

Abstract
Therapeutic plasma exchange, consisting of removing blood plasma and exchanging it with donated blood products, has been proposed for treating Alzheimer's disease (AD) to remove senescent or toxic factors. In preclinical studies, administration of plasma from young healthy mice to AD transgenic mice improved cognitive deficits without affecting brain amyloid plaques. Initial encouraging results have been collected in a double‐blind, placebo‐controlled study in nine AD patients receiving young plasma. In a 14‐month double‐blind, placebo‐controlled study in 322 AD patients, multiple infusions with plasma enriched with albumin with or without immunoglobulins slowed cognitive, functional, and clinical decline, especially in moderately affected patients. Clinical trials of plasma fractions containing hypothetically beneficial proteins are also under way. These initial positive clinical results need to be confirmed in larger and more rigorous controlled studies in which the possible benefits of plasma exchange approaches can be weighed against the intrinsic side effects of repetitive infusion procedures.
Keywords: Alzheimer's disease, parabiosis, plasma exchange therapy; plasmapheresis; therapeutic plasma exchange
1. INTRODUCTION
Alzheimer's disease (AD) is a chronic neurodegenerative disease that usually starts slowly and gradually worsens over time. It is the cause of approximately 70% of cases of dementia. The most common early symptom is difficulty in remembering recent events. As the disease advances, symptoms can include problems with language, disorientation for time and space, apathy, mood disturbances, inability to perform key activities of daily living, and behavioral issues. Gradually, basic activities are lost, ultimately leading to death. Although the speed of progression can vary, typical life expectancy after diagnosis is 3 to 8 years. As general life expectancy increases, the number of AD cases worldwide is expected to almost double every 20 years, from >50 million in 2018 to >152 million by 2050. The cause of AD is poorly understood. Risk for AD is partially driven by genetics and several risk loci have been identified. A recent meta‐analysis identified 29 risk loci, implicating 215 potential causative genes. Gene‐set analyses indicated biological mechanisms included immunity processes, lipid metabolism, tau binding proteins, and amyloid precursor protein metabolism. Histologically, the AD brain is characterized by extraneuronal plaques of amyloid β (Aβ), intraneuronal neurofibrillary tangles of hyperphosphorylated‐tau, dysfunctional microglia, reactive astrocytes, and dystrophic neurites. No treatments stop or reverse the progression of AD, although cholinesterase inhibitors or the N‐methyl‐D‐aspartate (NMDA)‐antagonist memantine may temporarily improve symptoms. New drug development in AD is very slow and suffers a high attrition rate. Molecules showing promise in animal studies have not confirmed that promise in the clinic.
2. PATHOPHYSIOLOGY AND ANTI‐Ab THERAPEUTIC APPROACHES TO ALZHEIMER'S DISEASE
The AD brain is histologically characterized by the presence of intracellular neurofibrillary tangles and extracellular plaques. The plaques are composed of Aβ, a 40‐ to 42‐amino acid peptide mediating physiological neuronal homeostasis. Neurofibrillary tangles are aggregates of the hyperphosphorylated form of tau, a protein involved in the stabilization of axonal microtubules. Other histopathological markers of the AD brain are dysfunctional microglia, reactive astrocytes, and dystrophic neurites. The Aβ cascade hypothesis of AD assumes that the brain accumulation of Aβ represents the initial event of the pathological process and starts 15 to 20 years before clinical symptoms become apparent. Point mutations of the amyloid precursor protein (APP) and the enzymes involved in its processing (PSEN1 and PSEN2) alter the production of Aβ and cause the autosomal dominant familial forms of AD. A specific mutation of APP (A673T) was found to protect against AD onset and cognitive decline in cognitively healthy elderly individuals. The mutant amino acid is adjacent to the cleavage site of the β‐site amyloid precursor protein cleaving enzyme‐1 (BACE1) and results in about a 40% reduction in Aβ production in vitro. In late‐onset sporadic AD, accumulation of brain Aβ has been attributed to faulty clearance or increased BACE1 activity. Aβ accumulation has also been linked to the apolipoprotein E ε4 (APOE*ε4) allele, the most important genetic risk factor associated with sporadic AD. These observations represent the foundation of the amyloid hypothesis of AD and during the last 20 years intensive efforts have been made to identify compounds which antagonize the accumulation of Aβ in the AD brain. This objective was mainly pursued through two approaches. One was to reduce Aβ production by inhibiting the two key enzymes (BACE1 and γ‐secretase) which cleave APP to generate Aβ. The other approach was to enhance Aβ clearance from the brain with active or passive immunotherapy. Unfortunately, neither of these had therapeutic effects in patients with mild‐to‐moderate AD. 1 From these failures the AD scientific community concluded that the mild‐to‐moderate stage of AD is too late for the anti‐Aβ drugs to reverse or halt the progression of the disease. In addition, because about 25% of mildly affected patients enrolled in clinical trials did not have evidence of Aβ brain deposition, new AD diagnostic criteria were proposed to define dementia due to AD based on biomarker evidence of brain amyloidosis. This enabled the definition of preclinical stages of AD to allow early pharmacological intervention. 2 Nevertheless, two large Phase 3 studies in prodromal AD patients (CREAD 1 and 2) with crenezumab, a monoclonal antibody directed against oligomeric Aβ 3 and one large Phase 3 study (APECS) with verubecestat, 4 a potent BACE1 inhibitor, were prematurely terminated because they failed to show clinical efficacy. The results of the APECS study were fully published and were surprising because, although the levels of Aβ deposition in the brain and Aβ in the cerebrospinal fluid decreased, cognitive function and the structural brain imaging findings worsened with verubecestat compared to placebo. Furthermore, a Phase 3 trial with atabecestat, another potent BACE1 inhibitor, in cognitively normal subjects with biomarker evidence of brain Aβ deposition, was also interrupted because of accelerated cognitive deterioration in subjects receiving the drug. 5 Finally, two large studies of umibecestat (Generation 1 and 2), a BACE1 inhibitor, in cognitively normal subjects without evidence of Aβ brain deposition but carrying the APOE4 allele, a genetic risk factor for AD, were also prematurely interrupted because of worsening cognitive function. 6 The failure of all these early intervention trials needs to be explained and has led to questioning of the amyloid hypothesis of AD, providing fresh impetus to the exploration of alternative etiologies and therapeutic strategies. One promising approach is therapeutic plasma exchange (TPE), which aims to supplement beneficial factors contained in young plasma that may promote neuronal survival and function and/or remove senescent detrimental factors that accumulate during aging.
3. PERIPHERAL INFLAMMATION IN ALZHEIMER'S DISEASE
The role of neuroinflammation in the pathogenesis of AD is gaining much interest as an avenue for new therapeutic approaches, particularly in view of the failure of most Aβ‐targeting drugs. Alteration of peripheral immune activity can affect the brain immune system 7 and be associated with increased risk of dementia. 8 A long‐term longitudinal study of 1633 participants revealed a positive association between midlife peripheral inflammation and shrinkage of brain volume in late life. 9 A 6‐month study in 300 community‐dwelling subjects with mild to severe AD has shown that increases in serum tumor necrosis factor alpha (TNF‐α) levels were associated with increased rate of cognitive decline. 10 Circulating levels of peripheral cytokines have been shown to correlate to cytokine levels in the brain, AD severity, brain atrophy, 11 and cognitive performance. 12 High plasma levels of monocyte chemoattractant protein‐1 (MCP‐1) were found to be associated with AD severity and faster cognitive decline. 13 C‐reactive protein, a biomarker of low‐grade inflammation, was associated with shortened latency for AD onset in ApoE4 carriers. 14 Interestingly, longitudinal studies have found that associated peripheral inflammation may occur years before AD onset. 15
Longitudinal studies in cognitively healthy subjects have shown that high baseline plasma Aβ42 levels are associated with future increased risk of AD. 16 Low serum Aβ‐albumin complexes were associated with decreased levels of cerebrospinal fluid (CSF) Aβ42, increased levels of CSF phosphorylated‐tau, and higher AD prevalence. 17 These observations suggested that a decreased ability of serum albumin to bind Aβ in aging could slow the clearance of Aβ from the central nervous system (CNS) and increase inflammatory response in the brain. Although elevated serum Aβ levels and systemic inflammation markers are associated with neurodegeneration and AD onset, we do not know if there is a causal relationship and if lowering serum levels of Aβ or inflammatory markers from the blood may be effective in AD patients.
4. REJUVENATION APPROACHES IN ANIMAL MODELS OF ALZHEIMER'S DISEASE
The hypothesis that removal of toxic and senescent factors from blood and simultaneously supplementing “rejuvenating” elements may be beneficial in aging and in AD has been quite extensively tested in animals (Figure 1). Animal models of blood exchange used heterochronic parabiosis, a surgical procedure that joins the organs and circulatory systems of two animals of different ages. 18 Heterochronic parabiosis has been shown to stimulate neurogenesis and synaptic plasticity in the hippocampus 19 and improve cognitive function 20 of aged mice. These changes were correlated with increased cAMP response element‐binding protein (CREB) signalling, which is implicated in synaptic plasticity. Moreover, exposure of young animals to aged blood has led to a significant reduction in neurogenesis in the dentate gyrus of the hippocampus, effects mediated by increased levels of C‐C motif chemokine 11 (CCL‐11). 20 Conversely, parabiosis between transgenic AD and wild‐type mice determined deposition of Aβ in vessel walls and parenchyma, and formation of AD‐like protein aggregates in the brain of wild‐type mice, showing that blood‐derived Aβ can enter the CNS determining degenerative changes. 21
FIGURE 1.
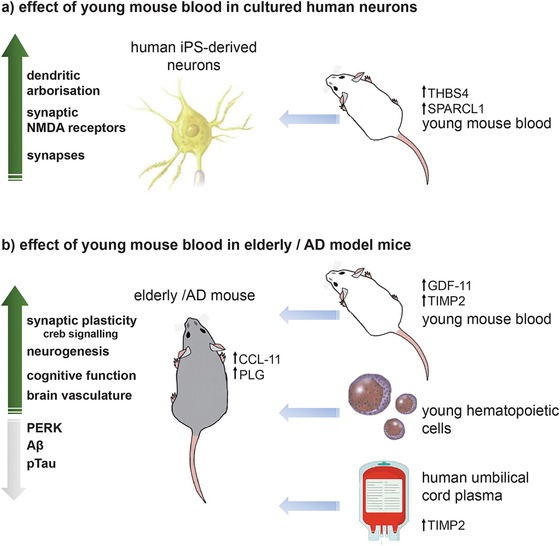
Overview of rejuvenating effects of blood exchange in preclinical studies. A, Young mouse blood factors thrombospondin‐4 and SPARC‐like protein 1 boosted neuronal function and N‐methyl‐D‐aspartate synaptic responses of human cultured iPS‐derived neurons, increasing dendrites and synapses formation. B, Young mouse blood enriched in growth differentiation factor 11 and tissue inhibitor of metalloproteinases 2 (TIMP2) enhanced cognitive function through cAMP response element‐binding protein signalling in aged mice, improved vascular brain function, increased neurogenesis, and decreased AD‐like pathology in transgenic animal models. Alzheimer's disease mice showed lowered brain abnormal phosphorylation of hippocampal extracellular signal regulated kinase, amyloid β burden, and tau phosphorylation. Treatment with young hematopoietic cells or administration of human umbilical cord plasma enriched in TIMP2, decreased aging related circulating factors CCL‐11, PLG, and improved cognition in old mice
Growth differentiation factor 11 (GDF‐11) was found in higher concentrations in young mouse serum and was considered responsible for remodelling of cerebral vasculature and enhancing neurogenesis in aged mice. 22 In aged human APP transgenic mice, exposure to young blood through parabiosis or intravenous plasma administration significantly rescued neuronal synaptophysin and calbindin levels, and attenuated cognitive deficit while amyloid plaque deposition remained unaffected. 23 Abnormal phosphorylation of hippocampal extracellular signal regulated kinase (ERK), a kinase linked to AD and neurodegeneration, dropped to wild‐type levels.
Peritoneal dialysis was found to decrease plasma Aβ levels in chronic kidney disease patients. 24 This technique has been used as an alternative to parabiosis in APP/PS1 transgenic mice and significantly attenuated brain Aβ burden, neuroinflammation, neurodegeneration, and cognitive deficits after a 1‐month treatment. 24 Peritoneal dialysis might enhance Aβ efflux from brain to blood, attenuating brain inflammation and improving Aβ phagocytosis by microglia and clearance of hyperphosphorylated‐tau.
Castellano et al. treated wild‐type aged mice with human umbilical cord plasma proteins and found enhanced hippocampal activity and improved cognitive function in spatial learning, memory, and fear‐conditioning testing. 25 The tissue inhibitor of metalloproteinases 2 (TIMP2), a blood‐borne factor, was found to be enriched in human cord plasma, young mouse plasma, and young mouse hippocampi. TIMP2 appeared in the brain after systemic administration and increased synaptic plasticity and hippocampus‐dependent cognition. 25
Cognitive function (specifically hippocampal memory) was improved in aged mice by replacement of old peripheral hematopoietic cells with young ones, in association with reduced synapse loss and reduced activation of microglia. 26 While previous parabiosis studies have attributed cognitive aging, at least in part, to reduced neurogenesis, Das et al. reported that restoration of neurogenesis is not essential for the preservation of cognitive function. Microglial rejuvenation, via peripheral manipulation of the hematopoietic system, may be sufficient to maintain or restore hippocampal function. 26 In a recent in vitro study focusing on the identification of specific young blood factors able to enhance cognitive function, young mouse serum induced human cultured neurons, boosted synapse formation and connectivity, and enhanced NMDA synaptic responses. 27 Thrombospondin‐4 (THBS4) and SPARC‐like protein 1 (SPARCL1), two proteins enriched in young blood, where found to mediate these effects. Recombinant THBS4 and SPARCL1 were able to increase dendritic arborization, double synapse numbers, and increase synaptic NMDA receptors in cultured neurons. 27 Although these observations might not necessarily translate to humans, multiple preclinical studies are suggesting that TPE might work in both aging alone and AD. It is still unclear how the plasma from young animals benefits the brain. Soluble factors in young plasma might interact with endothelial cells 22 targeting several anti‐aging pathways and/or lowering Aβ burden in the brain. A recent study found that intravenous injection of plasma collected from exercising (voluntarily running) mice into sedentary mice reduced baseline neuroinflammatory gene expression, suppressed lipopolysaccharide (LPS)‐induced brain inflammation and improved contextual learning and memory. 28 These beneficial effects appeared mediated by a marked increase in complement cascade inhibitors including clusterin. 28 Although no age difference effect was explored in this study, its findings do add support to the principle of plasma‐borne factors being able to affect cognition. Understanding which circulating plasma factors underlie the apparent restoration of age‐related cognitive function loss might lead to the development of new molecular targets for intervention.
5. THERAPEUTIC PLASMA EXCHANGE IN THE CLINICAL PRACTICE
Therapeutic plasma exchange is used to remove patient plasma and replace it with albumin or other colloids, fresh frozen plasma, and/or crystalloids while maintaining normal plasma volume and osmotic balance. The purpose is the elimination of circulating toxic substances such as autoantibodies, alloantibodies, immune complexes, proteins, and toxins. 29 During plasma exchange, blood from the patient is passed through an apheresis device (“apheresis” is derived from a Greek word meaning “removal”) which separates plasma from other blood components. This separation can be achieved either by centrifugal separation or by membrane filtration. Citrate anticoagulation is generally used with centrifugation devices, while heparin is used with membrane filtration. The removed plasma has to be replaced, usually volume for volume, with an appropriate fluid that is able to preserve intravascular oncotic pressure, thus maintaining systemic blood pressure. A colloid solution (eg, albumin and/or plasma) or a combination of crystalloid/colloid solution can be used. Typically, 30 to 40 mL/kg of plasma (1 to 1.5 plasma volumes) are removed at each procedure and replaced with isotonic 4.5% or 5.0% human albumin solution. Fresh frozen plasma is also used to replace clotting factors in patients at high risk of bleeding (such as those with Goodpasture syndrome and pulmonary hemorrhage) and is recommended in patients with thrombotic thrombocytopenic purpura. 30
Plasma exchange is widely used in the treatment of various pathologies, including Guillain‐Barré syndrome, 31 multiple sclerosis, 32 inflammatory demyelinating polyradiculoneuropathy, 33 acute inflammatory demyelinating disease of the CNS, 34 and other peripheral neurological conditions. 35 The American Society for Apheresis (ASFA) produces regularly updated, evidence‐based guidelines for TPE and Table 1 presents current first‐line indications. 36
TABLE 1.
Category I indications for therapeutic plasma exchange (first‐line therapy based on strong research evidence)
| Disease | Indication |
|---|---|
| Acute inflammatory demyelinating polyradiculoneuropathy Guillain‐Barre syndrome | Primary treatment |
| Antineutrophil cytoplasmic antibody‐associated rapidly progressive glomerulonephritis (granulomatosis with polyangiitis and microscopic polyangiitis) |
Dialysis dependence Diffuse alveolar haemorrhage |
| Anti‐glomerular basement membrane disease (Goodpasture's syndrome) |
Diffuse alveolar hemorrhage Dialysis independence |
| Chronic inflammatory demyelinating polyradiculoneuropathy | |
| Focal segmental glomerulosclerosis | Recurrent in transplanted kidney |
| Hyperviscosity in monoclonal gammopathies |
Symptomatic Prophylaxis for rituximab |
| Liver transplantation | Desensitization, ABO, living donor |
| Myasthenia gravis |
Moderate‐severe Pre‐thymectomy |
| N‐methyl d‐aspartate receptor antibody encephalitis | |
| Paraproteinemic demyelinating neuropathies/chronic acquired demyelinating polyneuropathies |
IgG/IgA IgM |
| Progressive multifocal leukoencephalopathy associated with natalizumab | |
| Renal transplantation, ABO compatible |
Antibody mediated rejection Desensitization, Living donor |
| Renal transplantation, ABO incompatible | Desensitization, living donor |
| Thrombotic microangiopathy, complement mediated | Factor H autoantibodies |
| Thrombotic microangiopathy, drug associated | Ticlopidine |
| Thrombotic thrombocytopenic purpura | |
| Wilson's disease, fulminant | Fulminant |
In addition to removing pathogenic substances, TPE may also remove normal plasma constituents, such as coagulation factors (which can cause transient changes in blood‐clotting factor levels, and prothrombin and activated partial thromboplastin times), immunoglobulins, and platelets. However, in patients with normal bone marrow and liver function, endogenous synthesis replaces most coagulation factors and platelets within 2 to 4 days. 37 Therapeutic plasma exchange can be associated with a variety of risks; some such as nausea, vomiting, fainting, and hypotension could be symptoms of citrate toxicity and associated hypocalcaemia or due to vagal stimulation. They are usually treated with oral or parenteral calcium supplementation or slowing the blood flow into the apheresis device. Other adverse effects include hematomas at venepuncture/line insertion sites, fluid overload or under‐replacement, and allergic or anaphylactic reactions. The insertion and care of central venous catheters is another important source of morbidity and mortality. Nevertheless, with current technologies, and in skilful hands, plasma exchange is a relatively safe procedure. 30
6. PLASMA REPLACEMENT APPROACHES IN PATIENTS WITH ALZHEIMER'S DISEASE
The aging brain shows increased levels of many lysosomal proteins and inflammatory cytokines, while neurons and glial cells show dysfunctional endosomes, lysosomes, and autophagosomes. Whether these abnormalities contribute to aging or are just epiphenomena is unclear. Manipulation of autophagy‐related genes in transgenic mice that overexpress APP or tau results in significant accumulation of these proteins or progression of AD. These observations indicate that aging and neurodegeneration are associated with a loss of proteostasis and it is likely that stabilization of protein homeostasis could benefit the aging brain. 38 The initial rationale for TPE in AD was that abnormal Aβ accumulation in the brain is a pathological event in the AD process. There is a dynamic equilibrium between brain and plasma Aβ levels and TPE could remove the excess of Aβ from the brain and provide clinical benefits. Initial studies tried to verify whether TPE could modify the concentration of Aβ in plasma and CSF; Table 2 summarizes the main clinical trials of different plasma replacement approaches in patients with AD.
TABLE 2.
Main clinical studies using therapeutic plasma exchange in Alzheimer's disease
| Compound | Sponsor | Study code and acronym | Subject population | Study design | Number of subjects | Treatment period and follow‐up |
|---|---|---|---|---|---|---|
| Plasma from young donors |
Stanford University Alkahest |
PLASMA |
Mild‐to‐moderate AD | Open label, placebo‐controlled, cross‐over | 18 |
4 weeks 14 weeks |
| Plasma albumin 5% |
Grifols Biologicals |
NA | Mild‐to‐moderate AD | Open label, uncontrolled | 7 |
3 weeks 52 weeks |
| Plasma albumin 5% |
Grifols Biologicals |
NCT00742417 | Mild‐to‐moderate AD | Double‐blind, sham treatment‐controlled | 42 |
21 weeks 44 weeks |
| Plasma albumin 5% albumin 20% immunoglobulin 5% |
Grifols Biologicals |
AMBAR |
Mild‐to‐moderate AD | Double‐blind, sham‐treatment‐controlled | 347 |
14 months 14 months |
| GRF6019 (plasma fraction) |
Alkahest Grifols Biologicals |
NCT03520998 | Mild‐to‐moderate AD | Double‐blind, dose‐controlled | 51 |
13 weeks 24 weeks |
| GRF6019 (plasma fraction) |
Alkahest Grifols Biologicals |
NCT03520998a | Severe AD | Double‐blind, placebo‐controlled | 20 |
5 days 9 weeks |
From ClinicalTrials.gov (https://clinicaltrials.gov/). Last accessed: September 9, 2019.
Recruiting, NA = not available.
Abbreviations: AD, Alzheimer's disease; AMBAR, Alzheimer's Management By Albumin Replacement
6.1. Plasma exchange with 5% albumin
Grifols (Barcelona, Spain) is developing plasma exchange therapies with human plasma enriched with human albumin (Albutein®) with or without human immunoglobulins (Flebogamma DIF®). The rationale for using albumin‐enriched plasma is that the vast majority of Aβ circulating in blood (around 90%) is bound to albumin in a 1:1 ratio. 39 In vitro studies showed that human albumin produced by Grifols (Albutein®) is able to bind Aβ peptide. 40 Initial pilot studies of TPE in AD patients were carried out with 5% human albumin. In a 6‐month, open label, uncontrolled pilot study, seven patients with mild‐to‐moderate AD underwent six plasma exchange infusions over 3 weeks. 41 During the 3‐week plasma exchange period there was a saw‐tooth fluctuation pattern in plasma Aβ40 and Aβ42 levels. Variations in mean CSF Aβ40 and Aβ42 concentrations were less clear. Mean Mini‐Mental State Examination (MMSE) and Alzheimer's Disease Assessment Scale‐Cog (ADAS‐Cog) scores remained quite stable,61 but this observation should be taken cautiously since there was no control group in this study.
A 21‐week, double‐blind, controlled study (NCT00742417) evaluated the safety, tolerability, and preliminary efficacy of TPE with 5% albumin in 42 mild‐to‐moderate AD patients. 42 Patients on TPE received two infusions/week for 3 weeks followed by one infusion/week for 6 weeks and, finally, one infusion every 2 weeks for an additional 12 weeks. The control group received sham infusions. Patients were followed up for 24 weeks after the treatment period. One patient in the control group and two patients in the TPE groups did not complete the full 21‐week treatment part of the study. Five additional patients in both groups did not complete the 24‐week follow‐up. Two patients in the control group (cholangitis and otitis media) and three in the plasma exchange group (hemorrhage associated with the catheter insertion, complex partial seizures, and fatal myocardial infarction) experienced serious adverse events. Eighteen patients in the TPE group (95%) and 14 patients in the control group (70%) reported adverse events (P < .05). More patients in the TPE group reported infections (56% vs 29%) and psychiatric symptoms (50% vs 36%) than did controls. There were no significant differences between treatment groups in Aβ1‐40 and Aβ1‐42 levels in CSF. Plasma Aβ1‐42 concentrations were significantly lower in the TPE‐treated group compared to controls while, paradoxically, plasma Aβ1‐40 levels tended to be higher. At week 21, patients undergoing plasma infusions performed significantly better than control patients on Boston Naming Test (P = .010) but worse on Neuropsychiatric Inventory (NPI) (P = .028) and Alzheimer's Disease Cooperative Study‐Activities of Daily Living (ADCS‐ADL) (P = .050). A possible explanation for these findings is that TPE had a negative impact on activities of daily living during the intensive treatment phases, while psychiatric symptoms may have been impacted by the patients having to tolerate a catheter inserted in their chests, and the discomfort caused by treatment‐related metabolic alterations. However, an increase in psychiatric symptoms has also been observed with other anti‐Aβ drugs, especially β‐secretase and γ‐secretase inhibitors, and has been linked to reductions of brain Aβ levels. 43 Conversely, infusions of young fresh frozen plasma in AD patients have been associated with improved activities of daily living and functionality. 44
A 14‐month, double‐blind, placebo‐controlled study (Alzheimer's Management By Albumin Replacement, AMBAR, NCT01561053) evaluated the effects of different plasma replacement levels of albumin (5% and 20%), with or without intravenous immunoglobulin (5%) in 347 mild‐to‐moderate AD patients. 45 The study was conducted at 41 sites in Spain and the United States. The intervention regime comprised a 6‐week intensive treatment stage with one infusion (2500 to 3000 mL) per week (TPE), followed by a 12‐month maintenance treatment stage with one infusion (100 to 200 mL) per month (low volume plasma exchange or LVPE). During the 6‐week TPE stage, patients were randomized to receive albumin 5% or sham plasma exchange (ratio 3:1). During the 12‐month LVPE stage, patients who received albumin 5% in the TPE phase, received one of three treatments: 20 g of albumin 20%, 20 g albumin 20% plus 10 g immunoglobulins 5%, or 40 g albumin 20% plus 20 g immunoglobulins 5%. Patients who received sham plasma exchange during the 6‐week intensive TPE continued to receive sham plasma infusions. The change from baseline to the end of maintenance treatment in the ADAS‐Cog and ADCS‐ADL scores were the coprimary efficacy variables. Secondary efficacy variables included change from baseline in scores on cognitive, functional, behavioral, and overall clinical performance. Changes in plasma and CSF Aβ and tau protein concentrations, structural and functional imaging changes in brain areas of interest were also measured. Results presented at Alzheimer conferences 46 reported that of the 347 randomized patients, only 322 started treatment and 72% of them completed the study (Table 3). The number of patients who did not complete the study were similar in control and low‐albumin groups (20.0% and 21.8%, respectively) but were higher in the TPE groups that included immunoglobulins (34.9% and 34.6%, respectively; Table 3). Similarly, the number of patients with serious adverse events were similar in control and in low albumin‐groups (10.1% and 10.3%, respectively), but were two numbers higher in the groups that received immunoglobulins (22.1% and 20.3%, respectively; Table 3). There were two deaths during the study, both in the low‐albumin+low‐immunoglobulin group (one suicide, other cause unstated). The most frequent complications in the TPE groups compared to controls were hypotension (21.8% vs 1.3%, respectively) and muscle pain (21.4% vs 6.3%). Regarding efficacy, while each of the three treatment groups showed arithmetically less decline on the ADAS‐Cog than the control group, the differences (1.7 to 2.1 points) were not statistically significant (Table 3). However, when the three treatment arms were combined the 66% lesser decline in the ADAS‐Cog compared to placebo approached statistical significance (P = .06). On the ADCS‐ADL, the treated groups performed insignificantly better than the control groups (2.8 to 4.7 points) but the pooled group declined 52% less than those on placebo (P = .03). A subgroup analysis based on MMSE severity at baseline found that the mild AD group (MMSE 22 to 26) did not decline over the study period, with or without treatment (Table 3). In the moderate AD group (MMSE 18 to 21), the placebo group (n = 26) showed a marked decline on both ADAS‐Cog (6.4 ± 1.3 points) and ADCS‐ADL (−14.1 ± 2.7 points) while in the TPE groups the decline was less on both measures (Table 3). When the three treatment groups were combined (n = 83) the mean decline on both ADAS‐Cog (2.6 ± 1.1 points, P = .05) and ADCS‐ADL (−5.5 ± 1.3 points, P = .002) was significantly less compared to the control group (Figure 2). At the AAIC 2019 conference, it was reported that the Clinical Dementia Rating–Sum of Boxes (CDR‐SB) and the Alzheimer's Disease Cooperative Study‐Clinical Global Impression of Change (ADCS‐CGIC) scales declined significantly less rapidly in the pooled TPE groups than in placebo‐treated patients. 47 In both conventional and low‐volume plasmapheresis groups, a saw‐tooth profile was observed for plasma Aβ levels. 47
TABLE 3.
Main baseline characteristics and main outcome measures of safety and efficacy of the AMBAR study
| Variable | Controls (n = 80) | Low albumin (n = 78) | Low albumin low immunoglobulin (n = 86) | High albumin high immunoglobulin (n = 78) |
|---|---|---|---|---|
| Males/females | 36/44 | 43/35 | 48/38 | 47/31 |
| Age (years) | 68.4 ± 0.9 (n = 80) | 68.5 ± 0.9 (n = 78) | 69.5 ± 0.8 (n = 86) | 69.5 ± 0.9 (n = 78) |
| Baseline MMSE | 21.7 ± 0.3 (n = 80) | 21.2 ± 0.3 (n = 78) | 22.1 ± 0.3 (n = 86) | 21.4 ± 0.3 (n = 78) |
| Patients not completing the study | 16/80 (20.0%) | 17/78 (21.8%) | 30/86 (34.9%) | 27/78 (34.6%) |
| Patients with serious adverse events | 8/79 (10.1%) | 8/78 (10.3%) | 19/86 (22.1%) | 16/79 (20.3%) |
| ADAS‐Cog change from baseline | 3.2 ± 1.0 (n = 64) | 1.5 ± 1.0 (n = 61) | 0.8 ± 1.1 (n = 57) | 0.8 ± 1.3 (n = 50) |
| Mild (MMSE 22‐26) | 0.6 ± 1.1 (n = 38) | −0.6 ± 1.1 (n = 25) | −0.3 ± 1.0 (n = 37) | −0.9 ± 1.5 (n = 23) |
| Moderate (MMSE 18‐21) | 6.4 ± 1.3 (n = 26) | 3.3 ± 1.5 (n = 36) | 1.9 ± 1.1 (n = 20) | 2.4 ± 2.0 (n = 27) |
| ADCS‐ADL change from baseline | −6.7 ± 1.5 (n = 64) | −3.9 ± 1.2 (n = 61) | −2.0 ± 1.0 (n = 57) | −3.5 ± 1.8 (n = 51) |
| Mild (MMSE 22‐26) | −1.3 ± 1.3 (n = 38) | −0.9 ± 1.4 (n = 25) | 0.8 ± 1.0 (n = 37) | −2.4 ± 1.7 (n = 23) |
| Moderate (MMSE 18‐21) | −14.1 ± 2.7 (n = 26) | −6.0 ± 1.8 (n = 36) | −5.7 ± 2.1 (n = 20) | −4.5 ± 3.0 (n = 28) |
From ClinicalTrials.gov (https://clinicaltrials.gov/). Last accessed: September 9, 2019.
Abbreviations: ADAS‐Cog, Alzheimer's Disease Assessment Scale‐Cognitive Subscale; ADCS‐ADL, Alzheimer's Disease Cooperative Study‐Activities of Daily Living; AMBAR, Alzheimer's Management By Albumin Replacement; MMSE, Mini‐Mental State Examination
FIGURE 2.
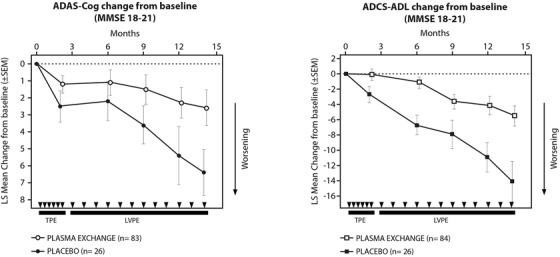
Mean change from baseline of the Alzheimer's Disease Assessment Scale‐Cognitive Subscale and Alzheimer's Disease Cooperative Study‐Activities of Daily Living of moderately affected patients of the Alzheimer's Management By Albumin Replacement study (modified from reference 75). LS = least square
6.2. Plasma infusion with young plasma
A 14‐week, double‐blind, placebo‐controlled, cross‐over study (PLASMA, NCT02256306) at Stanford University evaluated the safety and tolerability of infusions of young fresh frozen plasma (from donors of 18 to 30 years of age) in nine patients with mild‐to‐AD patients. 44 Infusions (250 mL) of plasma or placebo (saline) were given once a week for 4 consecutive weeks and treatments were separated by a wash‐out period of 6 weeks. A further group of nine AD patients received a 4‐week treatment with young fresh plasma in open‐label conditions. One patient in the open‐label, fresh plasma cohort discontinued treatment for urticaria during plasma infusion. Another patient in the cross‐over cohort discontinued participation because of an unrelated stroke that occurred during the end of the wash‐out period after placebo infusions. There were no related serious or severe adverse events. The most common adverse events in the plasma treatment group included hypertension (18%), dizziness (12%), sinus bradycardia (18%), headache (18%), and sinus tachycardia (18%) but the frequencies of these adverse events were not significantly different from those in the placebo cohort. Plasma infusion recipients demonstrated statistically significant improvements compared to placebo on functional measures (Functional Activities Questionnaire [FAQ] and Alzheimer's Disease Cooperative Study Activities of Daily Living Inventory in mild cognitive impairment [ADCS‐MCI‐ADL]) but not on cognitive (Alzheimer's Disease Assessment Scale‐Cog 13‐item version [ADAS‐Cog13]), behavioral (Neuropsychiatric Inventory‐Questionnaire [NPI‐Q]) or clinical global ( CDR‐SB) measures. However, P values were not corrected for multiple comparisons. In terms of functional brain imaging, functional magnetic resonance imaging (fMRI) analyses did not detect significant effects of plasma administration on the overall structure of 10 resting‐state networks. However, plasma administration produced a significantly mean lower z‐score inside the networks compared with the baseline.
6.3. Plasma infusion with plasma fractions
The rationale for using a plasma protein fraction is based on several factors. Although plasma is widely used, there are risks such as the potential transfer of pathogens, histo‐incompatibility, and allergic reactions to proteins such as clotting factors and immunoglobulins. Safer products have been developed by pooling plasma from multiple donations, fractionating the plasma into more defined products, and including additional processing steps to minimize the potential for pathogen transmission. The investigation of plasma fractions in AD is also supported by the theory that there are specific components of plasma that actually drive beneficial functions in aging.
GRF6019 is a human plasma protein fraction depleted of coagulation factors and gamma globulins and containing about 400 proteins believed essential to the beneficial effects of whole plasma. GRF6019 is being developed by Alkahest (San Carlos, California) in collaboration with Grifols (Barcelona, Spain). No data on GRF6019 have been fully published and all the information available is from conferences or company press releases. In animal models of human aging, GRF6019 was claimed to enhance neurogenesis, improve age‐related deficits in learning and memory, and reduce neuroinflammation. 48 Studies performed in aged mice at Alkahest compared intermittent dosing with plasma fractions (two to three times per week for up to 12 weeks) with pulsed dosing (daily infusion for 5 to 7 consecutive days). Pulsed dosing was found to be superior to intermittent dosing on behavioral and neurogenesis endpoints. Benefits after pulse dosing lasted up to 3 months, demonstrating that continuous dosing was not required in mice. 48 A 24‐week, dose‐range finding study (NCT03520998) evaluated the safety and tolerability of two intravenous dose regimens of GRF6019 (100 or 250 mL each day for 5 consecutive days administered at Week 1 and at Week 13) in 52 subjects with mild‐to‐moderate AD. 49 Forty subjects completed both dosing periods. The most common adverse events were mild headaches, infusion site reactions, transient lab abnormalities, and transient blood pressure changes. There were two serious adverse events; one was a hypersensitivity reaction assessed related to GRF6019, while the other was related to a history of deep venous thrombosis (a pre‐existing condition). Compared to baseline, subjects receiving GRF6019 had no decline in cognition, as measured by the 11‐item AD ADAS‐Cog11 and the MMSE, and negligible declines in function by the AD Cooperative Study Activities of Daily Living scale 23‐item version (ADCS‐ADL23), and the CDR‐SB score. A 9‐week, double‐blind, placebo‐controlled Phase 2 study (NCT03765762) is currently ongoing with the aim of evaluating the safety and tolerability of short‐term treatment with intravenous GRF6019 (250 mL each day for 5 consecutive days) in 20 patients with severe AD (MMSE score between 0 and 10 at baseline). The study is still recruiting patients. Alkahest, and its collaborator Grifols, expect to announce results during the second half of 2020. This is a singular study because patients at more advanced stages of AD are rarely included in clinical trials, and this novel approach could provide a novel treatment option for these individuals. A Phase 3 trial is being planned.
7. CLINICAL PERSPECTIVES
Plasma replacement studies in transgenic mouse models of AD suggest that factors present in the circulatory system can either worsen or attenuate brain pathological hallmarks and cognitive performance. 38 However, observations in mouse models of AD do not necessarily translate to humans, particularly because the models used miss some critical aspects of the disease (such as neurofibrillary tangle formation and neuronal death), and there has been no systematic work to optimize the experimental conditions of TPE (duration of heterochronic parabiosis, frequency, duration, and volume of plasma administration). Nevertheless, these studies are important because they provide the first demonstration that plasma exchange has potential therapeutic effects.
Initial clinical results obtained with TPE in AD patients are encouraging but we must point out that there are several methodological limitations that could undermine the results and their applicability to larger AD groups. Limited sample size of the available studies may have impacted the homogeneity of treatment groups at baseline, favoring (by chance) specific treatment arms. This is true also for the AMBAR study that randomized a more consistent group of patients (n = 347) but adopted a complicated study design involving four treatment groups and two study phases. In addition, AD patients enrolled in TPE studies may not be representative of general AD population because of several adopted exclusion criteria (such as abnormal coagulation parameters, hypohemoglobinemia, bradycardia, increased risk of allergic reactions). Most importantly, it should be noted that these initial studies, including the AMBAR trial, did not require biomarker‐proven brain Aβ deposition (either by Aβ‐PET or CSF Aβ42 levels) at entry. In the AMBAR study, 28% of screened patients did not show evidence of Aβ brain deposition, meaning that these patients had an underlying reason for their dementia other than AD. Additional analysis should be conducted in this subgroup of patients to verify if their response to TPE was similar to patients with biomarker evidence of brain Aβ deposition. Another important question regards protection of the study blind and the appropriateness of control groups. It is unclear if sham plasma exchange procedures adequately maintain blindness because they use lower volumes than the real procedure and it is known that plasmapheresis triggers a consistent physiological response, including a lowering of body temperature. Future studies should consider all the above described limitations; should be of adequate length (12 to 18 months); and, most importantly, better preserve the blind.
An important question is whether Aβ clearance is the mechanism through which TPE has produced initial positive cognitive and functional effects in AD patients. It could be that positive effects are due to the removal of detrimental elements present in the plasma of the AD patients (eg, β2‐microglobulin and/or eotaxin) or the supplementation of beneficial elements present in the plasma of young donors (eg, growth differentiation factor 11, granulocyte‐macrophage colony‐stimulating factor, growth hormone releasing hormone, osteocalcin, oxytocin or tissue inhibitors of metalloproteinases 2, clusterin). It is still unclear how young plasma or plasma enriched with albumin may exert an effect. Beneficial proteins or neuroprotective factors may enter the brain through the blood–brain barrier and/or at sites lacking a functional barrier, and/or may interact with endothelial cells to modulate neurovascular functions. Alternatively, inflammatory mediators, antibodies, reactive oxygen species or senescent factors, or pathological microorganisms present in the plasma of the AD patient may be removed during the exchange process (Figure 3). So far, few studies have investigated in humans or in animal models the effect of the systemic administration of selected plasma components. Future studies need to clarify mechanisms for any beneficial effects of TPE to better define its therapeutic potential.
FIGURE 3.
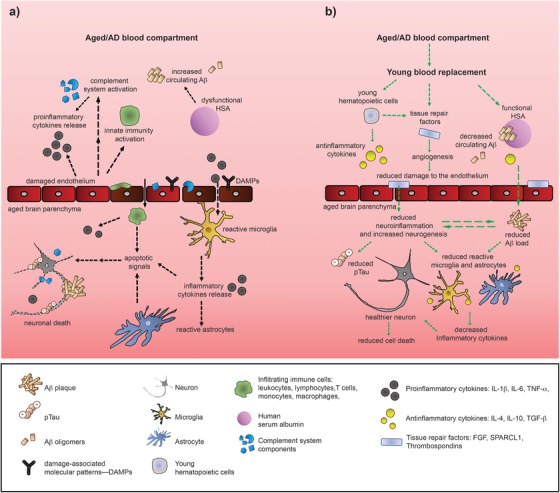
Benefits of young plasma: working hypothesis. A, Amyloid plaques and tau tangles in the Alzheimer's disease (AD) brain induce neuronal synapse loss and apoptosis. Activated microglia responsible for the clearance of cellular debris activate the innate and adaptive immune systems releasing inflammatory cytokines. Protracted glial‐mediated inflammation damages brain endothelial cells, exposing damage‐associated molecular pattern signals that overstimulate the peripheral immune response, activating complement and inducing a persistent inflammatory state, as well as decreasing amyloid β (Aβ) clearance by dysfunctional albumin. These effects contribute to cognitive deficits and neuronal death. B, Replacement of old plasma with young plasma exposes the AD‐damaged brain endothelium to protective factors like SPARC‐like protein 1, tissue inhibitor of metalloproteinases 2, and thrombospondin‐4, that might lead to beneficial effects such as increased neurogenesis, angiogenesis, and activation of antiapoptotic pathways. Young hematopoietic cells may decrease circulating proinflammatory molecules, induce anti‐inflammatory cytokines, and increase functional albumin (thus increasing Aβ clearance). Reduced Aβ and attenuated central and peripheral inflammation might improve cognition, enhance hippocampal function, and increase neuronal survival
Although TPE is safely used in some neurologic diseases, 50 clinical complications are described and should be expected. 51 Therapeutic plasma exchange in AD patients has to be considered with additional caution because the elderly subjects involved will be particularly sensitive to complications. Common risks include acute lung injury, circulatory overload, and allergic and/or anaphylactic reactions. Less common risks include transmission of infections, febrile nonhemolytic transfusion reactions, red blood cell alloimmunization, and hemolytic transfusion reactions. 50 Although the majority of these adverse effects are not lethal and are adequately managed in clinical practice, if TPE can be effective in AD patients it will be important to identify the key factors responsible, as they might lead to the development of molecule interventions with a better efficacy/risk profile.
8. CONCLUSIONS
Initial clinical studies with TPE using young plasma or young plasma enriched with albumin and/or immunoglobulin or selected plasma fractions have raised hopes for the management of both mild‐to‐moderate and severe AD patients. This is because clinical studies with TPE have been conducted in patients with established AD, a group of patients that has during the last 5 to 10 years been excluded from experimental trials with potential disease‐modifying drugs while the candidates that had already failed in established disease were tested in subjects with prodromal AD or even cognitively normal subjects at risk of developing AD. Thus, effective therapies in patients with frank AD are much needed. While initial results are encouraging, they are from small pilot studies that suffer methodological limitations such as a lack of real control groups and double‐blind conditions. In addition, the higher frequency of drop‐out in patients undergoing TPE compared to controls, may have led to overestimation of the beneficial effects; it is well known that in controlled AD trials discontinuing patients are generally those with the worst cognitive and functional performance and concomitant morbidity. Larger, longer, and fully blinded studies in AD patients with biomarker‐confirmed brain Aβ pathology are needed in the future to confirm the real clinical potential of TPE in AD. The issues of potential adverse effects and medical feasibility of chronic TPE in the particularly sensitive patient population represented by elderly people with established dementia need to be carefully considered.
CONFLICTS OF INTEREST
Bruno P. Imbimbo (PhD) is an employee at Chiesi Farmaceutici. He is listed among the inventors of a number of Chiesi Farmaceutici's patents of anti‐Alzheimer drugs. Stefania Ippati (PhD), Ferdinando Ceravolo (MD), and Mark Watling (MD) have no conflict of interest to declare.
ACKNOWLEDGMENT
This research did not receive funding or grants.
Imbimbo BP, Ippati S, Ceravolo F, Watling M. Perspective: Is therapeutic plasma exchange a viable option for treating Alzheimer's disease?. Alzheimer's Dement. 2020;6:e12004 10.1002/trc2.12004
REFERENCES
- 1. Panza F, Lozupone M, Logroscino G, Imbimbo BP. A critical appraisal of amyloid‐β‐targeting therapies for Alzheimer disease. Nat Rev Neurol. 2019;15:73‐88. [DOI] [PubMed] [Google Scholar]
- 2. Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer's disease: recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:280‐292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Yang T, Dang Y, Ostaszewski B, et al. Target Engagement in an Alzheimer Trial: crenezumab Lowers Aβ Oligomers in CSF. Ann Neurol. 2019;86:215‐224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Egan MF, Kost J, Voss T, et al. Randomized trial of verubecestat for prodromal Alzheimer's disease. N Engl J Med 2019;380:1408‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Henley D, Raghavan N, Sperling R, Aisen P, Raman R, Romano G. Preliminary results of a trial of atabecestat in preclinical Alzheimer's disease. N Engl J Med. 2019;380:1483‐1485. [DOI] [PubMed] [Google Scholar]
- 6. Shugart J, Strobel G. Cognitive Decline Trips Up API Trials of BACE Inhibitor. Alzheimer Research Forum. July 12. 2019. [Google Scholar]
- 7. Cao W, Zheng H. Peripheral immune system in aging and Alzheimer's disease. Mol Neurodegener. 2018;13:51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Dunn N, Mullee M, Perry VH, Holmes C. Association between Dementia and Infectious Disease: evidence from a Case‐Control Study. Alzheimer Dis Assoc Disord. 2005;19:91‐94. [DOI] [PubMed] [Google Scholar]
- 9. Walker KA, Hoogeveen RC, Folsom AR, et al. Midlife systemic inflammation is associated with late‐life brain volume. Neurology. 2017;89:2262‐2270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Holmes C, Cunningham C, Zotova E, et al. Systemic inflammation and disease progression in Alzheimer disease. Neurology. 2009;73:768‐774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Leung R, Proitsi P, Simmons A, et al. Inflammatory proteins in plasma are associated with severity of Alzheimer's disease. PloS One. 2013;8:e64971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Banks WA, Farr SA, Morley JE. Entry of blood‐borne cytokines into the central nervous system: effects on cognitive processes. Neuroimmunomodulation. 2002‐2003;10:319‐327. [DOI] [PubMed] [Google Scholar]
- 13. Lee WJ, Liao YC, Wang YF, Lin IF, Wang S, Fuh JL. Plasma MCP‐1 and cognitive decline in patients with Alzheimer's disease and Mild Cognitive Impairment: a two‐year follow‐up study. Sci Rep. 2018;8:1280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Engelhart MJ, Geerlings MI, Meijer J, et al. (2004) Inflammatory proteins in plasma and the risk of dementia: the Rotterdam Study. Arch Neurol. 2004;61:668‐672. [DOI] [PubMed] [Google Scholar]
- 15. Tao Q, Ang TFA, DeCarli C, et al. Association of chronic low‐grade inflammation with risk of Alzheimer disease in ApoE4 carriers. JAMA Network Open. 2018;1:e183597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Graff‐Radford NR, Crook JE, Lucas J, et al. Association of low plasma Aβ42/Aβ40 ratios with increased imminent risk for Mild Cognitive Impairment and Alzheimer disease. Arch Neurol. 2007;64:354‐362. [DOI] [PubMed] [Google Scholar]
- 17. Yamamoto K, Shimada H, Koh H, Ataka S, Miki T. Serum levels of albumin‐amyloid β complexes are decreased in Alzheimer's disease. Geriatr Gerontol Int. 2014;14:716‐723. [DOI] [PubMed] [Google Scholar]
- 18. Conboy MJ, Conboy IM, Rando TA. Heterochronic parabiosis: historical perspective and methodological considerations for studies of aging and longevity. Aging Cell. 2013;12:525‐530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Villeda SA, Luo J, Mosher KI, et al. The ageing systemic milieu negatively regulates neurogenesis and cognitive function. Nature. 2011;477:90‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Villeda SA, Plambeck KE, Middeldorp J, et al. Young blood reverses age‐related impairments in cognitive function and synaptic plasticity in mice. Nat Med. 2014;20:659‐663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Bu XL, Xiang Y, Jin WS, et al. Blood‐derived amyloid‐β protein induces Alzheimer's disease pathologies. Mol Psychiatry. 2018;23:1948‐1956. [DOI] [PubMed] [Google Scholar]
- 22. Katsimpardi L, Litterman NK, Schein PA, et al. Vascular and neurogenic rejuvenation of the aging mouse brain by young systemic factors. Science. 2014;344:630‐634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Middeldorp J, Lehallier B, Villeda SA, et al. Preclinical assessment of young blood plasma for Alzheimer disease. JAMA Neurol. 2016;73:1325‐1333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Jin WS, Shen LL, Bu XL, et al. Peritoneal dialysis reduces amyloid‐β plasma levels in humans and attenuates Alzheimer‐associated phenotypes in an APP/PS1 mouse model. Acta Neuropathol. 2017;134:207‐220. [DOI] [PubMed] [Google Scholar]
- 25. Castellano JM, Mosher KI, Abbey RJ, et al. Human umbilical cord plasma proteins revitalize hippocampal function in aged mice. Nature. 2017;544:488‐492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Das MM, Godoy M, Chen S, et al. Young bone marrow transplantation preserves learning and memory in old mice. Commun Biol. 2019;2:73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gan KJ, Südhof TC. Specific factors in blood from young but not old mice directly promote synapse formation and NMDA‐receptor recruitment. Proc Natl Acad Sci U S A. 2019;116:12524‐12533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. De Miguel Z, Betley MJ, Willoughby D, et al. Exercise conditioned plasma dampens inflammation via clusterin and boosts memory. bioRxiv. 2019. Sep. Sep 19. [Google Scholar]
- 29. Reeves HM, Winters JL. The mechanisms of action of plasma exchange. Br J Haematol. 2014;164:342‐351. [DOI] [PubMed] [Google Scholar]
- 30. El‐Ghariani K, Unsworth DJ. Therapeutic apheresis–plasmapheresis. Clin Med. 2006;6:343‐347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Chevret S, Hughes RA, Annane D. Plasma exchange for Guillain‐Barré syndrome. Cochrane Database Syst Rev. 2017;2:CD001798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Trebst C, Reising A, Kielstein JT, Hafer C, Stangel M. Plasma exchange therapy in steroid‐unresponsive relapses in patients with multiple sclerosis. Blood Purif. 2009;28:108‐115. [DOI] [PubMed] [Google Scholar]
- 33. Mehndiratta MM, Hughes RA, Pritchard J. Plasma exchange for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database Syst Rev. 2015;8:CD003906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Llufriu S, Castillo J, Blanco Y, et al. Plasma exchange for acute attacks of CNS demyelination: predictors of improvement at 6 months. Neurology. 2009;73:949‐953. [DOI] [PubMed] [Google Scholar]
- 35. Codron P, Cousin M, Subra JF, et al. Therapeutic plasma exchange in chronic dysimmune peripheral neuropathies: a 10‐year retrospective study. J Clin Apher. 2017;32:413‐422. [DOI] [PubMed] [Google Scholar]
- 36. Schwartz J, Padmanabhan A, Aqui N, et al. Guidelines on the use of therapeutic apheresis in clinical practice‐evidence‐based approach from the writing committee of the American Society for Apheresis: the seventh special issue. J Clin Apher. 2016;31:149‐162. [DOI] [PubMed] [Google Scholar]
- 37. Linenberger ML, Price TH. Use of cellular and plasma apheresis in the critically ill patient: part 1: technical and physiological considerations. J Intensive Care Med. 2005;20:18‐27. [DOI] [PubMed] [Google Scholar]
- 38. Wyss‐Coray T. Ageing, neurodegeneration and brain rejuvenation. Nature. 2016;539:180‐186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Biere AL, Ostaszewski B, Stimson ER, Hyman BT, Maggio JE, Selkoe DJ. Amyloid β‐peptide is transported on lipoproteins and albumin in human plasma. J Biol Chem. 1996;271:32916‐32922. [DOI] [PubMed] [Google Scholar]
- 40. Costa M, Ortiz AM, Jorquera JI. Therapeutic albumin binding to remove amyloid‐β. J Alzheimers Dis. 2012;29:159‐170. [DOI] [PubMed] [Google Scholar]
- 41. Boada M, Ortiz P, Anaya F, et al. Amyloid‐targeted therapeutics in Alzheimer's disease: use of human albumin in plasma exchange as a novel approach for Aβ mobilization. Drug News Perspect. 2009;22:325‐339. [DOI] [PubMed] [Google Scholar]
- 42. Boada M, Anaya F, Ortiz P, et al. Efficacy and safety of plasma exchange with 5% albumin to modify cerebrospinal fluid and plasma amyloid‐β concentrations and cognition outcomes in Alzheimer's disease patients: a multicenter, randomized, controlled clinical trial. J Alzheimers Dis. 2017;56:129‐143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Panza F, Lozupone M, Bellomo A, Imbimbo BP. Do anti‐amyloid‐β drugs affect neuropsychiatric status in Alzheimer's disease patients?. Ageing Res Rev. 2019;55:100948. [DOI] [PubMed] [Google Scholar]
- 44. Sha SJ, Deutsch GK, Tian L, et al. Safety, tolerability, and feasibility of young plasma infusion in the Plasma for Alzheimer Symptom Amelioration Study: a randomized clinical trial. JAMA Neurol. 2019;76:35‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Boada M, López O, Núñez L, et al. Plasma exchange for Alzheimer's disease Management by Albumin Replacement (AMBAR) trial: study design and progress. Alzheimers Dement. 2019;5:61‐69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Lopez OL. AMBAR (Alzheimer's Management By Albumin Replacement) phase IIb/III results. J Prevent Alzheimers Dis. 2018;5(suppl 1):S8. [Google Scholar]
- 47. Pick B. Grifols presents additional encouraging Alzheimer's trial results at AAIC. Grifols Press Release. 2019. July 16. [Google Scholar]
- 48. Hannestad J, Gallager I, Koborsi K, et al. Rationale and design of a prospective, randomized, double‐blind, dose‐comparison safety and tolerability study of GRF6019 in mild‐to‐moderate Alzheimer's disease. J Prevent Alzheimers Dis. 2018;5(suppl 1):S20‐1. [Google Scholar]
- 49. Hannestad J, Pederson T, Chao W, et al. OC35: a Phase 2 trial of GRF6019 in mild‐to‐moderate Alzheimer's disease. J Prevent Alzheimers Dis. 2019;6(suppl 1):S29. [Google Scholar]
- 50. Cortese I, Cornblath DR. Therapeutic plasma exchange in neurology: 2012. J Clin Apher. 2013;28:16‐19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Mortzell Henriksson M, Newman E, Witt V, et al. Adverse events in apheresis: an update of the WAA registry data. Transfus Apher Sci. 2016;54:2‐15. [DOI] [PubMed] [Google Scholar]