

Abstract
Bloodstream infections caused by uncommon or novel fungal species are challenging to identify and treat. We report a series of cases of fungemia due to a rare basidiomycete yeast, Dirkmeia churashimaensis, in neonatal patients in India. Whole-genome sequence typing demonstrated that the patient isolates were genetically indistinguishable, indicating a single-source infection.
Keywords: Dirkmeia churashimaensis, outbreak, bloodstream infections, neonatal intensive care unit, whole-genome sequencing, antimicrobial resistance, yeast, fungi, India
During the past decade, outbreaks of bloodstream infections (BSIs) caused by rare and challenging to identify fungi have increased (1). Many rare infections occurred among patients admitted to neonatal intensive care units (NICUs). Rarely, yeasts belonging to the phylum Basidiomycota, including genera Malassezia, Trichosporon, and Rhodotorula (2–4), have been implicated in outbreaks in NICUs.
Dirkmeia churashimaensis (previously Pseudozyma churashimaensis) is a rare basidiomycete, ustilaginomycetous, anamorphic yeast first isolated in 2008 from the leaves of sugar cane (Saccharum officinarum) in Okinawa, Japan (5). Initially, D. churashimaensis was identified as a novel Pseudozyma species on the basis of morphological and physiologic aspects and by molecular analysis of the D1/D2 domains and internal transcribed spacer (ITS) regions (5). In 2015, Wang et al. used multigene phylogeny and proposed that P. churashimaensis represents a new genus, Dirkmeia gen. nov. (6). Dirkmeia gen. nov. is a common endophytic yeast found in the leaf tissues of rice, corn, sugar cane, and pepper plants (7). Of note, foliar application of this leaf-colonizing yeast has been reported to control plant viral disease under field conditions (8). However, D. churashimaensis has not been reported to cause human infections. We report an unusual cluster of 12 cases of fungemia caused by D. churashimaensis among NICU patients in a multispecialty hospital in Delhi, India.
The Study
During June 2016–January 2017, a total of 12 cases of fungemia occurred among neonates admitted to a 24-bed NICU of a multispecialty hospital in Delhi. Cases of BSI were defined as the isolation of D. churashimaensis from >1 peripheral blood culture in patients with signs and symptoms of sepsis. The first case of fungal sepsis was observed in a preterm infant with very low birthweight (<1,500 g) who experienced asphyxia during birth. The patient’s blood culture was positive for yeast on day 6 after birth. Fluconazole treatment was initiated by administering a loading dose of 12 mg/kg bodyweight, after which the patient received 6 mg/kg bodyweight in addition to vancomycin and meropenem. The second case occurred 2 weeks later in a preterm baby with low birthweight (<2,500 g) whose blood culture yielded D. churashimaensis on day 2. During the next 6 months, 10 additional cases of D. churashimaensis BSI were identified (Table 1).
Table 1. Clinical details of patients with Dirkmeia churashimaensis fungemia in a neonatal intensive care unit, India*.
| Pt no. | Isolate ID | GA, wk/sex | DOB; delivery method | Birthweight, g | Date blood sample collected | Day of positive blood test† | Risk factors | Antifungal therapy‡ | NICU stay, d; outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 |
VPCI 2456/P/16§ |
31/M |
2016 Jun 25; LSCS |
1,400 |
2016 Jun 25 |
6 |
PT, VLBW, IUGR, thrombocytopenia, CVC, severe asphyxia, sepsis, mechanical ventilation |
FLU, 10 d; VAN and MER, 7 d |
15; survived |
| 2 |
VPCI 2478/P/16 |
29/M |
2016 Jul 7; LSCS |
1,100 |
2016 Jul 8 |
2 |
PT, VLBW, IUGR, sepsis, thrombocytopenia |
FLU, 14 d;
VAN and MER, 10 d |
12; survived |
| 3 |
VPCI 2510/P/16 |
29/F |
2016 Jul 19; VD |
1,000 |
2016 Jul 19 |
4 |
PT, VLBW, sepsis, thrombocytopenia |
FLU, 14 d;
VAN and MER, 14 d |
18; survived |
| 4 |
VPCI 2515/P/16§ |
27/F |
2016 Aug 30; VD |
1,000 |
2016 Aug 31 |
4 |
PT, VLBW, IUGR, thrombocytopenia, maternal history of preeclampsia, antepartum hemorrhage |
FLU, 14 d;
AMI and CIP, 12 d |
16; survived |
| 5 |
VPCI 2601/P/16 |
32/F |
2016 Sep 24; LSCS |
1,200 |
2016 Sep 24 |
3 |
PT, VLBW, persistent hypoglycemia, severe asphyxia, sepsis, CVC, mechanical ventilation |
FLU, 10 d;
VAN and MER, 12 d |
6; died |
| 6 |
VPCI 2634/P/16 |
27/M |
2016 Oct 17; VD |
750 |
2016 Oct 17 |
5 |
Extremely PT, ELBW, severe asphyxia, CVC, sepsis, mechanical ventilation |
FLU, 10 d |
8; died |
| 7 |
VPCI 2699/P/16§ |
30/M |
2016 Nov 9; VD |
800 |
2016 Nov 9 |
2 |
PT, ELBW, sepsis, persistent hypoglycemia, severe asphyxia, CVC, mechanical ventilation |
FLU, 10 d;
VAN and MER, 10 d |
11; died |
| 8 |
VPCI 2759/P/16 |
33/M |
2016 Nov 26; LSCS |
1,200 |
2016 Nov 28 |
3 |
PT, VLBW, severe asphyxia, CVC,
thrombocytopenia, persistent hypoglycemia, mechanical ventilation |
FLU, 14 d;
VAN and MER, 10 d |
10; survived |
| 9 |
VPCI 2801/P/16§ |
27/M |
2016 Dec 14; VD |
1,100 |
2016 Dec 14 |
4 |
PT, VLBW, severe asphyxia, thrombocytopenia, sepsis, CVC, mechanical ventilation |
FLU, 18 d;
VAN and MER, 12 d |
24; survived |
| 10 |
VPCI 2845/P/16 |
27/F |
2016 Dec 28; LSCS |
1,200 |
2016 Dec 28 |
6 |
PT, VLBW, thrombocytopenia, mechanical ventilation, sepsis, persistent hypoglycemia, CVC |
FLU, 10 d;
VAN and MER, 8 d |
8; died |
| 11 |
VPCI 2224/P/17§ |
30/M |
2017 Jan 3; LSCS |
1,350 |
2017 Jan 3 |
4 |
PT, VLBW, sepsis, persistent hypoglycemia, CVC |
FLU, 10 d;
VAN and MER, 10 d |
14; survived |
| 12 | VPCI 2271/P/17§ | 29/F | 2017 Jan 18; VD | 1,000 | 2017 Jan 19 | 4 | PT, VLBW, thrombocytopenia, mechanical ventilation, CVC, sepsis, persistent hypoglycemia | FLU, 10 d; VAN and MER, 12 d | 9; died |
*AMI, amoxicillin; CIP, ciprofloxacin; CVC, central venous catheter; DOB, date of birth; ELBW, extremely low birthweight (<1,000 g); FLU, fluconazole; GA, gestational age; ID, identification; IUGR, intrauterine growth restriction; LSCS, lower segment cesarean section; MER, meropenem; PT, preterm; Pt., patient; VAN, vancomycin; VPCI, Vallabhbhai Patel Chest Institute (Delhi, India); VD, vaginal delivery; VLBW, very low birthweight (<1,500 g). †Indicates days after birth. ‡All patients were given a 1-time loading dose of 12 mg/kg bodyweight of FLU and then 6 mg/kg bodyweight. §Isolates selected for whole-genome sequencing.
Isolates grew as yeast-like cream to pale yellow, dry, and wrinkled colonies with fringes on the margin on Sabouraud glucose agar at 35°C after 48 h of incubation; the isolates grew slowly at 37°C over 3 days. Micromorphology showed fusiform yeast cells with hyphae and polar budding with short denticles. Identification by VITEK2 (bioMérieux, https://www.biomerieux.com) yielded Cryptococcus laurentii with 88% probability. We conducted carbon assimilation on isolates and noted assimilation of D-trehalose and N-acetyl-glucosamine at 37°C in 48 h.
Because no multilocus sequence or microsatellite typing were available, we used whole-genome sequencing (WGS) and amplified fragment-length polymorphism typing to understand the genetic relationships among isolates. We conducted matrix-assisted laser desorption/ionization-time of flight mass spectrometry by using Biotyper 3.1 (Bruker Corp., https://www.bruker.com) to identify the yeasts. However, because no database of this yeast is available, we were not able to make an identification. The in-house database created yielded correct identification in the remaining 10 isolates with high score values (>2).
We used isolates ITS and D1/D2 regions to sequence isolates, as described previously (9). We searched ITS and D1/D2 region sequences in BLAST (https://blast.ncbi.nlm.nih.gov) and identified isolates from the outbreak as D. churashimaensis. The isolates had >99% identity with D. churashimaensis sequences from GenBank (accession nos. MN758637–48 and MN158668–79).
We used MEGA 7 (https://www.megasoftware.net) to perform phylogenetic analysis of ITS sequences by using the neighbor-joining method with 2,000 bootstrap values. All isolates from the outbreak clustered together. The reference D. churashimaensis isolate formed a distinct cluster but showed 99% nucleotide similarity with isolates from the outbreak. We performed amplified fragment-length polymorphism fingerprint analysis, as described previously (10), which yielded identical banding pattern among all 12 isolates, suggesting clonal origin (Figure 1).
Figure 1.
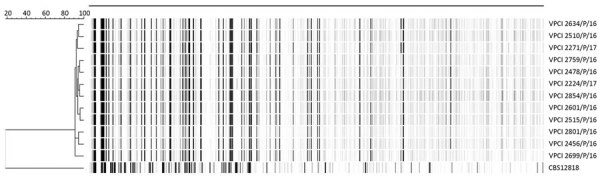
Dendrogram of amplified fragment-length polymorphism analysis of Dirkmeia churashimaensis isolated from 12 cases of fungemia in patients in a neonatal intensive care unit, Delhi, India. The dendrogram was constructed by using unweighted pair group method with averages and the Pearson correlation coefficient. Dendrogram was restricted to fragments of 60–400 bp. CBS12818, a Pseudozyma aphidis isolate previously reported from neonatal fungemia in India, was included in the analysis. Scale bar indicates the percentage similarity. VPCI, Vallabhbhai Patel Chest Institute (Delhi, India).
We performed WGS on 6 isolates by using IonPGM (IonTorrent; ThermoFisher, https://www.thermofisher.com) next-generation sequencing technology, following the manufacturer’s protocol. We deposited sequences into BioProject (accession no. PRJEB35981). We identified average nucleotide identity and SNPs by comparing 6 genomes in MUMmer (http://mummer.sourceforge.net) and compared all the genomes against other publicly available basidiomycete yeast genomes (Table 2) by using progressiveMauve (11). We constructed a whole-genome SNP-based phylogenetic tree by using SplitsTree4 (12; Figure 2). The assembled genome size of D. churashimaensis is ≈21 Mb with a G+C content of 58%. The assembly contained 397–502 contigs ranging in length from 535,979 to 946,852 bp (average contig length 741,415 bp). D. churashimaensis isolates were genotypically indistinguishable and had 99.6% similarity among the genomes (average nucleotide identity >99.6%; Table 2). The average number of SNP differences between isolates was 1,074.5 (range 402–1,621), indicating high clonality.
Table 2. Results of average nucleotide identity analysis giving percentage similarity among Dirkmeia churashimaensis isolates from patients in a neonatal intensive care unit, India, compared with other basidiomycetes and Saccharomyces cerevisiae isolates*.
| Isolate ID |
Isolate ID |
|||||
| VPCI 2456/P/16 |
VPCI 2515/P/16 |
VPCI 2699/P/16 |
VPCI 2801/P/16 |
VPCI 2224/P/17 |
VPCI 2217/P/17 |
|
| VPCI 2456/P/16 | 100 | 99.86 | 99.86 | 99.87 | 99.86 | 99.86 |
| VPCI 2515/P/16 | 99.87 | 100 | 99.89 | 99.91 | 99.93 | 99.91 |
| VPCI 2699/P/16 | 99.86 | 99.9 | 100 | 99.92 | 99.9 | 99.91 |
| VPCI 2801/P/16 | 99.88 | 99.91 | 99.92 | 100 | 99.89 | 99.9 |
| VPCI 2224/P/17 | 99.89 | 99.91 | 99.91 | 99.92 | 100 | 99.89 |
| VPCI 2271/P/17 | 99.88 | 99.87 | 99.88 | 99.89 | 99.89 | 100 |
| Cutaneotrichosporon oleaginosus | 68.22 | 68.82 | 68.51 | 68.68 | 68.54 | 68.57 |
| Cryptococcus neoformans | 70.94 | 69.27 | 69.99 | 70.37 | 70.15 | 69.95 |
| Trichosporon asahii | 69.54 | 63.37 | 69.32 | 69.66 | 69.78 | 69.88 |
| Saccharomyces cerevisiae | 64.82 | 63.40 | 63.56 | 64.24 | 64.48 | 64.52 |
*ID, identification; VPCI, Vallabhbhai Patel Chest Institute (Delhi, India).
Figure 2.
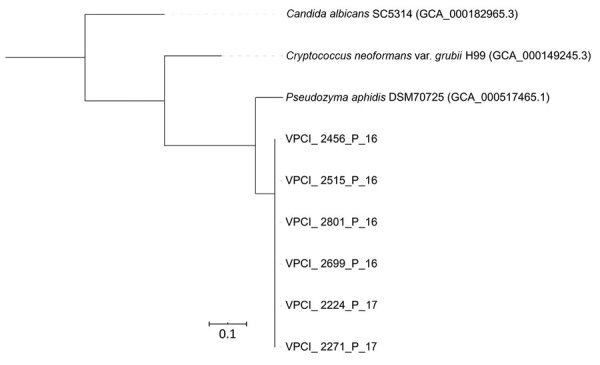
Whole-genome single-nucleotide polymorphism–based phylogenetic tree of 6 Dirkmeia churashimaensis isolates from cases of fungemia among patients in a neonatal intensive care unit, India. Other yeast species included for comparison. Scale bar indicates single-nucleotide polymorphism differences per site. VPCI, Vallabhbhai Patel Chest Institute (Delhi, India).
We conducted antifungal susceptibility testing using microbroth dilution method published by the US Clinical Laboratory Standards Institute (13). As expected with Basidiomycota, isolates in this outbreak were resistant to echinocandins. Susceptibility testing showed that all isolates were resistant to caspofungin, anidulafungin, and micafungin (MICs >8 µg/mL). However, all isolates had low MICs for azoles, including voriconazole (MIC 0.03–0.125 µg/mL; geometric mean [GM] 0.04 µg/mL), isavuconazole (MIC 0.03–0.125 µg/mL; GM 0.05 µg/mL), itraconazole (MIC 0.03–0.25 µg/mL; GM 0.057 µg/mL), posaconazole (MIC 0.03–0.25 µg/mL; GM 0.092 µg/mL), and fluconazole (MIC 1–4 µg/mL; GM 2.37 µg/mL). Amphotericin B (GM MIC 0.198 µg/mL) and 5-flucytosine (GM MIC0.157 µg/mL) had potent activity.
All patients were treated with fluconazole at a loading dose of 12 mg/kg bodyweight and then 6 mg/kg for 10–14 days; 5 patients died, a case-fatality rate of 42%. All patients had risk factors, such as preterm birth or low or very low birthweight, and 8/12 were intubated (Table 1). The most serious risk factors were central venous catheter (n = 9), thrombocytopenia (n = 8), and severe asphyxia (n = 6). The age at the onset of fungemia ranged from 2 to 6 days, and the attack rate was 0.33 during the 6-month outbreak. The mean gestational age was 29.2 weeks and the mean birthweight was 1.1 kg. Altogether, 11 patients had 1–6 days of antimicrobial drug therapy before isolation of yeast in blood culture.
After the second case of fungemia was identified, infection control measures were implemented and surveillance cultures obtained to trace the source of infection. Doctors, nursing staff, and assistants in the NICU were screened for hand carriage of the yeast, and extensive sampling of fomites including floors, equipment, disinfectants, vials, and infusion pumps was conducted. All environmental cultures were negative, and no other cases of fungemia due to D. churashimaensis were identified after continued compliance with infection control measures, including rigorous handwashing practice.
Conclusions
Our report highlights not only clinical importance of rare yeast species in the NICU but also emphasizes that WGS provides a highly sensitive tool for genotyping pathogens without prior knowledge of the genomes (1,14,15). Major healthcare-associated outbreaks of uncommon and novel fungal species have occurred in recent years, including Candida auris from a clonal outbreak in India (9). Mycologists should be vigilant when they isolate unusual or rare yeasts with potential antifungal resistance. Considerable challenges remain in the diagnosis of rare and unusual yeasts and the risk for misidentification of cases and outbreaks is high. Our findings reinforce the need for awareness of this new fungal risk among the public health community.
Acknowledgments
We thank Pradip Roy for technical assistance and Ferry Hagen for assistance in AFLP.
This work was supported in part by a research grant from the India Council of Medical Research under funding no. OMI/13/2014-ECD-I to A.C., Government of India, New Delhi, India.
J.F.M. has received grants from Astellas, Basilea, F2G, and Merck; has been a consultant to Astellas, Basilea, and Scynexis; and has received speaker’s fees from Astellas, Merck, United Medical, TEVA, and Gilead.
Biography
Dr. Chowdhary is a clinical microbiologist and a professor at the Vallabhbhai Patel Chest Institute, Delhi, India. Her main research interest is fungal infections.
Footnotes
Suggested citation for this article: Chowdhary A, Sharada K, Singh PK, Bhagwani DK, Kumar N, de Groot T, et al. Outbreak of Dirkmeia churashimaensis fungemia in a neonatal intensive care unit, India. Emerg Infect Dis. 2020 Apr [date cited]. https://doi.org/10.3201/eid2604.190847
References
- 1.Litvintseva AP, Brandt ME, Mody RK, Lockhart SR. Investigating fungal outbreaks in the 21st century. PLoS Pathog. 2015;11:e1004804. 10.1371/journal.ppat.1004804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Basu S, Tilak R, Kumar A. Multidrug-resistant Trichosporon: an unusual fungal sepsis in preterm neonates. Pathog Glob Health. 2015;109:202–6. 10.1179/2047773215Y.0000000019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ilahi A, Hadrich I, Goudjil S, Kongolo G, Chazal C, Léké A, et al. Molecular epidemiology of a Malassezia pachydermatis neonatal unit outbreak. Med Mycol. 2018;56:69–77. 10.1093/mmy/myx022 [DOI] [PubMed] [Google Scholar]
- 4.Perniola R, Faneschi ML, Manso E, Pizzolante M, Rizzo A, Sticchi Damiani A, et al. Rhodotorula mucilaginosa outbreak in neonatal intensive care unit: microbiological features, clinical presentation, and analysis of related variables. Eur J Clin Microbiol Infect Dis. 2006;25:193–6. 10.1007/s10096-006-0114-2 [DOI] [PubMed] [Google Scholar]
- 5.Morita T, Ogura Y, Takashima M, Hirose N, Fukuoka T, Imura T, et al. Isolation of Pseudozyma churashimaensis sp. nov., a novel ustilaginomycetous yeast species as a producer of glycolipid biosurfactants, mannosylerythritol lipids. J Biosci Bioeng. 2011;112:137–44. 10.1016/j.jbiosc.2011.04.008 [DOI] [PubMed] [Google Scholar]
- 6.Wang QM, Begerow D, Groenewald M, Liu XZ, Theelen B, Bai FY, et al. Multigene phylogeny and taxonomic revision of yeasts and related fungi in the Ustilaginomycotina. Stud Mycol. 2015;81:55–83. 10.1016/j.simyco.2015.10.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khunnamwong P, Jindamorakot S, Limtong S. Endophytic yeast diversity in leaf tissue of rice, corn and sugarcane cultivated in Thailand assessed by a culture-dependent approach. Fungal Biol. 2018;122:785–99. 10.1016/j.funbio.2018.04.006 [DOI] [PubMed] [Google Scholar]
- 8.Lee G, Lee SH, Kim KM, Ryu CM. Foliar application of the leaf-colonizing yeast Pseudozyma churashimaensis elicits systemic defense of pepper against bacterial and viral pathogens. Sci Rep. 2017;7:39432. 10.1038/srep39432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chowdhary A, Sharma C, Duggal S, Agarwal K, Prakash A, Singh PK, et al. New clonal strain of Candida auris, Delhi, India. Emerg Infect Dis. 2013;19:1670–3. 10.3201/eid1910.130393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kathuria S, Sharma C, Singh PK, Agarwal P, Agarwal K, Hagen F, et al. Molecular epidemiology and in-vitro antifungal susceptibility of Aspergillus terreus species complex isolates in Delhi, India: evidence of genetic diversity by amplified fragment length polymorphism and microsatellite typing. PLoS One. 2015;10:e0118997. 10.1371/journal.pone.0118997 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Darling AE, Mau B, Perna NT. progressiveMauve: multiple genome alignment with gene gain, loss and rearrangement. PLoS One. 2010;5:e11147. 10.1371/journal.pone.0011147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Huson DH, Bryant D. Application of phylogenetic networks in evolutionary studies. Mol Biol Evol. 2006;23:254–67. 10.1093/molbev/msj030 [DOI] [PubMed] [Google Scholar]
- 13.Clinical Laboratory Standards Institute. Reference method for broth dilution antifungal susceptibility testing. 4th ed. CLSI standard M27. Wayne (PA): The Institute; 2017. [Google Scholar]
- 14.Etienne KA, Roe CC, Smith RM, Vallabhaneni S, Duarte C, Escadón P, et al. Whole-genome sequencing to determine origin of multinational outbreak of Sarocladium kiliense bloodstream infections. Emerg Infect Dis. 2016;22:476–81. 10.3201/eid2203.151193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vaux S, Criscuolo A, Desnos-Ollivier M, Diancourt L, Tarnaud C, Vandenbogaert M, et al. ; Geotrichum Investigation Group. Multicenter outbreak of infections by Saprochaete clavata, an unrecognized opportunistic fungal pathogen. MBio. 2014;5:e02309–14. 10.1128/mBio.02309-14 [DOI] [PMC free article] [PubMed] [Google Scholar]