

Gaps and transitions (disruptions) in perinatal insurance coverage disproportionately affect indigenous, Hispanic, and black non-Hispanic women.
OBJECTIVE:
To measure the association between race–ethnicity and insurance status at preconception, delivery, and postpartum and the frequency of insurance gaps and transitions (disruptions) across these time points.
METHODS:
We conducted a cross-sectional analysis of survey data from 107,921 women in 40 states participating in the Centers for Disease Control and Prevention's Pregnancy Risk Assessment and Monitoring System from 2015 to 2017. We calculated unadjusted estimates of insurance status at preconception, delivery, and postpartum and continuity across these time points for seven racial–ethnic categories (white non-Hispanic, black non-Hispanic, indigenous, Asian or Pacific Islander, Hispanic Spanish-speaking, Hispanic English-speaking, and mixed race or other). We also examined unadjusted estimates of uninsurance at each perinatal time period by state of residence. We calculated adjusted differences in the predicted probability of uninsurance at preconception, delivery, and postpartum using logistic regression models with interaction terms for race–ethnicity and income.
RESULTS:
For each perinatal time point, all categories of racial–ethnic minority women experienced higher rates of uninsurance than white non-Hispanic women. From preconception to postpartum, 75.3% (95% CI 74.7–75.8) of white non-Hispanic women had continuous insurance compared with 55.4% of black non-Hispanic women (95% CI 54.2–56.6), 49.9% of indigenous women (95% CI 46.8–53.0) and 20.5% of Hispanic Spanish-speaking women (95% CI 18.9–22.2). In adjusted models, lower-income Hispanic women and indigenous women had a significantly higher predicted probability of uninsurance in the preconception and postpartum period compared with white non-Hispanic women.
CONCLUSION:
Disruptions in perinatal insurance coverage disproportionately affect indigenous, Hispanic, and black non-Hispanic women. Differential insurance coverage may have important implications for racial–ethnic disparities in access to perinatal care and maternal–infant health.
Racial and ethnic disparities in maternal health outcomes are a national public health crisis.1 Black non-Hispanic and indigenous women face greater risk of maternal morbidity2 and are two to four times more likely to die from pregnancy-related causes compared with white non-Hispanic women1; some groups of Asian and Hispanic women also face higher risks of maternal morbidity and mortality.2,3
In a recent report, the Centers for Disease Control and Prevention (CDC) identified lack of access to quality care as a key contributor to pregnancy-related deaths.4 Health insurance enrollment is a prerequisite for access to quality health care before, during, and after pregnancy.5 Limited evidence on racial–ethnic differences in perinatal insurance status suggests that significant disparities exist. In 2016, 7% of Hispanic women were uninsured at birth compared with only 3.5% of white women.6 There are also racial–ethnic differences in the type of coverage that pregnant women hold at delivery: a higher proportion of births to white women were paid by private insurance (63.3%) compared with black women (27.7%), indigenous women (19.7%) and Hispanic women (28.4%) in 2016.6 Finally, there is also evidence of racial–ethnic differences in perinatal insurance continuity: an analysis of data from 29 states in 2009 found that black non-Hispanic, Hispanic, and indigenous women were more likely to report unstable coverage from preconception to delivery.7
The objective of this cross-sectional analysis was to investigate the association between maternal race–ethnicity and insurance status before, during, and after pregnancy and the frequency of insurance disruptions across these time points.
METHODS
We used PRAMS (the Pregnancy Risk Surveillance and Monitoring System) survey data collected in 40 states and New York City from 2015 to 2017. The CDC Division of Reproductive Health administers PRAMS in collaboration with state health departments.8 From birth certificate data, participating states select a sample representative of all women who delivered a liveborn neonate. The survey collects data using a standardized mail and telephone survey of recently postpartum women, including demographic characteristics, insurance status, health care utilization, and health outcomes before, during, and after pregnancy. As in prior studies, we limited our sample to respondents with complete insurance information (93.9% of the total sample).7,9
We used PRAMS data to classify insurance status at three time points: 1) preconception, measured as insurance held in the month before conception; 2) delivery, measured as the primary payer for the childbirth episode; and 3) postpartum, measured as insurance held at the time of the postpartum survey. Nearly all women (97.1%) completed the survey 3 or more months after childbirth. Preconception and postpartum insurance variables were self-reported. For 88.9% of women, we coded delivery insurance as the primary payer for childbirth recorded by the delivery institution (eg, hospital) on the birth certificate. For the remaining 12.0% of women without payment information from the birth certificate, we used self-reported delivery insurance. For all women in the sample with both birth certificate and self-reported responses for delivery, 88.3% had concordant responses.
We followed methods that the CDC previously used to hierarchically characterize insurance coverage at each time point into one of three categories: Medicaid, private, or uninsured.7 The Medicaid category included women who reported enrollment in Medicaid or a state-named Medicaid program. The private category included women who reported private insurance alone or in combination with Medicaid and women who reported TRICARE or other military insurance. The uninsured category included women who reported no insurance. Consistent with the U.S. Census,10 other national surveys,11 and previous analyses of the PRAMS,7 women who reported only Indian Health Service (IHS) were also classified as uninsured. This is because the IHS provides a system of health care delivery, largely primary care, not health insurance.10 The only exception was Alaska, where the IHS response option on the PRAMS included other state-specific programs, and thus was classified as Medicaid.7
We also generated four measures of insurance continuity between each time point: 1) continuous insurance, defined as insured with no change in insurance status; 2) private–Medicaid discontinuity, defined as moving between Medicaid and private coverage; 3) uninsurance discontinuity, defined as moving between any type of insurance and uninsurance; and 4) continuous uninsurance, defined as being without insurance with no change in insurance status.
The PRAMS survey data include maternal race–ethnicity information from the birth certificate. These self-reported variables are collected using a maternal worksheet and entered into the birth certificate application by the delivery facility. PRAMS does not include information on maternal place of birth or immigration status; however, recent commentary has suggested that perinatal outcomes for Hispanic women should be reported separately by country of origin to account for the growing disparity in birth outcomes for U.S.-born and non–U.S.-born Hispanic women.12,13 Further, studies of uninsurance among reproductive-aged women have found that nearly 1 in 3 noncitizen women are uninsured, compared with 9% of U.S.-born citizens.14 Thus, we used primary language (English or Spanish) as a proxy for country of origin for Hispanic women. Language is one of the most frequently used, and strongest predictors of, acculturation,15 and has been used as a proxy for nativity or acculturation in other studies of health disparities among Hispanic populations in the United States.16 This resulted in seven distinct race–ethnicity categories: white non-Hispanic; black non-Hispanic; Hispanic Spanish-speaking; Hispanic English-speaking; indigenous (American Indian or Alaskan Native), Asian and Pacific Islander; and a composite of missing, unknown, or mixed race.
We calculated the unadjusted, weighted proportion of women with each insurance category for each perinatal time point, as well as the proportion of women within each category of insurance continuity from preconception to postpartum. We also examined unadjusted estimates of uninsurance for each time point by state of residence. We stratified all descriptive statistics by race–ethnicity.
We used multivariable logistic regression models to estimate the association between uninsurance at each time point and race–ethnicity, adjusting for age, education, marital status, state of residence, and household income as a percentage of the federal poverty level. An interaction between household income and race–ethnicity was also included as racial–ethnic disparities in insurance status may vary by income level given differences in insurance options for women of different incomes. Categorical coverage of pregnancy under Medicaid covers women up to 200% of the federal poverty level in the median state; income-based Medicaid covers parents and caregivers up to 138% of the federal poverty level in the median state; Affordable Care Act Marketplace subsidies cover women from 100 to 400% of the federal poverty level in all states; and employer-sponsored coverage covers working, generally higher income, women. For interpretability, we reported the results of the logistic regression models as predicted probabilities. We also calculated the adjusted average marginal differences in the predicted probability of uninsurance between white non-Hispanic women (the reference category) and other racial–ethnic categories.
We set a 95% CI a priori and conducted all analyses using Stata 15.1. Design features and survey weights provided by the CDC were applied with Stata's survey commands to account for the complex survey design. We calculated predicted probabilities using the Stata margins command with covariates held at observed sample values. The University of Michigan Institutional Review Board deemed this study of de-identified survey data exempt from review.
RESULTS
The sample included 107,921 women with complete insurance information. Table 1 presents the demographic characteristics of the sample.
TABLE 1.
Sample Characteristics by Race–Ethnicity

The unadjusted rate of uninsurance at preconception was 9.4% (95% CI 9.0–9.8) among white non-Hispanic women (Fig. 1; Appendix 1 [Appendix 1 is available online at http://links.lww.com/AOG/B772]). We found higher rates of preconception uninsurance among black non-Hispanic (12.8%, 95% CI 12.0–13.7), Hispanic English-speaking (22.3%, 95% CI 20.6–24.1), Hispanic Spanish-speaking (55.1%, 95% CI 53.0–57.1), and indigenous women (23.7%, 95% CI 21.3–26.2). At delivery, all race–ethnicities except Hispanic Spanish-speaking women (13.6%, 95% CI 12.1–15.1) had rates of uninsurance less than 5%. Patterns of uninsurance in the postpartum period were similar to preconception. Notably, half of Hispanic Spanish-speaking women were uninsured postpartum (53.4%, 95% CI 51.4–55.5).
Fig. 1. Insurance status by time period and race–ethnicity. Data are weighted proportions; other, mixed, or unknown race–ethnicity not shown.
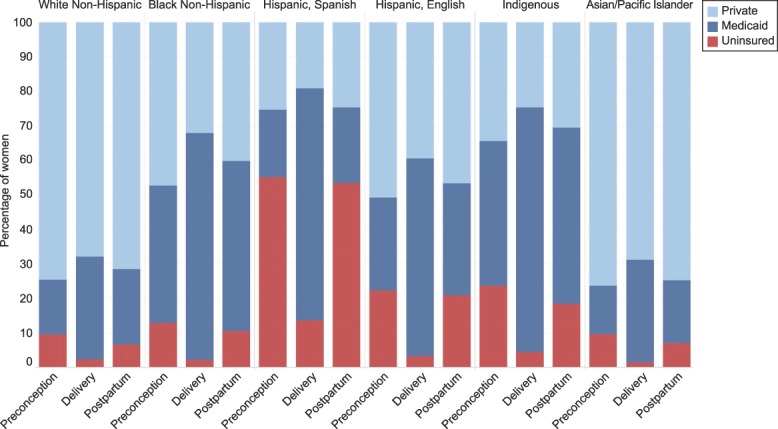
Daw. Racial–Ethnic Disparities in Perinatal Insurance Coverage. Obstet Gynecol 2020.
White non-Hispanic (75.3%, 95% CI 74.7–75.8) and Asian and Pacific Islander (75.5%, 95% CI 73.7–77.2) women had higher rates of continuous insurance compared with all other racial–ethnic categories (Fig. 2; Appendix 2 [Appendix 2 is available online at http://links.lww.com/AOG/B772]). Only 55.4% of black non-Hispanic women had continuous insurance (95% CI 54.2–56.6); 24.9% experienced a private–Medicaid discontinuity (95% CI 23.8–25.9), and 19.2% experienced an insurance–uninsurance discontinuity (95% CI 18.2–20.2). Approximately 50% of indigenous women had continuous insurance (95% CI 46.8–53.0); 17.3% had a private–Medicaid discontinuity (95% CI 15.0–19.8); and 31.5% has an uninsurance discontinuity (95% CI 28.9–34.2). Hispanic Spanish-speaking women had the lowest rate of continuous insurance (20.5%, 95% CI 18.9–22.2), a result of high rates of insurance–uninsurance discontinuity (59.0%, 95% CI 57.0–61.1) and continuous uninsurance (8.5%, 95% CI 7.3–9.9).
Fig. 2. Insurance continuity from preconception to postpartum by race–ethnicity. Data are weighted proportions; other, mixed, or unknown race–ethnicity not shown.
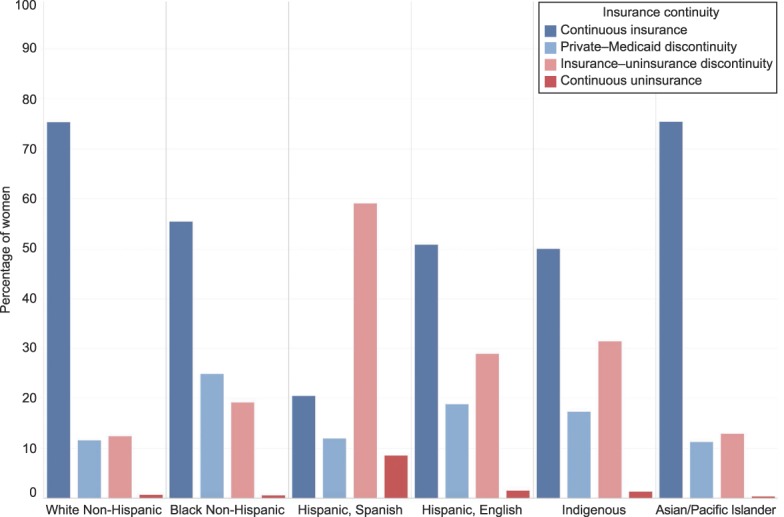
Daw. Racial–Ethnic Disparities in Perinatal Insurance Coverage. Obstet Gynecol 2020.
Among black non-Hispanic women, the percentage with any period of uninsurance ranged from 6.7% (95% CI 2.7–15.9) in New Mexico to 47.0% in South Dakota (95% CI 36.6–57.7) (Appendix 3, available online at http://links.lww.com/AOG/B772). In 18 states, at least two thirds of Hispanic Spanish-Speaking women experienced uninsurance in the perinatal period. State variation was also wide among white non-Hispanic women, ranging from 2.6% (95% CI 1.8–3.9) in Massachusetts to 29.8% (95% CI 26.7–33.2) in Texas. We did not calculate state-specific estimates for indigenous or Asian-Pacific Islander women owing to small sample sizes.
In adjusted analyses, we found the widest racial disparities in uninsurance in the preconception and postpartum period for women in the lowest income brackets (less than 138% of the federal poverty level and 139–199% of the federal poverty level ) (Fig. 3; Appendix 4 [Appendix 4 is available online at http://links.lww.com/AOG/B772]). For women at less than 138% of the federal poverty level, the predicted probability of uninsurance was 31.7 percentage points (95% CI 28.5–34.9) and 31.4 percentage points (95% CI 28.1–34.7) higher among Hispanic Spanish-speaking women compared with white non-Hispanic women in the preconception and postpartum periods, respectively. Hispanic English-speaking women with incomes less than 138% of the federal poverty level also had a higher predicted probability of preconception uninsurance (7.9 percentage points higher; 95% CI 5.2–10.6) and postpartum uninsurance (9.0 percentage points higher; 95% CI 6.4–11.5) compared with white non-Hispanic women. For each time point, black non-Hispanic women had significantly lower or similar (no statistical difference) probabilities of uninsurance compared with white non-Hispanic women, despite having significantly higher unadjusted rates of preconception and postpartum uninsurance.
Fig. 3. Adjusted predicted probability of uninsurance by time period, race–ethnicity, and household income. Preconception (A), delivery (B), and postpartum (C). Data are predicted probabilities calculated based on a logistic regression model adjusted for age, education, marital status, state of residence, household income, and an interaction term between household income and race–ethnicity; all covariates held at sample observed values. Bars represent 95% CIs. Asian or Pacific Islander and other, mixed, or unknown race–ethnicity are not shown.

Daw. Racial–Ethnic Disparities in Perinatal Insurance Coverage. Obstet Gynecol 2020.
In general, the magnitude of racial–ethnic differences decreased with increasing household income. For the highest income bracket (400% of the federal poverty level or higher), we found higher uninsurance rates for indigenous women at each time point. We did not find statistically significant racial–ethnic differences in uninsurance for black non-Hispanic or Hispanic women in the highest income bracket.
DISCUSSION
Using multistate data from 2015 to 2017, we found wide racial–ethnic disparities in insurance status and continuity of insurance coverage across the preconception, pregnancy, and postpartum periods. In the general adult and pediatric populations, uninsurance and changes between types of insurance are associated with disruptions in physician care, increased emergency department use, worsened self-reported quality of care and poor health status.17–19 Racial–ethnic disparities in insurance stability, thus, may contribute to disparities in the receipt and continuity of care across the perinatal period.
Nearly half of all black non-Hispanic women had discontinuous insurance from preconception to postpartum and one in four experienced a private–Medicaid discontinuity. However, within income groups, we found that the adjusted predicted probability of preconception and postpartum uninsurance was lower or nonsignificant for black non-Hispanic compared with white non-Hispanic women. This suggests that the population-level black-white disparity in perinatal uninsurance is largely explained by lower average household incomes among black non-Hispanic women (50.4% had household incomes less than 138% of the federal poverty level in our sample) and, in turn, higher rates of Medicaid coverage during pregnancy, which is a less stable source of coverage (65.8% compared with 29.9% for white non-Hispanic women in our sample).
Spanish-speaking Hispanic women had the highest rates of discontinuous insurance, and nearly one in 10 were continuously uninsured from preconception to postpartum. This is consistent with prior research that identified non-English language as a predictor of postpartum uninsurance.20 This finding is likely to partly reflect the limited insurance options available to immigrant women. Legal immigrants, with the exception of refugees and asylees, are subject to a 5-year waiting period for Medicaid eligibility. Although marketplace subsidies are available to immigrant women with incomes between 100% and 400% of the federal poverty level, more than half of Hispanic Spanish-speaking women in our sample had incomes less than 138% of the federal poverty level. This group is likely also partially comprised of undocumented women, who account for nearly 7% of births in the United States21 and are four times more likely than U.S. citizens to be uninsured,22 a result of more limited access to employer-sponsored coverage and restrictions on eligibility for public programs such as Medicaid.
Finally, we found that half of indigenous women experienced discontinuous insurance from preconception to postpartum (50.1%). This heterogeneous group—which comprise women from tribal nations with varied cultures in diverse communities—is often not analyzed in studies of pregnancy-related outcomes; however, the limited studies of indigenous women have found higher rates of no or inadequate prenatal care23,24 and higher infant23 and maternal mortality1 rates compared with nonindigenous women.1,23,24 In this analysis, indigenous women had the highest rate of Medicaid coverage at delivery compared with any other racial–ethnic group. Thus, ensuring Medicaid stability before and after pregnancy may be critical for coverage continuity and access to care in this population.
This study has several limitations. First, the PRAMS survey does not contain the detail necessary to examine transitions in continuity across private insurance plans (private–private discontinuity) or Medicaid programs (Medicaid–Medicaid discontinuity). Thus, estimates of insurance disruptions are likely conservative. Second, we are not able to examine within-plan changes that could affect the continuity of care, for example, if a woman's provider is removed from her insurer’s network over the course of pregnancy. Third, the results may not generalize to the 10 states not included in the survey, namely, Arizona, California, Florida, Idaho, Indiana, Minnesota, Mississippi, Nevada, North Carolina, and South Carolina. However, the included states represent a broad range of geographies and racial–ethnic compositions. The median income thresholds for Medicaid eligibility in 2019 are also similar in included and excluded states (138% of the federal poverty level and 102% of the federal poverty level for low-income parents, respectively, and 206% and 199% for pregnant women, respectively).25 Fourth, respondents self-report insurance status at the preconception and postpartum time points, which may be subject to recall and reporting bias. However, we would expect any reporting bias to be constant within individuals over the perinatal period, which would not affect measures of insurance changes. Finally, race–ethnicity information on the birth certificate could be subject to error or misreporting. Previous validation studies comparing race–ethnicity information from birth certificates to other sources have found high reliability for white, black, and Hispanic mothers, but lower specificity for indigenous populations.26–28 This could result in an underreporting of indigenous mothers in our sample.
The American College of Obstetricians and Gynecologists29 and the American Medical Association30 have recently called for interventions to mitigate perinatal insurance disruptions. One proposal, under consideration at the federal level31 and in several states,32 is the extension of pregnancy Medicaid coverage from 60 days to one year postpartum.32–35 Our findings suggest that this policy change has the potential to reduce racial–ethnic disparities in insurance disruptions experienced by Hispanic, black non-Hispanic, and indigenous women who are disproportionally enrolled in pregnancy Medicaid and experience higher rates of uninsurance in the postpartum period.
However, proposals to extend postpartum Medicaid do not address the disparities in uninsurance that we observed in the preconception period, which were similar in magnitude to those after birth. Reducing disparities in preconception coverage is also an important target for policy change, particularly as the prevalence of chronic conditions is rising among women giving birth in the United States.36 Many risk factors for adverse maternal and infant outcomes are best addressed before pregnancy, including chronic conditions, health behaviors, and exposures.37
In this analysis of data from 40 states, we found wide racial–ethnic disparities in perinatal insurance coverage and in continuity of coverage. Policies to improve continuity of coverage, especially for low-income Medicaid beneficiaries, are needed to reduce racial–ethnic disparities in perinatal uninsurance.
Footnotes
Supported by a grant awarded to Drs. Admon (PI), Dalton (Co-I), and Winkelman (Co-I) from the Health Resources and Services Administration (HRSA) of the Department of Health and Human Services (HHS) as part of an award totaling $100,000. The contents of the manuscript are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the federal government. Jamie Daw's work on this project was supported by a Calderone Junior Faculty Prize. The funders had no role in the study design, writing of the report, or the decision to submit the article for publication.
Financial Disclosure Vanessa Dalton received grant funding from the Agency for Healthcare Research (ARHQ) and Quality, National Institutes for Health (NIH), American Association of Obstetricians and Gynecologists Foundation, the Laura and John Arnold Foundation, National Institute for Reproductive Health and Blue Cross Blue Shield Foundation. She is also a paid contributing editor for the Medical Letter and an author for UpToDate. She has also serviced as a paid expert witness for Bayer, a consultant for Bind and has participated on study sections for the NIH and ARHQ. The other authors did not report any potential conflicts of interest.
The authors thank all PRAMS study participants and members of the PRAMS Working Group.
Each author has confirmed compliance with the journal's requirements for authorship.
Peer reviews and author correspondence are available at http://links.lww.com/AOG/B773.
REFERENCES
- 1.Petersen EE, Davis N, Goodman D, Cox S. Racial/ethnic disparities in pregnancy-related deaths—United States, 2007–2016. Morb Mortal Wkly Rep 2019;68:762–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Admon LK, Winkelman TNA, Zivin K, Terplan M, Mhyre JM, Dalton VK. Racial and ethnic disparities in the incidence of severe maternal morbidity in the United States, 2012–2015. Obstet Gynecol 2018;132:1158–66. [DOI] [PubMed] [Google Scholar]
- 3.Creanga AA, Berg CJ, Syverson C, Seed K, Bruce FC, Callaghan WM. Race, ethnicity, and nativity differentials in pregnancy-related mortality in the United States: 1993-2006. Obstet Gynecol 2012;120:261–8. [DOI] [PubMed] [Google Scholar]
- 4.Petersen EE, Davis NL, Goodman D. Pregnancy-related deaths, United States, 2011–2015, and strategies for prevention, 13 states, 2013–2017. Morb Mortal Wkly Rep 2019;68:423–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eisenberg JM, Power EJ. Transforming insurance coverage into quality health care: voltage drops from potential to delivered quality. JAMA 2000;284:2100–7. [DOI] [PubMed] [Google Scholar]
- 6.Martin JA, Hamilton BE, Osterman MJ, Driscoll A, Drake P. Births: final data for 2016. Natl Vital Stat Rep 2018;67:1–54. [PubMed] [Google Scholar]
- 7.D'Angelo D, Le B, O'Neil ME, Williams L, Ahluwalia IB, Harrison LL, et al. Patterns of health insurance coverage around the time of pregnancy among women with live-born infants—pregnancy risk assessment monitoring system, 29 states, 2009. Morb Mortal Wkly Rep 2015;64:1–19. [PMC free article] [PubMed] [Google Scholar]
- 8.Shulman HB, D'Angelo DV, Harrison L, Smith RA, Warner L. The pregnancy risk assessment monitoring system (PRAMS): overview of design and methodology. Am J Public Health 2018;108:1305–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Daw JR, Kozhimannil K, Admon LK. High rates of perinatal insurance churn persist after the ACA. Health Affairs Blog. Available at: https://www.healthaffairs.org/do/10.1377/hblog20190913.387157/full/. Retrieved September 24, 2019. [Google Scholar]
- 10.Artiga S, Arguello R, Duckett P. Health coverage and care for American Indians and Alaska natives. Available at: https://www.kff.org/disparities-policy/issue-brief/health-coverage-and-care-for-american-indians-and-alaska-natives/view/print/. Retrieved December 9, 2019. [Google Scholar]
- 11.National Center for Health Statistics. Long-term trends in health insurance: estimates from the national health interview survey, United States, 1968–2018. Available at: https://www.cdc.gov/nchs/data/nhis/health_insurance/TrendHealthInsurance1968_2018.pdf. Retrieved December 9, 2019. [Google Scholar]
- 12.Montoya-Williams D, Burris H, Fuentes-Afflick E. Perinatal outcomes in Medicaid expansion and nonexpansion states among Hispanic women. JAMA 2019;322:893–4. [DOI] [PubMed] [Google Scholar]
- 13.DeSisto CL, McDonald JA. Variation in birth outcomes by mother's country of birth among Hispanic women in the United States, 2013. Public Health Rep 2018;133:318–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McMorrow S, Johnston EM, Steedle R, Thomas T. Health insurance coverage for women of reproductive age, 2013–2016. Available at: https://www.urban.org/sites/default/files/publication/99534/12.18.18_health_insurance_coverage_for_women_of_reproductive_age_2013-16_1.pdf. Retrieved October 28, 2019. [Google Scholar]
- 15.Thomson MD, Hoffman-Goetz L. Defining and measuring acculturation: a systematic review of public health studies with Hispanic populations in the United States. Soc Sci Med 2009;69:983–91. [DOI] [PubMed] [Google Scholar]
- 16.Carter-Pokras O, Zambrana RE, Yankelvich G, Estrada M, Castillo-Salgado C, Ortega AN. Health status of Mexican-origin persons: do proxy measures of acculturation advance our understanding of health disparities? J Immigr Minor Health 2008;10:475–88. [DOI] [PubMed] [Google Scholar]
- 17.Sommers BD, Gourevitch R, Maylone B, Blendon RJ, Epstein AM. Insurance churning rates for low-income adults under health reform: lower than expected but still harmful for many. Health Aff (Millwood) 2016;35:1816–24. [DOI] [PubMed] [Google Scholar]
- 18.Federico SG, Steiner JF, Beaty B, Crane L, Kempe A. Disruptions in insurance coverage: patterns and relationship to health care access, unmet need, and utilization before enrollment in the state children's health insurance program. Pediatrics 2007;120:e1009–16. [DOI] [PubMed] [Google Scholar]
- 19.Lavarreda SA, Gatchell M, Ponce N, Brown ER, Chia YJ. Switching health insurance and its effects on access to physician services. Med Care 2008;46:1055–63. [DOI] [PubMed] [Google Scholar]
- 20.Daw JR, Hatfield LA, Swartz K, Sommers BD. Women in the United States experience high rates of coverage “churn” in months before and after childbirth. Health Aff (Millwood) 2017;36:598–606. [DOI] [PubMed] [Google Scholar]
- 21.Passel JS, Cohn D. Number of babies born to unauthorized immigrants in U.S. continued to decline in 2014. Available at: http://www.pewresearch.org/fact-tank/2016/10/26/number-of-babies-born-to-unauthorized-immigrants-in-u-s-continues-to-decline/. Retrieved August 16, 2017.
- 22.Kaiser Family Foundation. Health coverage of immigrants. Available at: https://www.kff.org/disparities-policy/fact-sheet/health-coverage-of-immigrants/. Retrieved April 16, 2018. [Google Scholar]
- 23.Baldwin LM, Grossman DC, Casey S, Hollow W, Sugarman JR, Freeman WL, et al. Perinatal and infant health among rural and urban American Indians/Alaska Natives. Am J Public Health 2002;92:1491–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Castor ML, Smyser MS, Taualii MM, Park AN, Lawson SA, Forquera RA. A nationwide population-based study identifying health disparities between American Indians/Alaska Natives and the general populations living in select urban counties. Am J Public Health 2006;96:1478–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kaiser Family Foundation. Where are states today? Medicaid and CHIP eligibility levels for children, pregnant women, and adults. Available at: http://www.kff.org/medicaid/fact-sheet/where-are-states-today-medicaid-and-chip/#table2. Retrieved May 1, 2019. [Google Scholar]
- 26.Baumeister L, Marchi K, Pearl M, Williams R, Braveman P. The validity of information on “race” and “Hispanic ethnicity” in California birth certificate data. Health Serv Res 2000;35:869–83. [PMC free article] [PubMed] [Google Scholar]
- 27.Reichman NE, Hade EM. Validation of birth certificate data: a study of women in New Jersey's HealthStart program. Ann Epidemiol 2001;11:186–93. [DOI] [PubMed] [Google Scholar]
- 28.Mason LR, Nam Y, Kim Y. Validity of infant race/ethnicity from birth certificates in the context of U.S. demographic change. Health Serv Res 2014;49:249–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.American College of Obstetricians and Gynecologists. ACOG statement on AMA support for 12 months of postpartum coverage under Medicaid. Available at: https://www.acog.org/About-ACOG/News-Room/Statements/2019/AMA-Support-for-12-Months-Postpartum-Medicaid-Coverage?IsMobileSet=false. Retrieved August 2, 2019. [Google Scholar]
- 30.American Medical Association. AMA adopts new policies at 2019 annual meeting. Available at: https://www.ama-assn.org/press-center/press-releases/ama-adopts-new-policies-2019-annual-meeting. Retrieved October 21, 2019. [Google Scholar]
- 31.Congress.gov. H.R.4996: Helping MOMS Act of 2019. 116th Congress. Available at: https://www.congress.gov/bill/116th-congress/house-bill/4996. Retrieved December 10, 2019. [Google Scholar]
- 32.Ranji U, Gomez I, Salganicoff A. Expanding postpartum Medicaid coverage. Available at: https://www.kff.org/womens-health-policy/issue-brief/expanding-postpartum-medicaid-coverage/. Retrieved August 7, 2019. [Google Scholar]
- 33.Peahl A, Kozhimannil K, Admon LK. Addressing the US maternal health crisis: policies of 2020 presidential candidates. Health Affairs Blog. Available at: https://www.healthaffairs.org/do/10.1377/hblog20190625.583781/full/. Retrieved June 26, 2019. [Google Scholar]
- 34.Congress.gov. S.3494:MOMMIES Act. 115th Congress. Available at: https://www.congress.gov/bill/115th-congress/senate-bill/3494. Retrieved October 21, 2019. [Google Scholar]
- 35.Congress.gov. H.R.1897 MOMMA's Act. 116th Congress. Available at: https://www.congress.gov/bill/116th-congress/house-bill/1897/text. Retrieved October 21, 2019. [Google Scholar]
- 36.Admon LK, Winkelman TNA, Moniz MH, Davis MM, Heisler M, Dalton VK. Disparities in chronic conditions among women hospitalized for delivery in the United States, 2005-2014. Obstet Gynecol 130;2017:1319–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Prepregnancy counseling. ACOG Committee Opinion No. 762. American College of Obstetricians and Gynecologists. Obstet Gynecol 2019;133:e78–89. [DOI] [PubMed] [Google Scholar]