

Abstract
Background
Today’s foot and ankle surgeon has an enhanced understanding of forefoot pathology and treatment options compared to surgeons who practiced in previous decades. This paper summarizes developments in forefoot surgery in the past 40 years, specifically in treatments for mallet toe, hammertoe, neuroma, and metatarsophalangeal joint instability.
Materials and Methods
A review of the literature was conducted using the PubMed search engine, with key terms including, “mallet toe,” “hammertoe,” “neuroma,” “metatarsophalangeal joint instability,” “plantar plate,” and “forefoot surgery.” Chapters in major orthopaedic textbooks covering these topics were also reviewed. We then chronicled the history of the diagnosis and treatment of these pathologies, with a focus on the past 40 years.
Conclusions
There have been major advances in understanding and treating forefoot pathologies in the past four decades; however, there remain areas for improvement both in the diagnosis and treatment of these problems.
Level of Evidence
Level V, meta-synthesis.
Keywords: Mallet toes, Hammertoes, Morton’s neuroma, Metatarsophalangeal joint instability, Forefoot surgery
Introduction
Forefoot pathology affects many individuals and can be debilitating, severely impairing one’s ability to participate in vocational and avocational activities. Today, the orthopedic surgeon has libraries of tools and techniques with which to treat forefoot conditions. However, not so long ago, our understanding of, and ability to treat pathologies of the forefoot were limited. The purpose of this paper is to offer a succinct summary of knowledge and surgical treatments of common forefoot disorders as they have evolved over the last 4 decades—the span of the senior author’s career. The intention is to provide the beginning of foot and ankle surgery with an understanding of history so as to continue to build the future of forefoot surgery.
At the time that the senior author began his career as an orthopedic surgeon in 1978, there were only three orthopedic foot and ankle fellowships in the United States, and the definitive textbook for foot surgery was DuVries’ Surgery of the Foot, a fourth edition text with 625 pages [1]. The last 35-page chapter was on surgical treatment of the forefoot, though the majority of the chapter focused on hallux valgus and hallux rigidus, while the remaining outlined a few treatments for hammertoes. The sparse treatment of the topic reflects the state of knowledge at the time. In fact, we now know there are multiple causes of forefoot pain and dysfunction, the correct diagnosis and proper treatment of which are crucial to patient improvement. This paper will address four common conditions: (1) mallet toe, (2) hammertoe, (3) neuroma, and (4) lesser metatarsophalangeal joint instability.
Mallet Toe
The term, mallet toe, first appeared in the orthopaedic literature in a book chapter by Lake in 1939. In 1973, the DuVries textbook had two pages on the topic, in which “hammertoe” and “mallet toe” were both described as “essentially acquired partial or complete dislocations of the proximal interphalangeal joints”, and when the distal interphalangeal joint was involved, the deformity was referred to specifically as a “mallet toe” (Fig. 1) [1]. Unfortunately, over the years, the definitions of toe deformities have been confusing. Today, a simplified nomenclature has been adopted, as described in the most recent edition of Mann’s Surgery of the Foot and Ankle: “A mallet toe involves the distal interphalangeal (DIP) joint [such that] the distal phalanx is flexed on the middle phalanx” [2].
Fig. 1.

Mallet toe deformity demonstrates flexion deformity at the distal interphalangeal joint
The etiology of mallet toe is varied, and has been attributed to anatomy and toe length, shoewear, trauma, or a factor in systemic neurologic disease. With a fixed mallet toe deformity, patients often complain of pain at the dorsal DIP joint, and/or pain at the tip of the affected toe, where undue pressure from footwear and weight bearing is experienced. Calluses may be found at either of these locations. When symptoms can no longer be tolerated with treatments such as modified shoewear and padding in a patient without underlying systemic disease, surgical intervention may be indicated.
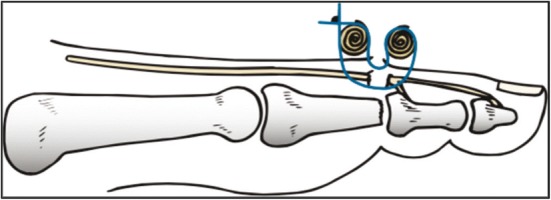
In the 1970s, surgical treatment involved soft-tissue releases, tenotomies, tendon transfers, joint resection, and arthrodesis [1]. In the DuVries text, joint reduction was achieved by resecting the middle phalangeal head to allow relocation of the distal phalanx. Fixation was often attempted with sutures and bolsters, placed dorsal to the DIP joint, outside of the skin (Fig. 2). Despite the described techniques of the time, there were no reports on the long-term outcomes of surgical treatment of mallet toe deformity until 1995, when the senior author published a report of 50 patients followed over a 55-month follow-up. The described technique involved resection of the joint, including preparation of both the middle and distal phalangeal joint surfaces, and fixation with a Kirschner wire (k-wire) that traversed the DIP joint and was removed after 3 weeks. Wire fixation of the joint offered a simpler and more reliable technique than bolster fixation (Fig. 3).
Fig. 2.
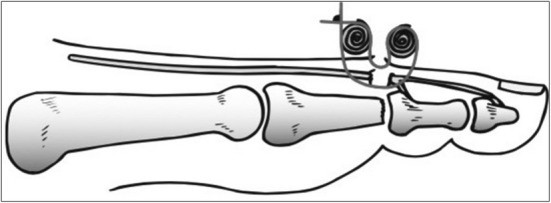
Early mallet toe repair using Telfa© bolster for fixation
Fig. 3.

Mallet toe repair using k-wire fixation
While 86% of patients were satisfied with the results of their surgery, fusion was not achieved in all toes such that fibrous union of the DIP joint was reported in 28% of treated toes. This has led to the question of how to achieve compression for reliable fusion at the DIP joint, which is small and difficult to treat. While there have been many published reports of intramedullary fixation of the proximal interphalangeal joint in feet (see section on hammertoes), very little has been published on fixation of the distal interphalangeal joint. Khan et al. described outcomes of the Smart Toe© implant, an intramedullary nitinol implant, in small joints of the foot. Only 13.4% of the joints examined (11 of 82) were distal interphalangeal joints, and while the authors reported an average 71% in subjective improvement by patients, they did not report on the fusion rates associated with the implant, let alone specific fusion rates at the distal versus proximal interphalangeal joints. Jones et al. described using the Barouk screw, a screw with distal and proximal threads that when used in a retrograde manner, captures the middle and distal phalanges in a mallet toe correction. Of five toes in five patients, all achieved fusion, and all but one patient was satisfied with the procedure. One patient was “satisfied with reservations”, and had a history of multiple preexisting ipsilateral foot problems that precluded normal shoewear [3]. Recently, the senior author of this paper has been using headless compression screws, inserted at the tip of the distal phalanx and traversing the distal interphalangeal joint; however, results of this method have not been published. This remains an area that will see continued improvement in available techniques and implants.
Hammertoe
The current accepted definition of a hammertoe is a deformity in which the middle and distal phalanges are flexed on the proximal phalanx. A simple hammertoe does not involve the metatarsophalangeal (MTP) joint, whereas a complex hammertoe involves a hyperextension deformity at the MTP joint (Fig. 4) [2]. Related to this is claw toe deformity, which involves a complex hammertoe deformity of all lesser toes, rather than only one toe. As with a mallet toe, a hammertoe deformity can result in painful callosities, difficult shoewear, and painful ambulation. When activity changes, shoewear modifications, and nonsurgical treatment modalities such as toe taping fail, surgical intervention may be indicated.
Fig. 4.
a Simple hammertoe deformity with flexion of the PIP joint; b complex hammertoe deformity with extension of MTP and flexion of the PIP joint
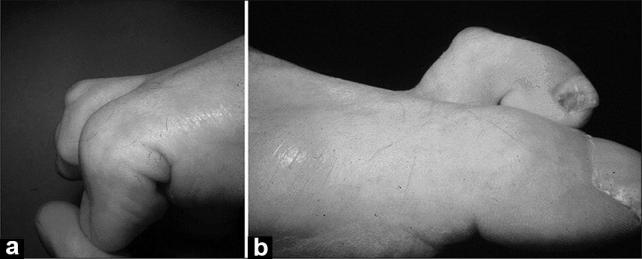
Forty years ago, operative solutions for hammertoe deformity often resulted in instability, malalignment, progressive disfigurement, or recurrent deformity (Fig. 5). Proximal phalangectomy was performed to allow for reduction of the MTP joint; however, such a procedure resulted in contraction of the MTP joint, further dorsally displacing the proximal phalanx and causing recurrent deformity. To prevent this complication, other surgeons began to perform syndactylization following proximal phalangectomy, in an attempt to anchor the affected digit down to its neighboring digit. This too was disfiguring because when the length of the affected digit was not maintained, the toe would shorten while being tethered to its neighbor. With aggressive resection of bone, toes would become excessively unstable and displaced, preventing normal walking or shoewear.
Fig. 5.

a Hammertoe treated with partial proximal phalangectomy; b progressive deformity with passage of time; c clinical photo of patients deformity
As with mallet toe fixation, attempts were made to stabilize the hammertoe deformity at the PIP joint with external bolsters (Fig. 6). In 2000, the senior author published 5-year follow-up for 118 cases of surgical hammertoe correction [4]. Important changes in surgical technique included preparation of both the proximal and middle phalanges, with proximal phalangeal condylectomy at the PIP joint, and resection of the articular surface at the middle phalanx. Additionally, fixation was achieved with retrograde Kirschner wire placement through all three phalanges (Fig. 7). At 5 years, 86% of patients were satisfied, or satisfied with reservations, with the result of their surgery. Of those who were dissatisfied, the majority were unhappy with resultant malalignment, which occurred in 15% of cases (Fig. 8). Another group’s retrospective study of over two thousand hammertoe corrections using k-wire fixation underscored the safety and efficacy of the technique. In their study, Kramer et al. found a low infection rate (0.3%), malalignment in 2.1% of cases, vascular compromise in 0.6% of cases, and a 3.5% reoperation rate [5]. Furthermore, k-wire fixation has independently been shown to be more reliable in preventing recurrence than external bandaging techniques [6].
Fig. 6.
Treatment of hammer toe deformity with Telfa© bolster fixation
Fig. 7.
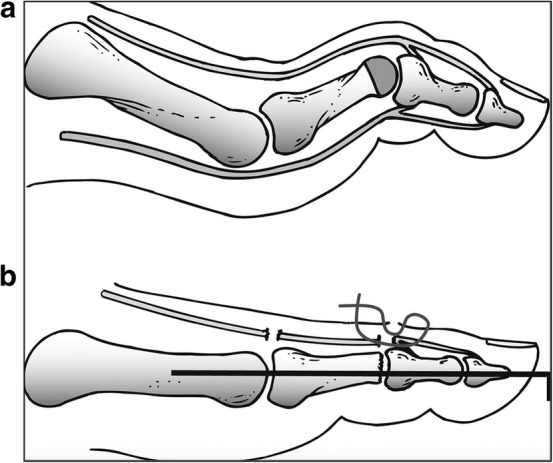
a Preoperative hammer toe deformity; b following hammer toe repair with k-wire fixation
Fig. 8.
a Postoperative hyperextension deformity following hammer toe repair; b lateral drift of toe following hammer toe repair, at risk for pressure deformity
Today, there is an active quest for hammertoe fixation, as evidenced by myriad available commercial implants to address the problem [7]. In the senior author’s paper cited above, k-wire fixation resulted in a fusion rate at the PIP joint of 81%. The results of k-wire fixation have been encouraging in that surgery is helpful in the majority of patients; however, they highlight room for improvement with respect to fusion and malalignment. A second k-wire has been found to address malalignment with success [8]. What have become more heavily developed are intramedullary devices, whose theoretical advantages over k-wire fixation include eliminated pin-site infections from protruding pins, which occurs in about 1.7% of forefoot procedures, and as stated above, in less than 1% of hammertoes fixed with k-wires. Additionally, there is also the possibility that intramedullary devices offer greater compression over k-wire fixation. However, early evidence brings these potential benefits into question. Intramedullary devices that fix the PIP joint but do not violate the DIP joint can be difficult to insert, and once implanted, may offer variable compression, depending on the surgeon’s technique in preparing the joint surfaces and inserting the device, as well as patient factors such as bone quality. A cadaveric study comparing k-wire to intramedullary fixation of hammertoes showed that with cyclic loading, k-wires offered greater, not less, stability and provided for a stiffer construct [9].
In 2015, Guelfi et al. reviewed the available literature on k-wire versus intramedullary fixation of hammertoes and found similar patient satisfaction, radiographic fusion, complication and revision surgery rates [10]. Since then, additional studies comparing specific intramedullary devices with k-wire fixation have been performed, often showing equivalent results. A retrospective, comparative study of two different intramedullary fixation devices (SmartToe, Stryker; and Tenfuse, Wright Medical) and k-wire fixation was reported by Obrador et al. [11]. They found no statistically significant differences in functional outcome and incidence of complications observed among the three fixation groups. Richman et al. compared another type of intramedullary device (Cannulink, Wright Medical) to k-wire fixation in a retrospective study and found greater complications in the k-wire group, but no statistically significant difference in clinical outcomes, including reoperation rates [12]. The senior author of this paper studied the fusion rate using a popular intramedullary device (SmartToe), and found it to be 81%, identical to the fusion rate in his early k-wire study [13, 14]. Other groups, studying the same device report a range of fusion rates, from 63 to 98% [14–16]. And a direct comparative study of this particular intramedullary device and k-wire fixation demonstrated no differences in malunion, nonunion, fracture, or the need for revision surgery [15]. Multiple other groups have reported the results of a variety of intramedullary devices [7, 17–20], generally showing favorable clinical outcomes. So, much remains to be learned about the clinical benefit of intramedullary versus traditional, percutaneous k-wire fixation of hammertoe correction. Furthermore, as there are so many different available products, it is difficult to discern whether one product is superior to others.
In addition to seemingly equivalent clinical outcomes, it is unclear whether there are advantages in operative time and cost of using novel implants over traditional wire fixation. Available data suggest that there are none. Albright et al. performed a cost analysis of traditional percutaneous k-wire fixation versus commercial implants for hammertoe fixation and found that there was a much higher cost associated with the implants compared to wire fixation that did not justify the potential clinical benefit [21]. Surgical time for k-wire fixation versus other types of fixation has not been compared and remains an area for further study.
Interdigital Neuroma
Thomas George Morton described “Morton’s neuralgia” in 1876, and this disease entity has since been referred to as “Morton’s neuroma”, or interdigital neuroma [1]. The literature prior to the 1970s was sparse on the topic. Dieterle and Kuzma presented a case report in 1922 [22], and between that year and 1970, there were only eight papers on the topic, mainly descriptive case reports. The late 1970s and 1980s brought histologic studies that provided understanding of the underlying tissue abnormalities associated with the clinical presentation [23–25].
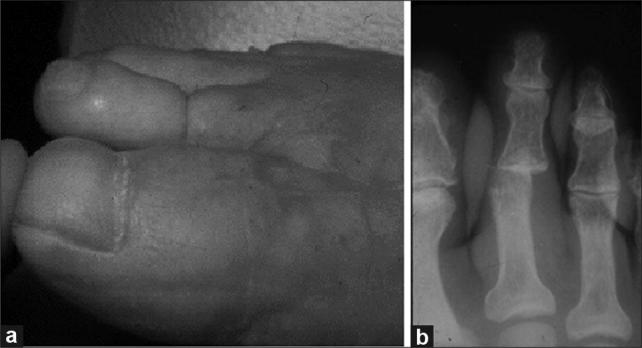
Interdigital neuromas are characterized by forefoot pain that localize to the plantar interdigital spaces and can radiate proximally and distally. The pain is often characterized as sharp, shooting, or burning. Histologically, the common digital nerve, which traverses the interdigital spaces between the metatarsal heads, underneath the transmetatarsal ligament, is often found to have intraneural fibrosis, sclerohyalinosis, excessive elastic fibers in the stroma, and associated changes in the surrounding tissue such as hyperplasia of the muscle layer and proliferation of small vessels (Fig. 9) [2].
Fig. 9.
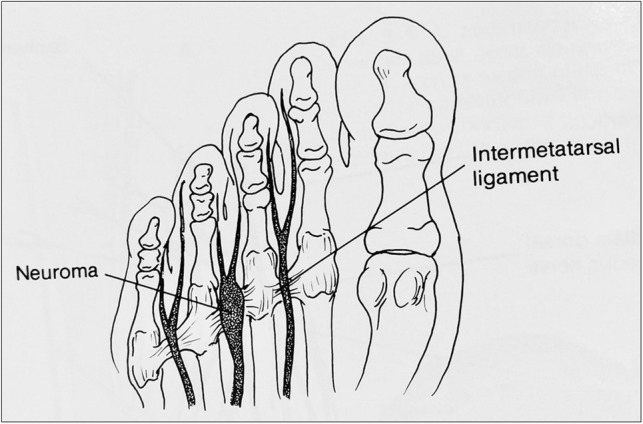
Diagram of interdigital neuroma
Forty years ago, the most common location for an interdigital neuroma was not known, and it was debatable as to what would be the best approach to surgically access the common digital nerve. The DuVries textbook referenced authors who described plantar approaches, as well as those who used dorsal approaches. The text reported that 95% of patients undergoing a dorsal exposure to excise the neuroma were asymptomatic after the procedure [1].
In 1983, Mann and Reynolds published the first report of postoperative results following neuroma excision through a dorsal approach [26]. They studied 76 neuromas in 56 patients and found an equal number of interdigital neuromas in the second and third interspaces. Eighty percent of their patients had subjective improvement of their preoperative pain. This study was followed by Addante et al. in 1986, who reported the outcomes on 136 patients who underwent neuroma excision through a dorsal approach [27]. Two patients had residual pain that was successfully addressed with revision neuroma excision; the authors did not report on patient satisfaction. In 1988, Karges reported the results of a plantar approach to neuroma excision in 57 feet from 51 patients and noted a 93% rate of good to excellent results [28]. The author attributed the high satisfaction rate to a more proximal resection of the nerve than can be achieved through a dorsal approach and felt that the plantar scar did not affect patient satisfaction. It was not until the 1990s that Friscia et al. published the largest study on surgical outcomes for interdigital neuroma [29]. In their study, 366 feet in 313 patients were followed for an average of 5.9 years after undergoing a dorsal approach to neuroma excision. Eighty-eight percent of patients were satisfied with the procedure, and the size of the neuroma inversely correlated with the level of satisfaction following surgery. It was not until a decade later that the next largest follow-up study was reported by the senior author of the current paper [30]. 74 neuromas in 71 feet were followed for an average of 5.8 years following a dorsal approach. Similar to the study before it, 85% of patients reported good to excellent satisfaction. In both of the latter studies, bilateral neuroma excision was generally associated with lower satisfaction.
While the DuVries text noted that the third webspace was the most common location for an interdigital neuroma, this claim was not substantiated by data. Several studies since the 1970s have reported on the incidence of interdigital neuromas in specific webspaces. In the Mann and Reynolds study of 76 neuromas, there were an equal number of neuromas in the second and third webspaces. In the Friscia paper following over 300 feet, 91% of neuromas were found in the third webspace. In the Coughlin study, 78% of neuromas were in the third webspace, and 22% in the second (Fig. 10). Out of 136 patients, the Addante paper reported 66.4% of neuromas in the third webspace, 17.8% in the second, and 3.9% in the first. Levitsky et al. studied the digital nerves of 71 cadaveric feet and found that of those with neuromas, 55.2% were in the third webspace, while 44.8% were in the second [31]. The data over the years support the claim from the DuVries textbook and can help the surgeon have a higher index of suspicion for a neuroma when a patient’s pain is in the third digital webspace. It is, however, important to keep in mind that neuromas in more than one location in the same patient can occur [32].
Fig. 10.
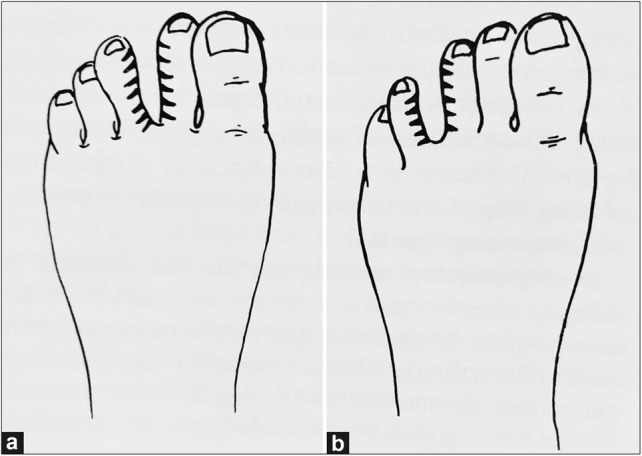
Pattern of numbness with second or third interdigital neuroma
Since the earliest studies on surgical outcomes for interdigital neuromas cited above, a number of additional studies with similar follow-up have confirmed generally good results and satisfaction in over 80% of patients who undergo a dorsal approach neurectomy [33–37]. With respect to a plantar approach, Nery et al. reported an 89% satisfaction rate in 160 patients (227 neuromas) [38]. Of the patients who were less than satisfied, many had complaints related to their surgical scar, a problem that has been documented in other studies [39, 40]. Regardless of the approach, surgical treatment of interdigital neuromas tend to have better outcomes than nonsurgical modalities in the patient with pain that is recalcitrant to conservative measures [41].
Modifications to surgical techniques have been described to supplement, or to supplant neurectomy. For example, endoscopic or open decompression of the nerve by transection of the transmetatarsal ligament, or by metatarsal osteotomy has been described [42–44]. The merit of osteotomy for decompressing the common digital nerve is questionable based on plantar pressure measurements in patients with and without a neuroma. One such study found show no correlation between variables including peak pressure, contact time, and pressure–time integrals under the metatarsal heads, forefoot width, and foot length in symptomatic and control groups. The authors therefore questioned the validity of performing osteotomies to treat neuromas that are not associated with other MPJ pathologies [45]. Simple resection of the transmetatarsal ligament is also questionable given findings in anatomic studies that show interdigital neuromas typically lie distal to the ligament and that transection of the ligament alone does not address the pathologic tissue [46]. To compound this problem, when the transmetatarsal ligament is released endoscopically, there are associated risks of damage to nearby structures [47]. Other authors have described further augmenting neurectomy by burying the proximal stump of nerve into muscle [48–51]. Though with limited outcomes data, this technique appears to be as effective as, and without proven benefits over neurectomy alone.
Alternatives to surgery have been described in the last 20 years; however, outcomes for these treatments have been short term and variable. Alcohol sclerosing therapy, wherein alcohol is injected into the intermetatarsal space either blind or under ultrasound guidance, has been described by some as an effective way to reduce pain associated with interdigital neuromas [52–54]. The type of alcohol used is generally not specified in the literature, though it is often phenol when it is specified and various strengths of alcohol have been described. While the technique shows generally favorable immediate and short-term outcomes, it does not appear to offer long-term pain relief [55–57]. Other agents that have been described to improve symptoms include corticosteroids, hyaluronic acid, and capsaicin [58–60]. However, long-term relief has not been reported with these injectants. Other treatment modalities such as extracorporeal shockwave therapy and radiofrequency ablation have also been described. And like other newer techniques, long-term outcomes, as well as refined techniques, are yet to be described [61–65].
Other development in the last 4 decades revolving around interdigital neuroma have been in the diagnosis of the condition. Most notably, magnetic resonance imaging and ultrasound have been shown to have some confirmatory value once a diagnosis based on history and physical exam has been made [66–72]. One group has reported on the potential of electrodiagnostic studies in making the diagnosis [73]. While an imaging study may help to confirm the diagnosis, the additional cost and time of obtaining such tests, coupled with their variable sensitivity and specificity, make a good history and physical exam the mainstay of identifying the condition. While the value of ultrasound as an imaging modality in diagnosis is not universally accepted, it does have potential in directing injections for either diagnostic or treatment purposes [74, 75]. In the future, as image resolution continues to improve and costs decline, adjunct diagnostic techniques such as MRI and ultrasound may become more widely used.
Lesser Metatarsal-Phalangeal Joint Instability
Lesser metatarsal-phalangeal joint instability can lead to dorsal and medial or lateral deviation of the lesser toes. This can cause pain, changes in gait, and problematic shoewear. Forty years ago, deformities at the lesser MTP joint were poorly understood. Textbook treatment of the topic was mainly descriptive in the context of other pathologies such as hallux valgus, neuromas, trauma, or conditions experienced by dancers [76–78]. The etiology had not yet been studied, though various treatments were described.
In 1987, the term “crossover second toe deformity” was coined by the senior author of this paper [79]. It described a deformity in which the second toe deviates medially, then eventually dorsally and medially over the great toe and was thought to be due to an incompetent lateral collateral ligament and joint capsule at the second MTP joint (Fig. 11). This etiology was extrapolated and applied to deformities at the other lesser MTP joints as well. Described treatments over several decades remained the same. They included soft-tissue release, reefing of the joint capsule in an attempt to reduce and pull the toe into place, extensor digitorum brevis transfer beneath the transmetatarsal ligament to allow for a dynamic plantar pull of the displaced digit, flexor tendon transfer, phalangeal closing wedge osteotomy, metatarsal condylectomy, and distal oblique metatarsal osteotomy. The results of many of these procedures were generally thought to be satisfactory in a majority of patients; however, there were still large numbers of patients who experienced continued deformity and pain [78].
Fig. 11.

Intraoperative photo demonstrating complete rupture of the lateral collateral ligament associated with a crossover second toe deformity
In 2000, Deland and Sung performed a cadaveric study on one specimen from a donor with second crossover toe deformity [80]. They compared the anatomy of the diseased MTP joint to the normal anatomy of the donor’s contralateral foot. They found multiple derangements. These included medial displacement of the flexor tendons and plantar plate, deformity of the plantar plate, contracture of the medial collateral ligament, and rupture of the lateral collateral ligament. Their study was important in defining anatomic changes with crossover toe deformity, but did not identify the causative factor for the deformity.
After studying 16 cadaveric specimens with crossover toe deformity, a team led by the senior author published what ended up being a landmark paper on the cause of lesser toe MTP joint deformity [81, 82]. The team found that disruptions in the thickened plantar capsule at the MTP joint, otherwise known as the plantar plate, were the main cause of dorsal and medial/lateral deviation of the proximal phalanx on the metatarsal head (Fig. 12). Tears in the plantar plate were typically transverse and at the insertion of the plantar plate on the proximal phalanx of the deformed toe. This piece of information was key to developing classification and direct treatment of the clinical problem. Plantar plate tears in this study were graded on a scale of zero to four, according to increasing severity, as indicated in Table 1.
Fig. 12.
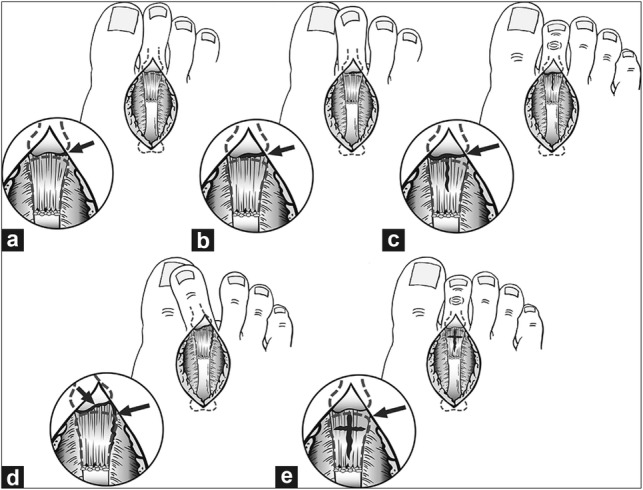
Diagram of grading of crossover toe pathology. Grade zero (not shown) indicates attenuation with or without capsular discoloration of the plantar plate. a Grade one involves a distal transverse partial tear (< 50%); grade one may also indicate medial/lateral/central or intrasubstance lesions that involve less than 50% of the plantar plate substance. b Grade two indicates a more complete (> 50%) distal transverse tear at the insertion, or tears of the medial/lateral/central/intrasubstance areas (> 50%). c, d Grade three involves a transverse and longitudinal plantar plate tear that may involve the collateral ligaments; e Grade four indicates a complete disruption of the plantar plate in a “buttonhole” shape, a combination of transverse and longitudinal tears
Table 1.
Grading of plantar plate tears
| Grade | Description |
|---|---|
| 0 | Plantar plate or capsular attenuation, and/or capsular discoloration |
| 1 | Transverse distal tear (adjacent to insertion into proximal phalanx (< 50%); medial/lateral/or central area) and/or midsubstance tear (< 50%) |
| 2 | Transverse distal tear (≥ 50%); medial/lateral/or central area and/or midsubstance tear (< 50%) |
| 3 | Transverse and/or longitudinal extensive tear (may involve collateral ligaments) |
| 4 | Extensive tear with button hole (dislocation); combination transverse and longitudinal plate tear |
At the time that the cadaveric study was published, there had been less than a handful of reports on direct plantar plate repair techniques through a plantar approach [83–85]. In these studies, postoperative arthrography tended to show intact repairs, and patients tended to be satisfied. However, given the plantar approach, the potential for a painful and problematic scar on the sole of the foot is a deterrent for many foot and ankle surgeons. There was one study that described a dorsal approach and a plantar plate repair, combined with a Weil osteotomy [86]. These authors described a technique in which a dorsal incision was made over the affected interspace, the extensor digitorum brevis tendon was divided, and the extensor digitorum longus was lengthened with a “z” shaped tenotomy. Shortening the metatarsal head through a Weil osteotomy allowed for visualization of the plantar plate. A tear in the plantar plate would be completed and repaired with a suture passed through the tissue, then through drill holes in the proximal phalanx, and tied on the dorsal aspect of the proximal phalanx. The Weil osteotomy would then be fixed with small titanium screws. These authors reported satisfaction in 17 out of 23 patients and a stable MTP joint in the majority of toes.
In 2011, Weil et al. reported on the outcomes of a very similar procedure involving direct repair of the plantar plate after a Weil osteotomy to allow for visualization of the tissue through a dorsal approach [87]. They studied the outcomes in 13 patients and found 85% of patients reported in improved function and 77% were either satisfied or very satisfied with the procedure.
The technique offered by the Gregg and Weil papers was endorsed in the 2012 cadaveric study on plantar plate tears, because it allowed for a dorsal approach as well as direct repair of the causative defect of a dislocated MTP joint. This technique has since been refined with additional reported outcomes in the literature. The commonalities among reported procedures include a Weil osteotomy for visualization of the plantar plate, completion of the plantar plate tear at the phalangeal base insertion, passage of suture using a specialized suture passer from various vendors, tying the suture dorsally through tunnel holes in the proximal phalanx, and extensor tendon lengthening as needed for residual tension (Fig. 13) [82, 87–90].
Fig. 13.
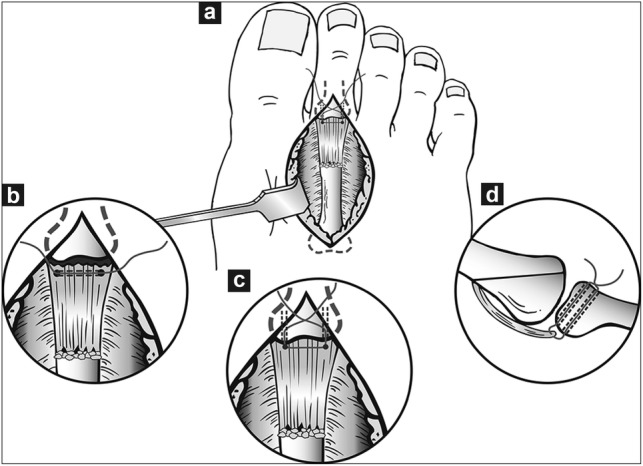
Method of plantar plate repair. a A dorsal incision is made over the affected MTP joint and adequate exposure of the plantar plate is achieved with a Weil osteotomy and release of adhesive tissue with a McGlamry elevator if necessary (not shown). b After completion of the plantar plate tear from the base of the proximal phalanx, sutures are passed through the distal plantar plate in a horizontal mattress pattern. c The sutures are then passed through two drill holes through the proximal phalanx base and tied dorsally. d A sagittal view of the MTP joint shows the repaired plantar plate and sutures passed through bone tunnels
Nery et al. reported the outcomes of 22 patients who underwent direct plantar plate repair [91]. The second MTP joint was the most commonly affected joint (63%) and all toes were more stable postoperatively, which correlated with improvement in the AOFAS score. Flint et al. performed a prospective case series to evaluate the results of 138 plantar plate repairs in 97 feet [92]. Patients were followed for 12 months. Eighty percent of patients had “good” to “excellent” satisfaction scores at 1 year and pain scores decreased from 5.4/10 to 1.5/10. Toes were generally stiffer, but more stable. However, there was not a significant increase in the ability to pass the “paper pullout test” following surgery (42% preoperative, 54% postoperative). The authors concluded that direct plantar plate repair through a dorsal approach has reliable outcomes and is a viable option for treating an unstable lesser MTP joint. This conclusion is corroborated by a retrospective study of 50 patients by Cook et al. who found that after 1 year, there was an increase in MTP joint stability in 92% of cases, as well as improvement in pain and function scores [92, 93].
A few papers have described alternative techniques or modifications to the above technique for plantar plate repair [94–96]. However, the outcomes of these procedures are even less studied than those of the dorsal approach reported in the literature.
In the span of the senior author’s career, understanding of lesser MTP joint instability has brought two major advancements: first, is the knowledge that plantar plate pathology is the primary cause of lesser MTP joint instability; and second, is the adoption of techniques to directly address the problem of instability by plantar plate repair. There is room for innovation in surgical technique. The future may bring modifications that further improve joint stability and restoration of anatomic function, such as restoration of the ability to pass the paper pull out test. As satisfaction is less than 100%, more needs to be done to understand risk factors for a less than satisfactory result to improve patient counseling as well as to anticipate adjunct procedures, such as temporary pinning of the toe.
Conclusion
This paper summarized the evolution of four forefoot pathologies in the last 4 decades: (1) mallet toe, (2) hammertoe, (3) neuroma, and (4) lesser metatarsophalangeal joint instability. The last 40 years have brought a vast array of knowledge and techniques in Foot and Ankle Surgery. As alluded to in the introduction of this paper, the definitive textbook on the subject in the 1970s was a 625 book by DuVries. Today, there are multiple reference textbooks for surgeons, one of which is a two-volume text for which the senior author has had the privilege to serve as the lead editor. In addition to dedicated chapters on specific forefoot pathologies, the published literature continues to grow with new investigations. As much as today’s surgeon is able to accurately diagnose and treat patients’ forefoot woes, there remains room for improvement—both in knowledge of the disease and development of improved techniques.
Author Contributions
This manuscript has been read and approved by all authors and represents honest work. Both authors contributed to the writing of this manuscript.
Funding
None.
Compliance with Ethical Standards
Conflict of Interest
The senior author, MC, has consulting relationships with Stryker & Arthrex, whose implants are referenced in this paper. The lead author, DD has no conflicts of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.DuVries HL. Surgery of the Foot. St. Louis: Mosby; 1959. [Google Scholar]
- 2.Coughlin MJ. Chapter 7. In: Coughlin M, Saltzman R, Anderson R, editors. Mann’s surgery of the foot and ankle. 9. Philadelphia, PA: Elsevier Saunders; 2014. pp. 357–361. [Google Scholar]
- 3.Jones S, Ali F, Genever A, Flowers MJ, Bostock SH. Distal interphalangeal joint arthrodesis of the lesser toes using the Barouk screw. The Foot. 2003;13(1):10–13. doi: 10.1016/s0958-2592(02)00113-x. [DOI] [Google Scholar]
- 4.Coughlin MJ, Dorris J, Polk E. Operative repair of the fixed hammertoe deformity. Foot and Ankle International. 2000;21(2):94–104. doi: 10.1177/107110070002100202. [DOI] [PubMed] [Google Scholar]
- 5.Kramer WC, Parman M, Marks RM. Hammertoe correction with k-wire fixation. Foot and Ankle International. 2015;36(5):494–502. doi: 10.1177/1071100714568013. [DOI] [PubMed] [Google Scholar]
- 6.Holinka J, Schuh R, Hofstaetter JG, Wanivenhaus AH. Temporary Kirschner wire transfixation versus strapping dressing after second MTP joint realignment surgery: a comparative study with ten-year follow-up. Foot and Ankle International. 2013;34(7):984–989. doi: 10.1177/1071100713478406. [DOI] [PubMed] [Google Scholar]
- 7.Canales MB, Razzante MC, Ehredt DJ, Jr, Clougherty CO. A simple method of intramedullary fixation for proximal interphalangeal arthrodesis. Journal of Foot and Ankle Surgery. 2014;53(6):817–824. doi: 10.1053/j.jfas.2014.03.017. [DOI] [PubMed] [Google Scholar]
- 8.Boffeli TJ, Thompson JC, Tabatt JA. Two-pin fixation of proximal interphalangeal joint fusion for hammertoe correction. Journal of Foot and Ankle Surgery. 2016;55(3):480–487. doi: 10.1053/j.jfas.2016.01.027. [DOI] [PubMed] [Google Scholar]
- 9.Rothermel SD, Aydogan U, Roush EP, Lewis GS. Proximal interphalangeal arthrodesis of lesser toes utilizing k-wires versus expanding implants: comparative biomechanical cadaveric study. Foot and Ankle International. 2019;40(2):231–236. doi: 10.1177/1071100718805066. [DOI] [PubMed] [Google Scholar]
- 10.Guelfi M, Pantalone A, Cambiaso Daniel J, Vanni D, Guelfi MGB, Salini V. Arthrodesis of proximal inter-phalangeal joint for hammertoe: intramedullary device options. J Orthop Traumatol. 2015;16(4):269–273. doi: 10.1007/s10195-015-0360-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Obrador C, Losa-Iglesias M, Becerro-de-Bengoa-Vallejo R, Kabbash CA. Comparative study of intramedullary hammertoe fixation. Foot and Ankle International. 2018;39(4):415–425. doi: 10.1177/1071100717745854. [DOI] [PubMed] [Google Scholar]
- 12.Richman SH, Siqueira MBP, McCullough KA, Berkowitz MJ. Correction of hammertoe deformity with novel intramedullary PIP fusion device versus k-wire fixation. Foot and Ankle International. 2017;38(2):174–180. doi: 10.1177/1071100716671883. [DOI] [PubMed] [Google Scholar]
- 13.Catena F, Doty JF, Jastifer J, Coughlin MJ, Stevens F. Prospective study of hammertoe correction with an intramedullary implant. Foot and Ankle International. 2014;35(4):319–325. doi: 10.1177/1071100713519780. [DOI] [PubMed] [Google Scholar]
- 14.Sandhu JS, DeCarbo WT, Hofbauer MH. Digital arthrodesis with a one-piece memory nitinol intramedullary fixation device: a retrospective review. Foot and Ankle Specialist. 2013;6(5):364–366. doi: 10.1177/1938640013496458. [DOI] [PubMed] [Google Scholar]
- 15.Scholl A, McCarty J, Scholl D, Mar A. Smart toe® implant versus buried Kirschner wire for proximal interphalangeal joint arthrodesis: a comparative study. Journal of Foot and Ankle Surgery. 2013;52(5):580–583. doi: 10.1053/j.jfas.2013.02.007. [DOI] [PubMed] [Google Scholar]
- 16.Payo-Ollero J, Casajús-Ortega A, Llombart-Blanco R, Villas C, Alfonso M. The efficacy of an intramedullary nitinol implant in the correction of claw toe or hammertoe deformities. Archives of Orthopaedic and Trauma Surgery. 2019 doi: 10.1007/s00402-019-03203-w. [DOI] [PubMed] [Google Scholar]
- 17.Jay RM, Malay DS, Landsman AS, Jennato N, Huish J, Younger M. Dual-component intramedullary implant versus Kirschner wire for proximal interphalangeal joint fusion: a randomized controlled clinical trial. Journal of Foot and Ankle Surgery. 2016;55(4):697–708. doi: 10.1053/j.jfas.2016.03.017. [DOI] [PubMed] [Google Scholar]
- 18.Basile A, Albo F, Via AG. Intramedullary fixation system for the treatment of hammertoe deformity. Journal of Foot and Ankle Surgery. 2015;54(5):910–916. doi: 10.1053/j.jfas.2015.04.004. [DOI] [PubMed] [Google Scholar]
- 19.Konkel KF, Sover ER, Menger AG, Halberg JM. Hammer toe correction using an absorbable pin. Foot and Ankle International. 2011;32(10):973–978. doi: 10.3113/FAI.2011.0973. [DOI] [PubMed] [Google Scholar]
- 20.Konkel KF, Menger AG, Retzlaff SA. Hammer toe correction using an absorbable intramedullary pin. Foot and Ankle International. 2007;28(8):916–920. doi: 10.3113/FAI.2007.0916. [DOI] [PubMed] [Google Scholar]
- 21.Albright RH, Waverly BJ, Klein E, Weil L, Jr, Weil LS, Sr, Fleischer AE. Percutaneous Kirschner wire versus commercial implant for hammertoe repair: a cost-effectiveness analysis. Journal of Foot and Ankle Surgery. 2018;57(2):332–338. doi: 10.1053/j.jfas.2017.10.019. [DOI] [PubMed] [Google Scholar]
- 22.Dieterle JO, Kuzma JF. A case of Morton’s metatarsalgia (Morton’s toe) treated by operation. Wisconsin Medical Journal. 1946;45:967. [PubMed] [Google Scholar]
- 23.Graham CE, Graham DM. Morton’s neuroma: a microscopic evaluation. Foot Ankle. 1984;5(3):150–153. doi: 10.1177/107110078400500308. [DOI] [PubMed] [Google Scholar]
- 24.Graham CE, Johnson KA, Ilstrup DM. The intermetatarsal nerve: a microscopic evaluation. Foot Ankle. 1981;2(3):150–152. doi: 10.1177/107110078100200305. [DOI] [PubMed] [Google Scholar]
- 25.Ha’Eri, G.B., Fornasier, V.L., Schatzker, J. (1979). Morton’s neuroma—pathogenesis and ultrastructure. Clinical Orthopaedics and Related Research, (141), 256–259. [PubMed]
- 26.Mann RA, Reynolds JC. Interdigital neuroma–a critical clinical analysis. Foot Ankle. 1983;3(4):238–243. doi: 10.1177/107110078300300411. [DOI] [PubMed] [Google Scholar]
- 27.Addante JB, Peicott PS, Wong KY, Brooks DL. Interdigital neuromas. Results of surgical excision of 152 neuromas. Journal of the American Podiatric Medical Association. 1986;76(9):493–495. doi: 10.7547/87507315-76-9-493. [DOI] [PubMed] [Google Scholar]
- 28.Karges DE. Plantar excision of primary interdigital neuromas. Foot Ankle. 1988;9(3):120–124. doi: 10.1177/107110078800900305. [DOI] [PubMed] [Google Scholar]
- 29.Friscia DA, Strom DE, Parr JW, Saltzman CL, Johnson KA. Surgical treatment for primary interdigital neuroma. Orthopedics. 1991;14(6):669–672. doi: 10.3928/0147-7447-19910601-07. [DOI] [PubMed] [Google Scholar]
- 30.Coughlin MJ, Pinsonneault T. Operative treatment of interdigital neuroma. A long-term follow-up study. Journal of Bone and Joint Surgery. 2001;83(9):1321–1328. [PubMed] [Google Scholar]
- 31.Levitsky KA, Alman BA, Jevsevar DS, Morehead J. Digital nerves of the foot: anatomic variations and implications regarding the pathogenesis of interdigital neuroma. Foot Ankle. 1993;14(4):208–214. doi: 10.1177/107110079301400406. [DOI] [PubMed] [Google Scholar]
- 32.Valero J, Gallart J, González D, Deus J, Lahoz M. Multiple interdigital neuromas: a retrospective study of 279 feet with 462 neuromas. Journal of Foot and Ankle Surgery. 2015;54(3):320–322. doi: 10.1053/j.jfas.2014.05.011. [DOI] [PubMed] [Google Scholar]
- 33.Bucknall V, Rutherford D, MacDonald D, Shalaby H, McKinley J, Breusch SJ. Outcomes following excision of Morton’s interdigital neuroma: a prospective study. The Bone and Joint Journal. 2016;98-B(10):1376–1381. doi: 10.1302/0301-620X.98B10.37610. [DOI] [PubMed] [Google Scholar]
- 34.Reichert P, Zimmer K, Witkowski J, Wnukiewicz W, Kuliński S, Gosk J. Long-term results of neurectomy through a dorsal approach in the treatment of Morton’s Neuroma. Advances in Clinical and Experimental Medicine. 2016;25(2):295–302. doi: 10.17219/acem/60249. [DOI] [PubMed] [Google Scholar]
- 35.Kasparek M, Schneider W. Surgical treatment of Morton’s neuroma: clinical results after open excision. International Orthopaedics. 2013;37(9):1857–1861. doi: 10.1007/s00264-013-2002-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lee KT, Kim JB, Young KW, Park YU, Kim JS, Jegal H. Long-term results of neurectomy in the treatment of Morton’s neuroma: more than 10 years’ follow-up. Foot and Ankle Specialist. 2011;4(6):349–353. doi: 10.1177/1938640011428510. [DOI] [PubMed] [Google Scholar]
- 37.Pace A, Scammell B, Dhar S. The outcome of Morton’s neurectomy in the treatment of metatarsalgia. International Orthopaedics. 2010;34(4):511–515. doi: 10.1007/s00264-009-0812-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nery C, Raduan F, Del Buono A, Asaumi ID, Maffulli N. Plantar approach for excision of a Morton neuroma: a long-term follow-up study. Journal of Bone and Joint Surgery. 2012;94(7):654–658. doi: 10.2106/JBJS.K.00122. [DOI] [PubMed] [Google Scholar]
- 39.Kundert H-P, Plaass C, Stukenborg-Colsman C, Waizy H. Excision of Morton’s neuroma using a longitudinal plantar approach: A midterm follow-up study. Foot and Ankle Specialist. 2016;9(1):37–42. doi: 10.1177/1938640015599032. [DOI] [PubMed] [Google Scholar]
- 40.Faraj AA, Hosur A. The outcome after using two different approaches for excision of Morton’s neuroma. Chinese Medical Journal. 2010;123(16):2195–2198. [PubMed] [Google Scholar]
- 41.Valisena S, Petri GJ, Ferrero A. Treatment of Morton’s neuroma: A systematic review. Foot and Ankle Surgery. 2018;24(4):271–281. doi: 10.1016/j.fas.2017.03.010. [DOI] [PubMed] [Google Scholar]
- 42.Lee J, Kim J, Lee M, Chu I, Lee S, Gwak H. Morton’s neuroma (interdigital neuralgia) treated with metatarsal sliding osteotomy. Indian Journal of Orthopaedics. 2017;51(6):692–696. doi: 10.4103/0019-5413.217678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kubota M, Ohno R, Ishijima M, et al. Minimally invasive endoscopic decompression of the intermatatarsal nerve for Morton’s neuroma. Journal of Orthopaedics. 2015;12(Suppl 1):S101–S104. doi: 10.1016/j.jor.2014.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Zelent ME, Kane RM, Neese DJ, Lockner WB. Minimally invasive Morton’s intermetatarsal neuroma decompression. Foot and Ankle International. 2007;28(2):263–265. doi: 10.3113/FAI.2007.0263. [DOI] [PubMed] [Google Scholar]
- 45.Naraghi R, Slack-Smith L, Bryant A. Plantar pressure measurements and geometric analysis of patients with and without Morton’s neuroma. Foot and Ankle International. 2018;39(7):829–835. doi: 10.1177/1071100718766553. [DOI] [PubMed] [Google Scholar]
- 46.Kim J-Y, Choi JH, Park J, Wang J, Lee I. An anatomical study of Morton’s interdigital neuroma: the relationship between the occurring site and the deep transverse metatarsal ligament (DTML) Foot and Ankle International. 2007;28(9):1007–1010. doi: 10.3113/FAI.2007.1007. [DOI] [PubMed] [Google Scholar]
- 47.Brodsky JW, Passmore RN, Shabat S. Transection of the plantar plate and the flexor digitorum longus tendon of the fourth toe as a complication of endoscopic treatment of interdigital neuroma. A case report. Journal of Bone and Joint Surgery American. 2004;86(10):2299–2301. doi: 10.2106/00004623-200410000-00026. [DOI] [PubMed] [Google Scholar]
- 48.Ratanshi I, Hayakawa TEJ, Giuffre JL. Excision with interpositional nerve grafting: An alternative technique for the treatment of Morton Neuroma. Annals of Plastic Surgery. 2016;76(4):428–433. doi: 10.1097/SAP.0000000000000727. [DOI] [PubMed] [Google Scholar]
- 49.Rungprai C, Cychosz CC, Phruetthiphat O, Femino JE, Amendola A, Phisitkul P. Simple neurectomy versus neurectomy with intramuscular implantation for interdigital neuroma: A comparative study. Foot and Ankle International. 2015;36(12):1412–1424. doi: 10.1177/1071100715596741. [DOI] [PubMed] [Google Scholar]
- 50.Vito GR, Talarico LM. A modified technique for Morton’s neuroma. Decompression with relocation. Journal of the American Podiatric Medical Association. 2003;93(3):190–194. doi: 10.7547/87507315-93-3-190. [DOI] [PubMed] [Google Scholar]
- 51.Wolfort SF, Dellon AL. Treatment of recurrent neuroma of the interdigital nerve by implantation of the proximal nerve into muscle in the arch of the foot. Journal of Foot and Ankle Surgery. 2001;40(6):404–410. doi: 10.1016/s1067-2516(01)80009-0. [DOI] [PubMed] [Google Scholar]
- 52.Perini L, Perini C, Tagliapietra M, et al. Percutaneous alcohol injection under sonographic guidance in Morton’s neuroma: follow-up in 220 treated lesions. La Radiologia Medica. 2016;121(7):597–604. doi: 10.1007/s11547-016-0622-9. [DOI] [PubMed] [Google Scholar]
- 53.Pasquali C, Vulcano E, Novario R, Varotto D, Montoli C, Volpe A. Ultrasound-guided alcohol injection for Morton’s neuroma. Foot and Ankle International. 2015;36(1):55–59. doi: 10.1177/1071100714551386. [DOI] [PubMed] [Google Scholar]
- 54.Magnan B, Marangon A, Frigo A, Bartolozzi P. Local phenol injection in the treatment of interdigital neuritis of the foot (Morton’s neuroma) Chirurgia Degli Organi di Movimento. 2005;90(4):371–377. [PubMed] [Google Scholar]
- 55.Santos D, Morrison G, Coda A. Sclerosing alcohol injections for the management of intermetatarsal neuromas: A systematic review. Foot. 2018;35:36–47. doi: 10.1016/j.foot.2017.12.003. [DOI] [PubMed] [Google Scholar]
- 56.Gurdezi S, White T, Ramesh P. Alcohol injection for Morton’s neuroma: a five-year follow-up. Foot and Ankle International. 2013;34(8):1064–1067. doi: 10.1177/1071100713489555. [DOI] [PubMed] [Google Scholar]
- 57.Espinosa N, Seybold JD, Jankauskas L, Erschbamer M. Alcohol sclerosing therapy is not an effective treatment for interdigital neuroma. Foot and Ankle International. 2011;32(6):576–580. doi: 10.3113/FAI.2011.0576. [DOI] [PubMed] [Google Scholar]
- 58.Lee K, Hwang I-Y, Ryu CH, Lee JW, Kang SW. Ultrasound-guided hyaluronic acid injection for the management of Morton’s Neuroma. Foot and Ankle International. 2018;39(2):201–204. doi: 10.1177/1071100717739578. [DOI] [PubMed] [Google Scholar]
- 59.Campbell CM, Diamond E, Schmidt WK, et al. A randomized, double-blind, placebo-controlled trial of injected capsaicin for pain in Morton’s neuroma. Pain. 2016;157(6):1297–1304. doi: 10.1097/j.pain.0000000000000544. [DOI] [PubMed] [Google Scholar]
- 60.Lizano-Díez X, Ginés-Cespedosa A, Alentorn-Geli E, et al. corticosteroid injection for the treatment of Morton’s neuroma: a prospective, double-blinded, randomized. Placebo-Controlled Trial. Foot and Ankle International. 2017;38(9):944–951. doi: 10.1177/1071100717709569. [DOI] [PubMed] [Google Scholar]
- 61.Masala S, Cuzzolino A, Morini M, Raguso M, Fiori R. Ultrasound-guided percutaneous radiofrequency for the treatment of Morton’s neuroma. Cardiovascular and Interventional Radiology. 2018;41(1):137–144. doi: 10.1007/s00270-017-1786-y. [DOI] [PubMed] [Google Scholar]
- 62.Brooks D, Parr A, Bryceson W. Three cycles of radiofrequency ablation are more efficacious than two in the management of Morton’s Neuroma. Foot and Ankle Specialist. 2018;11(2):107–111. doi: 10.1177/1938640017709905. [DOI] [PubMed] [Google Scholar]
- 63.Seok H, Kim S-H, Lee SY, Park SW. Extracorporeal shockwave therapy in patients with Morton’s Neuroma a randomized, placebo-controlled trial. Journal of the American Podiatric Medical Association. 2016;106(2):93–99. doi: 10.7547/14-131. [DOI] [PubMed] [Google Scholar]
- 64.Deniz S, Purtuloglu T, Tekindur S, et al. Ultrasound-guided pulsed radio frequency treatment in Morton’s neuroma. Journal of the American Podiatric Medical Association. 2015;105(4):302–306. doi: 10.7547/13-128.1. [DOI] [PubMed] [Google Scholar]
- 65.Fridman R, Cain JD, Weil L., Jr Extracorporeal shockwave therapy for interdigital neuroma: a randomized, placebo-controlled, double-blind trial. Journal of the American Podiatric Medical Association. 2009;99(3):191–193. doi: 10.7547/0980191. [DOI] [PubMed] [Google Scholar]
- 66.Park YH, Choi WS, Choi GW, Kim HJ. Intra- and interobserver reliability of size measurement of morton neuromas on sonography. Journal of Ultrasound in Medicine. 2019 doi: 10.1002/jum.14928. [DOI] [PubMed] [Google Scholar]
- 67.Cohen SL, Miller TT, Ellis SJ, Roberts MM, DiCarlo EF. Sonography of Morton Neuromas: What are we really looking at? Journal of Ultrasound in Medicine. 2016;35(10):2191–2195. doi: 10.7863/ultra.15.11022. [DOI] [PubMed] [Google Scholar]
- 68.Bignotti B, Signori A, Sormani MP, Molfetta L, Martinoli C, Tagliafico A. Ultrasound versus magnetic resonance imaging for Morton neuroma: systematic review and meta-analysis. European Radiology. 2015;25(8):2254–2262. doi: 10.1007/s00330-015-3633-3. [DOI] [PubMed] [Google Scholar]
- 69.Torres-Claramunt R, Ginés A, Pidemunt G, Puig L, de Zabala S. MRI and ultrasonography in Morton’s neuroma: Diagnostic accuracy and correlation. Indian J Orthopaedics. 2012;46(3):321–325. doi: 10.4103/0019-5413.96390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Park H-J, Kim SS, Rho M-H, Hong H-P, Lee S-Y. Sonographic appearances of Morton’s neuroma: differences from other interdigital soft tissue masses. Ultrasound in Medicine and Biology. 2011;37(8):1204–1209. doi: 10.1016/j.ultrasmedbio.2011.05.008. [DOI] [PubMed] [Google Scholar]
- 71.Weishaupt D, Treiber K, Kundert H-P, et al. Morton neuroma: MR imaging in prone, supine, and upright weight-bearing body positions. Radiology. 2003;226(3):849–856. doi: 10.1148/radiol.2263011925. [DOI] [PubMed] [Google Scholar]
- 72.Hidalgo-Ovejero AM, Martinez-Grande M, Sanchez-Villares JJ, Garcia-Mata S, Lasanta P. Clinical examination and imaging studies in the diagnosis of interdigital neuroma. Journal of Bone and Joint Surgery American. 2002;84(7):1276–1277. doi: 10.2106/00004623-200207000-00032. [DOI] [PubMed] [Google Scholar]
- 73.Aydinlar EI, Uzun M, Beksac B, Ozden VE, Karaarslan E, Oge AE. Simple electrodiagnostic method for Morton neuroma. Muscle and Nerve. 2014;49(2):193–197. doi: 10.1002/mus.23899. [DOI] [PubMed] [Google Scholar]
- 74.Ruiz Santiago F, Prados Olleta N, Tomás Muñoz P, Guzmán Álvarez L, Martínez Martínez A. Short term comparison between blind and ultrasound guided injection in morton neuroma. European Radiology. 2019;29(2):620–627. doi: 10.1007/s00330-018-5670-1. [DOI] [PubMed] [Google Scholar]
- 75.Tagliafico A, Bignotti B, Martinoli C. Update on ultrasound-guided interventional procedures on peripheral nerves. Semin Musculoskelet Radiol. 2016;20(5):453–460. doi: 10.1055/s-0036-1594282. [DOI] [PubMed] [Google Scholar]
- 76.Coughlin M, Saltzman C, Anderson R. Mann's surgery of the foot and ankle. 9. Philadelphia, PA: Elsevier Sanders; 2014. [Google Scholar]
- 77.Coughlin MJ. Chapter 12. In: Coughlin M, Mann R, editors. Mann’s surgery of the foot and ankle. 7. Philadelphia, PA: Elsevier Saunders; 1999. [Google Scholar]
- 78.Coughlin MJ. Chapter 7. In: Coughlin M, Mann R, Saltzman C, editors. Mann’s surgery of the foot and ankle. 8. Philadelphia, PA: Elsevier Saunders; 1999. [Google Scholar]
- 79.Coughlin MJ. Crossover second toe deformity. Foot Ankle. 1987;8(1):29–39. doi: 10.1177/107110078700800108. [DOI] [PubMed] [Google Scholar]
- 80.Deland JT, Sung IH. The medial crossover toe: a cadaveric dissection. Foot and Ankle International. 2000;21(5):375–378. doi: 10.1177/107110070002100503. [DOI] [PubMed] [Google Scholar]
- 81.Coughlin MJ, Schutt SA, Hirose CB, et al. Metatarsophalangeal joint pathology in crossover second toe deformity: a cadaveric study. Foot and Ankle International. 2012;33(2):133–140. doi: 10.3113/FAI.2012.0133. [DOI] [PubMed] [Google Scholar]
- 82.Coughlin MJ, Baumfeld DS, Nery C. Second MTP joint instability: grading of the deformity and description of surgical repair of capsular insufficiency. The Physician and Sportsmedicine. 2011;39(3):132–141. doi: 10.3810/psm.2011.09.1929. [DOI] [PubMed] [Google Scholar]
- 83.Bouché RT, Heit EJ. Combined plantar plate and hammertoe repair with flexor digitorum longus tendon transfer for chronic, severe sagittal plane instability of the lesser metatarsophalangeal joints: preliminary observations. Journal of Foot and Ankle Surgery. 2008;47(2):125–137. doi: 10.1053/j.jfas.2007.12.008. [DOI] [PubMed] [Google Scholar]
- 84.Blitz NM, Ford LA, Christensen JC. Plantar plate repair of the second metatarsophalangeal joint: technique and tips. Journal of Foot and Ankle Surgery. 2004;43(4):266–270. doi: 10.1053/j.jfas.2004.05.011. [DOI] [PubMed] [Google Scholar]
- 85.Powless SH, Elze ME. Metatarsophalangeal joint capsule tears: an analysis by arthrography, a new classification system and surgical management. Journal of Foot and Ankle Surgery. 2001;40(6):374–389. doi: 10.1016/s1067-2516(01)80005-3. [DOI] [PubMed] [Google Scholar]
- 86.Gregg J, Silberstein M, Clark C, Schneider T. Plantar plate repair and Weil osteotomy for metatarsophalangeal joint instability. Foot and Ankle Surgery. 2007;13(3):116–121. doi: 10.1016/j.fas.2007.01.001. [DOI] [Google Scholar]
- 87.Weil L, Jr, Sung W, Weil LS, Sr, Malinoski K. Anatomic plantar plate repair using the Weil metatarsal osteotomy approach. Foot and Ankle Specialist. 2011;4(3):145–150. doi: 10.1177/1938640010397342. [DOI] [PubMed] [Google Scholar]
- 88.Hsu RY, Barg A, Nickisch F. Lesser metatarsophalangeal joint instability: Advancements in plantar plate reconstruction. Foot and Ankle Clinics. 2018;23(1):127–143. doi: 10.1016/j.fcl.2017.09.009. [DOI] [PubMed] [Google Scholar]
- 89.Watson TS, Reid DY, Frerichs TL. Dorsal approach for plantar plate repair with weil osteotomy: Operative technique. Foot and Ankle International. 2014;35(7):730–739. doi: 10.1177/1071100714536540. [DOI] [PubMed] [Google Scholar]
- 90.Cooper MT, Coughlin MJ. Sequential dissection for exposure of the second metatarsophalangeal joint. Foot and Ankle International. 2011;32(3):294–299. doi: 10.3113/FAI.2011.0294. [DOI] [PubMed] [Google Scholar]
- 91.Nery C, Coughlin MJ, Baumfeld D, Mann TS. Lesser metatarsophalangeal joint instability: prospective evaluation and repair of plantar plate and capsular insufficiency. Foot and Ankle International. 2012;33(4):301–311. doi: 10.3113/FAI.2012.0301. [DOI] [PubMed] [Google Scholar]
- 92.Flint WW, Macias DM, Jastifer JR, Doty JF, Hirose CB, Coughlin MJ. Plantar plate repair for lesser metatarsophalangeal joint instability. Foot and Ankle International. 2017;38(3):234–242. doi: 10.1177/1071100716679110. [DOI] [PubMed] [Google Scholar]
- 93.Cook JJ, Cook EA, Hansen DD, et al. One-year outcome study of anatomic reconstruction of lesser metatarsophalangeal joints. Foot and Ankle Specialist. 2019 doi: 10.1177/1938640019846974. [DOI] [PubMed] [Google Scholar]
- 94.McCartan BL, Juels CA, Shih JA. Technique and tips for multiplanar correction of plantar plate repairs in lesser metatarsophalangeal joints. Journal of the American Podiatric Medical Association. 2019;109(1):80–86. doi: 10.7547/17-086. [DOI] [PubMed] [Google Scholar]
- 95.Clements JR, Ghai AK. An innovative method for plantar plate repair: Technique guide and case report. Journal of Foot and Ankle Surgery. 2019;58(3):555–561. doi: 10.1053/j.jfas.2018.09.006. [DOI] [PubMed] [Google Scholar]
- 96.Prissel MA, Hyer CF, Donovan JK, Quisno AL. Plantar plate repair using a direct plantar approach: An outcomes analysis. Journal of Foot and Ankle Surgery. 2017;56(3):434–439. doi: 10.1053/j.jfas.2016.12.002. [DOI] [PubMed] [Google Scholar]