
FIGURE 11.
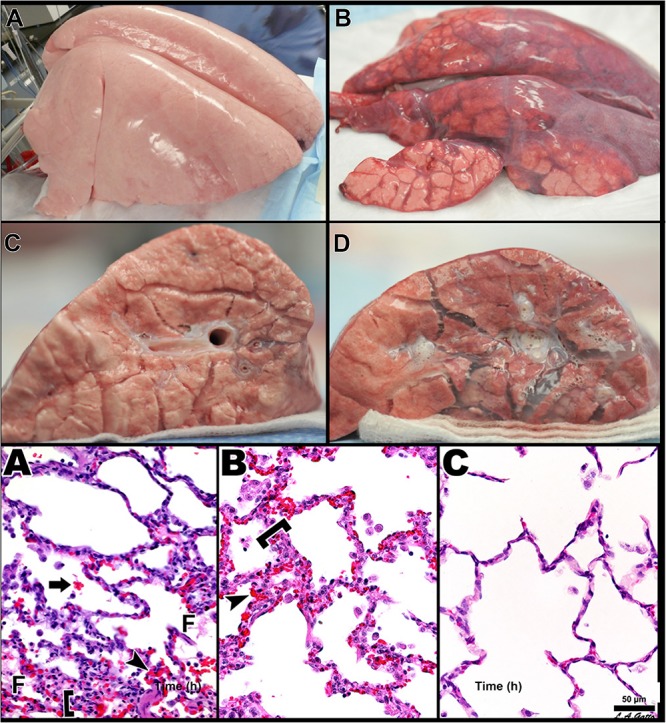
Three groups of pigs were ventilated for 48 h with a clinically applicable, high-fidelity porcine peritoneal sepsis (PS) and gut ischemia/reperfusion (I/R) acute respiratory distress syndrome (ARDS) model: (1) Control group without PS + I/R injury ventilated with a tidal volume (Vt) of 10 cc/kg and a positive end-expiratory pressure (PEEP) of 5 cm H2O. (2) ARDSnet group using a low-Vt ventilation method, applied following PS + I/R injury at the time point at which the animal reached the oxygen saturation limit listed in the ARDSnet protocol, with PEEP and FiO2 adjusted by oxygenation (Acute Respiratory Distress Syndrome Network, 2000). (3) Time-controlled adaptive ventilation (TCAV) method using the airway pressure release ventilation (APRV) mode applied immediately after PS + I/R injury (Habashi, 2005; Jain et al., 2016). Upper – Gross lung photographs after 48 h of ventilation following PS + I/R injury at necropsy (Control not shown). In the TCAV group (A,B), lungs inflated fully to near total lung capacity at 25 cm H2O without any gross atelectasis. The cut surface of the diaphragmatic lobe also showed no interstitial or airway edema and no atelectasis. Lungs in the ARDSnet group (C,D) also inflated to 25 cm H2O showed low lung volume with heterogeneous collapse and atelectasis and were wet and “boggy.” The cut surface showed both interstitial and airway edema. Lower – Photomicrographs of representative lung sections of specimens from the Control (A), ARDSnet (B), and TCAV (C) groups each at 40× magnification. F, fibrinous deposit in the air compartment; arrow, blood in alveolus; arrowhead, congested alveolar capillary; bracket, thickened alveolar wall. (A) Control: animals received 48 h of mechanical ventilation without PS + I/R injury. Specimen shows typical early acute lung injury pathology including fibrinous deposits, blood in alveolus, congested capillaries, and thickened alveolar walls. (B) ARDSnet: animals received PS + I/R injury, and LVt ventilation was applied after the onset of acute lung injury (i.e., PaO2/FiO2 ratio <300). Specimen shows typical advanced acute lung injury pathology including fibrinous deposits, blood in alveolus, congested capillaries, leukocyte infiltration, and thickened alveolar walls. (C) TCAV: specimen shows normal pulmonary architecture, alveoli are well-expanded and thin walled, and there are no exudates (Roy S. et al., 2013). Permissions obtained from Wolters Kluwer Health, Inc. License 4699411460832.