
Figure 4.
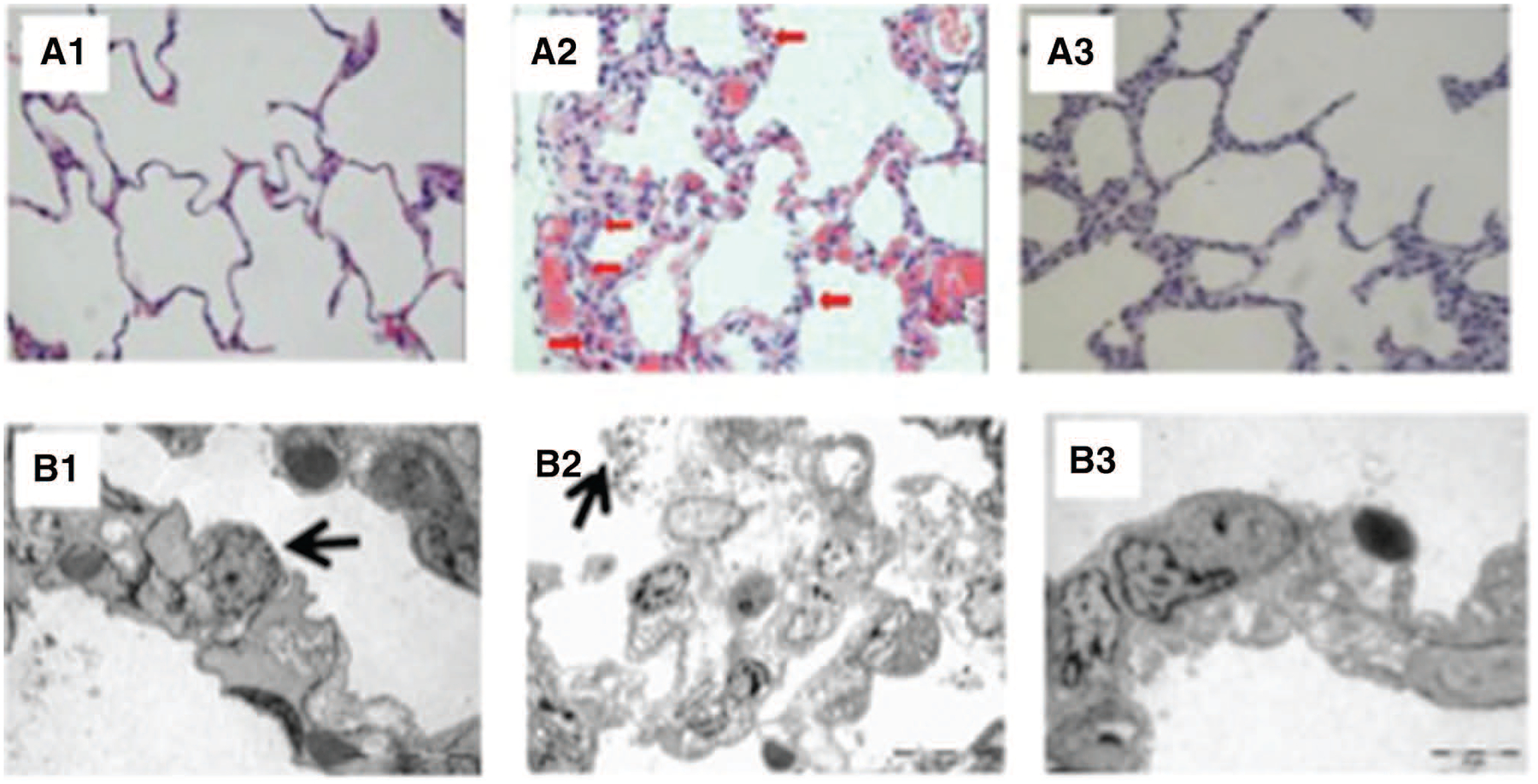
Histologic images obtained from the ventral pulmonary fragments of the control (left), cardiopulmonary bypass (CPB; middle), and lung perfusion (right) groups using light (upper; magnification 400×) and electron (lower) microscopy. As can be seen in the panel A2, the interalveolar septa were thickened by edema and infiltrated by polymorphonuclear (red arrows), thickening of the intraalveolar septa, while the interalveolar septa integrity was preserved in the lung perfusion group (A3). Panel B1 shows an electron micrograph from a lung fragment from the control group where the alveolar septa and capillaries are normal, and the histoarchitecture of the alveolar space is maintained. Note a type II pneumocyte, with lamellar bodies (arrow). Panel B2 shows a lung fragment from the CPB group (970×). Notice the extended edema vacuolization of the alveolar septa resulting in a consequent thickness of interalveolar septa. There are signs of extrusion of surfactant vesicles of surfactant into alveolar spaces (arrow). Panel B3 shows that the histoarchitecture of the interalveolar septa and capillaries was preserved, as well as the absence of interstitial edema (1650×).