
Figure 2: Cardiovascular risk factors drive reticulated thrombopoiesis and accelerate atherosclerosis via enhanced megakaryopoiesis.
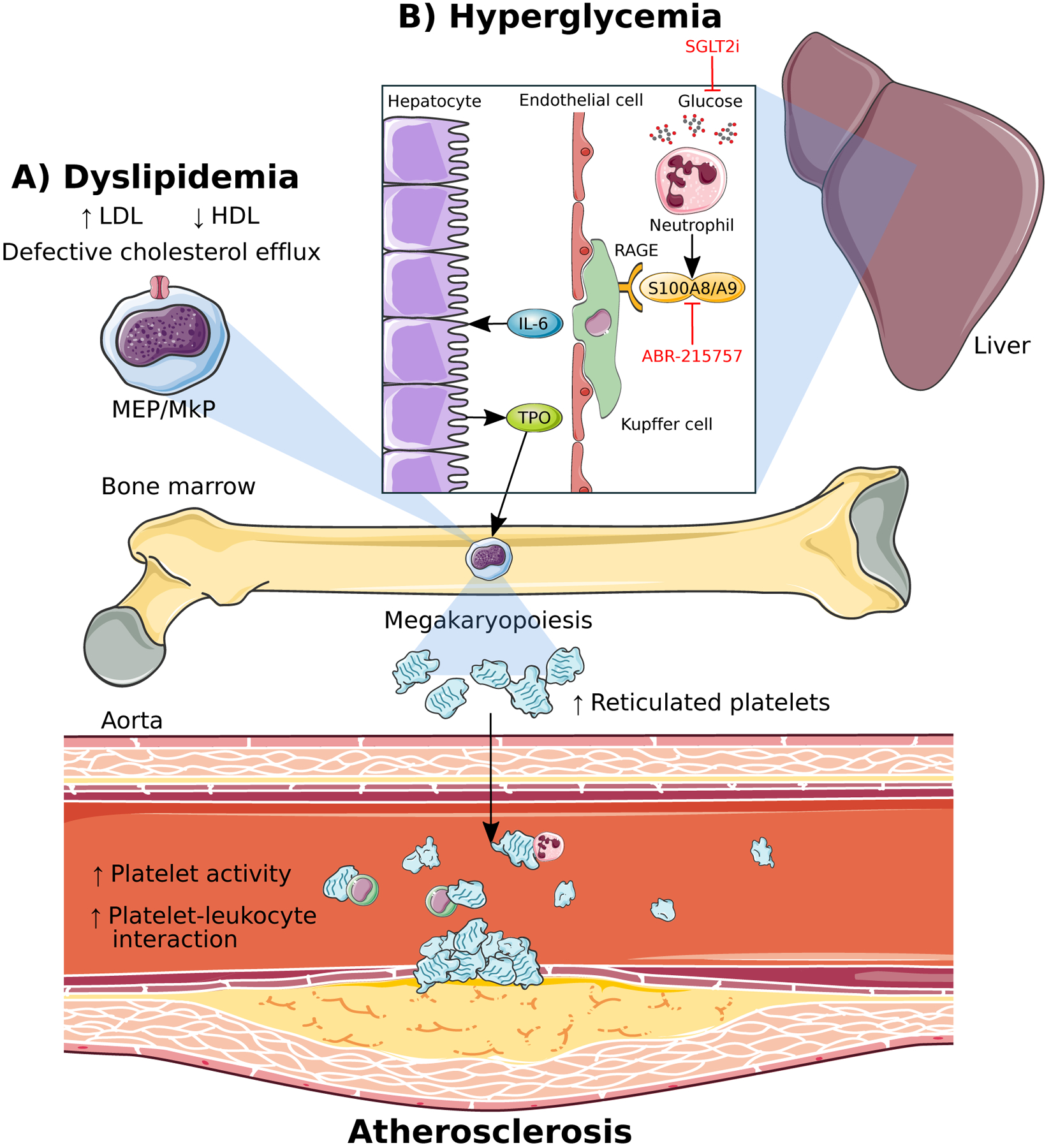
A) Dyslipidemia in the form of form of increased low-density lipoproteins (LDL) and decreased high-density lipoproteins (HDL) along with defective cholesterol efflux promotes proliferation and differentiation of megakaryocyte-erythroid progenitors (MEPs) and megakaryocyte progenitors (MkPs). B) Hyperglycemia-induced S100A8/A9 from neutrophils stimulates megakaryopoiesis and promotes atherosclerosis via enhanced liver inflammation. Binding of S100A8/A9 to the receptor for advanced glycation end-products (RAGE) on Kuppfer cells in the liver stimulates IL-6 production leading to TPO production from hepatocytes which travels to the bone marrow to promote megakaryopoiesis. Reticulated thrombocytosis resulting from enhanced megakaryopoiesis in both dyslipidemia and hyperglycemia leads to increased platelet activity, platelet-leukocyte interactions and accelerated atherosclerosis. Lowering blood glucose using the sodium-glucose cotransporter 2 inhibitor (SGLT2i), dapagliflozin, as well as blocking S100A8/A9 binding to RAGE, prevents hyperglycemia-induced thrombocytosis and atherosclerosis.