). The blasts are the dominant cellular component in the bone marrow of blastic phase (BP) CML (N, P). Presence of strikingly increased blasts could be demonstrated by CD34 immunohistochemistry (R). On bone marrow aspirate smears, blastic cells are also dominant (S; red arrows).