
FIGURE 2.
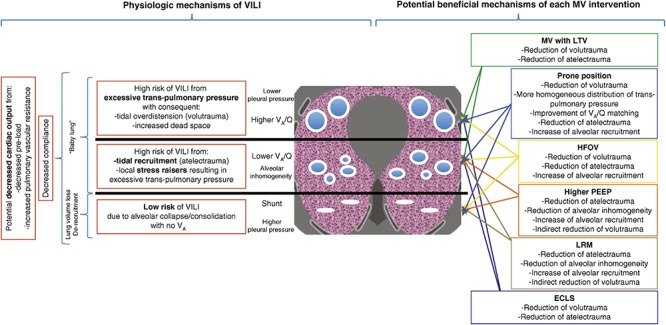
Gravity dependent three-compartment model of acute respiratory distress syndrome (ARDS) pathology: Left – Physiological mechanisms of ventilator-induced lung injury (VILI) and Right – Potential beneficial mechanisms of various protective ventilation strategies to minimize VILI. Open alveoli are shown as blue circles similar in size (top), unstable alveoli as smaller circles of various sizes (middle), and collapsed alveoli as solid white lines (bottom). The ARDSnet low tidal volume (LVt) method is designed to protect compliant open alveoli in the non-dependent lung and rest the collapsed tissue in the dependent portion of the lung by keeping it unventilated. Positive end-expiratory pressure (PEEP) is added in an attempt to stabilize the alveoli in between (Acute Respiratory Distress Syndrome Network, 2000). High-frequency oscillatory ventilation (HFOV) and lung recruitment maneuvers (LRMs) have been shown ineffective in reducing ARDS mortality (Brower et al., 2004; Meade et al., 2008; Mercat et al., 2008; Ferguson et al., 2013; Young et al., 2013; Cavalcanti et al., 2017; Hodgson et al., 2019). Prone position has been shown effective at reducing mortality (Guerin et al., 2013) by a mechanism of reducing regional alveolar strain and inflammation (Motta-Ribeiro et al., 2018; Xin et al., 2018). VILI, ventilator-induced lung injury; MV, mechanical ventilation; LTV, low tidal volume and inspiratory pressure; PEEP, positive end-expiratory pressure; ECLS, extracorporeal life support; HFOV, high-frequency oscillatory ventilation; LRM, lung recruitment maneuver; Q, perfusion; VA, alveolar ventilation; VA/Q, ventilation/perfusion ratio; baby lung, functional residual capacity (FRC) (Del Sorbo et al., 2017). Permissions to publish obtained from ATS.