
Fig. 2.
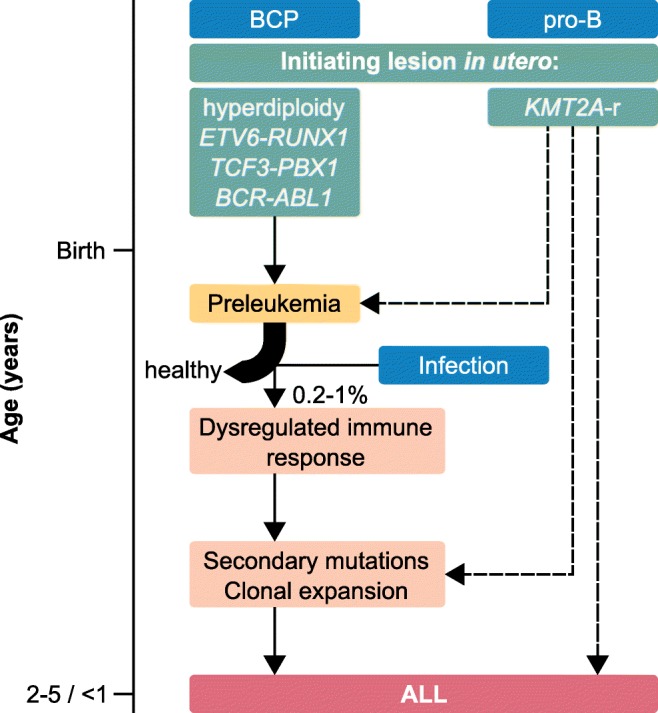
Timeline of ALL development. The initiating lesions (green) occur in utero and lead to a state of preleukemia after birth. Exposure to infection leads to a dysregulated immune response in a small fraction (about 0.2–1%) of preleukemic children. Most preleukemic children remain healthy [6, 7]. The children develop ALL by acquiring secondary mutations, eventually leading to clonal expansion. In the case of KMT2A rearrangements (KMT2A-r, right), it is not completely clear whether the KMT2A-r are sufficient for ALL development (right dashed arrow). It is also possible that the KMT2A-r directly trigger secondary mutations (central dashed arrow). One case of a healthy KMT2A-r carrier has been reported [13], leading to the possibility of a preleukemic state for those cases (left dashed arrow). The given median ages of ALL onset are 2–5 years of age for B cell precursor subtypes (BCP, left) and < 1 year of age for pro-B cell subtype (pro-B, right)