

Abstract
Introduction Textiloma (Txm) is a nonmedical term that has been given to foreign body-related inflammatory pseudotumor arising from retained nonabsorbable cotton matrix that is either inadvertently or deliberately left behind during surgery, which may trigger an inflammatory reaction. This report describes a case of Txm mimicking a recurrent high-grade astrocytoma.
Case Report We, here, present the case of a 69-year-old female with a 6-month history of progressive left-sided weakness. Neuroimaging studies revealed a large nonenhancing mass in the right frontoparietal lobe. Pathology reported a World Health Organization tumor classification grade II, diffuse astrocytoma. After surgical intervention, external beam radiation was given to the remaining areas of residual tumor. Routine magnetic resonance imaging (MRI) revealed a nodular area of contrast enhancement in the dorsal and inferior margin of the biopsy tract, growing between interval scans, and perfusion-weighted imaging parameters were elevated being clinically asymptomatic. She underwent a complete resection of this area of interest and pathology returned as a Txm with Surgicel fibers.
Conclusion After treatment of a neoplasm, if unexpected clinical or imaging evidence of recurrence is present, a foreign body reaction to hemostatic material used during the initial surgery should be included in the differential diagnosis.
Keywords: foreign body, astrocytoma, neoplasm recurrence, local, textiloma
Introduction
Textiloma (Txm) is a nonmedical term that has been given to foreign body-related inflammatory pseudotumor arising from retained nonabsorbable cotton matrix that is either inadvertently or deliberately left behind during surgery, which may trigger an inflammatory reaction. In current neurosurgical practice, Txm often refers to a resorbable hemostatic agent that is intentionally left in place to prevent the potentially disastrous consequences of postoperative intracranial hemorrhage. The vast majority of neurosurgical patients in whom resorbable hemostatic agents are left in place remain asymptomatic. 1
Txms in the field of neurosurgery have been found mostly in patients with subdural lesions postcraniotomy. This report describes a case of Txm mimicking a recurrent high-grade astrocytoma, highlighting the importance of recognizing this entity in the setting of tumoral recurrence.
Case Report
A 69-year-old right-handed female presented to our facility with a 6-month history of progressive left-sided weakness. She was initially managed by an outside facility as a stroke but she continued clinically deteriorating. After neuroimaging was obtained, a biopsy was performed on a large, nonenhancing mass in the right frontoparietal lobe. Pathology reported a diffuse astrocytoma, World Health Organization grade II with wild type isocitrate dehydrogenase 1 by immunohistochemistry, epidermal growth factor receptor amplification, and phosphatase and tensin homolog negative results by fluorescent in situ hybridization analysis. She received external beam radiation to the areas of residual tumor with a total dose of 54 Gy.
During a routine evaluation, 4 months after completion of radiation therapy, a magnetic resonance imaging (MRI) revealed a nodular area of contrast enhancement dorsal and inferior to the margin of the biopsy tract, growing between interval scans ( Fig. 1 ). Advanced MRI techniques using dynamic susceptibility contrast perfusion-weighted imaging (PWI) reported elevated relative cerebral blood volume (rCBV) up to 3:1 when compared with the contralateral white matter, supporting hyperperfusion and tumor recurrence. Of note, she was clinically asymptomatic.
Fig. 1.
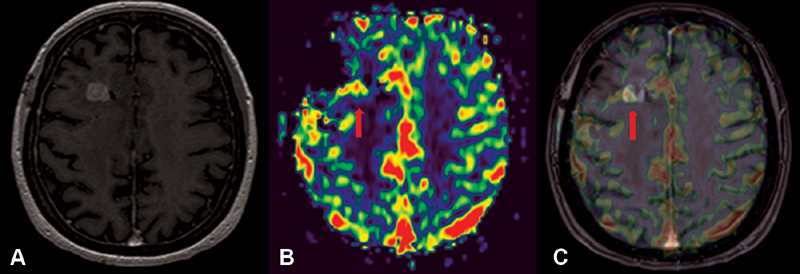
Advanced magnetic resonance imaging of the case. ( A ) Contrasting axial image in T1 with gadolinium, ( B ) perfusion map rCBV, ( C ) image fusion rCBV/MRI. Nodular area of contrast enhancement in the dorsal margin of the biopsy tract, with elevated rCBV, suggesting hyperperfusion (arrows). MRI, magnetic resonance imaging; rCBV, relative cerebral blood volume.
After the biopsy, she underwent a complete resection of this area. The pathology returned as a Txm with Surgicel fibers ( Fig. 2 ). Reactive changes were also seen consistent with radiation effect and areas of atypical cells consistent with residual tumor but not significantly mitotically active. She did not require any further treatments and continued MRI surveillance for 14 months until another area of progression was seen.
Fig. 2.
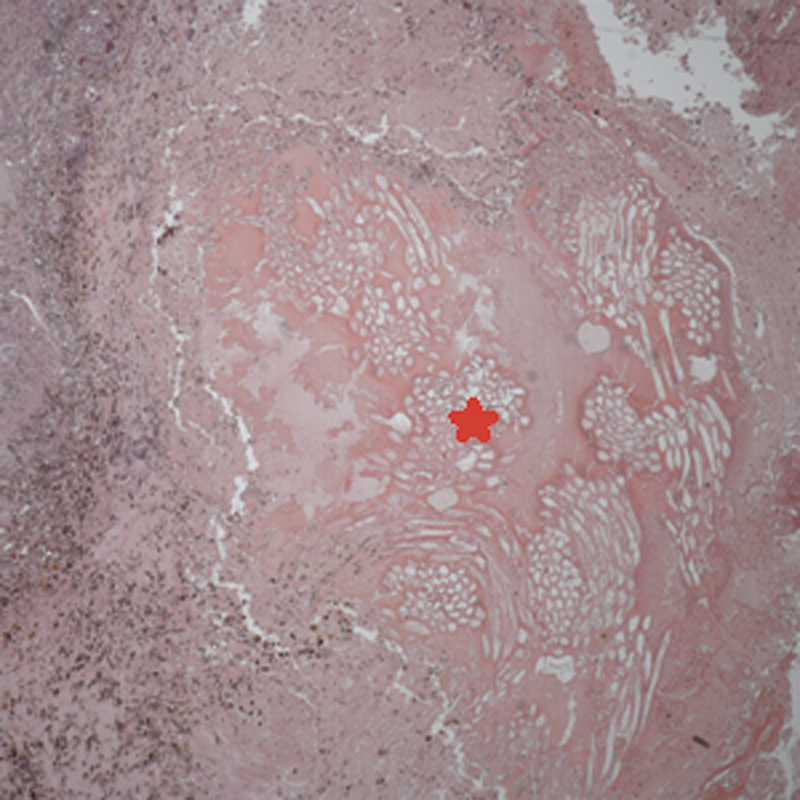
Low power (×40 original magnification) micrograph of Txm showing optically clear bundles of foreign material ( * ) with morphology consistent with oxidized cellulose that is used for hemostasis. The left portion of the micrograph shows fibrosis, hemosiderin-laden macrophages, and chronic inflammation (H & E). H & E, hematoxylin and eosin.
Discussion
Intracranial and spinal Txm sometimes can manifest with early severe symptoms, neurological deficits, pain, or seizures but, generally, they are nonspecific or asymptomatic, like in our case. This inflammatory reaction is commonly misdiagnosed as an abscess, tumor reoccurrence, radiation necrosis, infarction, or primary neoplasm. 2 Our case shows a clinical scenario similar to a pseudoprogression phenomenon in which radiographic changes from treatments are not easy to distinguish from recurrent tumor. Pseudoprogression characterizes a well-described phenomenon in patients with high-grade gliomas (HGG) treated with radiation and chemotherapy in which radiographic changes, such as new areas of contrast enhancement and edema occur early after treatments. 3
Foreign-body reactions encountered in neurosurgical practice; however, they are very rare and they are usually due to hemostatic agents that are deliberately left behind during craniotomies. Surgicel, or oxidized cellulose polymer, is composed of polyanhydroglucuronic acid that is woven into surgical gauze fibers and primarily used to coagulate bleeding vessels. Txm composed of oxidized regenerated cellulose (Surgicel; Ethicon, Inc. and Johnson & Johnson, Inc.) have been previously reported. 1
For evaluation of Txm, a computed tomography (CT) scan is the imaging technique of choice. Suggested CT findings are low-density heterogeneous masses with a hyperdense rim with enhancement after contrast injection. In MRI, a heterogeneous structure with a low-signal intensity, wavy pattern at T1 and a high-signal intensity at T2 has been reported. Txm cannot be easily distinguished from a recurrent tumor or abscess due to their nonspecific characteristics. 4 Therefore, careful history taking about previous operations and being aware of Txm are very important for imaging diagnosis.
In regards to advanced neuroimaging, only a few reports have included diffusion imaging and apparent diffusion coefficient mapping in Txm, mainly as a tool for distinguish them from brain abscess. 5 The lack of low apparent diffusion coefficient centrally within the lesion favors against abscess and could push toward the other diagnoses including Txm. MRI spectroscopy has the potential to differentiate between tumor and infection/inflammation, thus it helps in selecting cases to identify a recurrent tumor from other lesions. 2 In our case, the use of advanced neuroimaging with dynamic susceptibility contrast PWI suggested transformation to a HGG but the corresponding high-grade features were not visible on the pathology specimen.
Ribalta et al 1 conducted a study in which five patients with Txm were identified, all of which based on the clinical and neuroimaging findings, suggested a recurrent tumor or tumor progression prompting the resection of the mass. In our case, the use of dynamic susceptibility contrast PWI suggested transformation to a HGG which also prompted surgical excision of the mass.
Conclusions
After treatment of a neoplasm, if unexpected clinical or imaging evidence of recurrence is present, a foreign body reaction to hemostatic material used during the initial surgery should be included in the differential diagnosis which could often spare patients from unnecessary therapies. Standard conventional neuroimaging and advanced techniques have limitations. The standardization of advanced MRI is well recognized as a pressing clinical and research need.
Acknowledgments
Dr. Teresa Ribalta, Department of Pathology, Hospital Clinic, University of Barcelona, Barcelona, Spain; Dr. Gregory N. Fuller, Department of Pathology, The University of Texas MD Anderson Cancer Center, Houston, Texas, United States, Department of Pathology, Baylor University Medical Center, Dallas, Texas, United States, Department of Radiology, Baylor University Medical Center, Dallas, Texas, United States.
Footnotes
Conflicts of Interest None.
References
- 1.Ribalta T, McCutcheon I E, Neto A G et al. Textiloma (gossypiboma) mimicking recurrent intracranial tumor. Arch Pathol Lab Med. 2004;128(07):749–758. doi: 10.5858/2004-128-749-TGMRIT. [DOI] [PubMed] [Google Scholar]
- 2.Peloquin P, Vannemreddy P SSV, Watkins L M, Byrne R W. Intracranial cotton ball gossypiboma mimicking recurrent meningioma: report of a case with literature review for intentional and unintentional foreign body granulomas. Clin Neurol Neurosurg. 2012;114(07):1039–1041. doi: 10.1016/j.clineuro.2012.01.046. [DOI] [PubMed] [Google Scholar]
- 3.Melguizo-Gavilanes I, Bruner J M, Guha-Thakurta N, Hess K R, Puduvalli V K. Characterization of pseudoprogression in patients with glioblastoma: is histology the gold standard? J Neurooncol. 2015;123(01):141–150. doi: 10.1007/s11060-015-1774-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Aydogan M, Mirzanli C, Ganiyusufoglu K, Tezer M, Ozturk I. A 13-year-old textiloma (gossypiboma) after discectomy for lumbar disc herniation: a case report and review of the literature. Spine J. 2007;7(05):618–621. doi: 10.1016/j.spinee.2006.08.004. [DOI] [PubMed] [Google Scholar]
- 5.Bilginer B, Yavuz K, Agayev K, Akbay A, Ziyal I M.Existence of cotton granuloma after removal of a parasagittal meningioma: clinical and radiological evaluation -a case report- Kobe J Med Sci 200753(1,2):43–47. [PubMed] [Google Scholar]