

ABSTRACT
Background
Cooking interventions have been linked to reductions in obesity and improvements in dietary intake in children.
Objective
To assess whether child cooking involvement (CCI) was associated with fruit intake (FI), vegetable intake (VI), vegetable preference (VP), and vegetable exposure (VE) in children participating in the Texas, Grow! Eat! Go! (TGEG) randomized controlled trial.
Methods
Baseline data from TGEG included 1231 3rd grade students and their parents. Conducted in 28 low-income, primarily Hispanic schools across Texas, TGEG schools were assigned to: 1) Coordinated School Health (CSH) only (control group), 2) CSH plus gardening and nutrition intervention (Learn, Grow, Eat & Go! or LGEG group), 3) CSH plus physical activity intervention (Walk Across Texas or WAT group), and 4) CSH plus LGEG plus WAT (combined group). Height, weight, dietary intake, VE, VP, and CCI were collected at baseline and postintervention. Linear regressions were used to assess the relation between baseline CCI and fruit and vegetable (FV) intake, VE, and VP. A priori covariates included age, sex, race/ethnicity, and TGEG treatment group.
Results
Children who were always involved in family cooking had higher VP and VE when compared with children who were never involved in family cooking (β = 3.26; 95% CI: 1.67, 4.86; P < 0.01 and β = 2.26; 95% CI: 0.67, 3.85; P < 0.01, respectively). Both VI and FI were higher for children who were always involved in family cooking compared with children who never cooked with their family (β = 2.45; 95% CI: 1.47, 3.44; P < 0.01 and β = 0.93; 95% CI: 0.48, 1.39; P < 0.01, respectively). VI and fruit consumption were higher for children who reported being sometimes involved in family cooking compared with children who were never involved in family cooking, (β = 1.47; 95% CI: 0.51, 2.42; P < 0.01, and β = 0.64; 95% CI: 0.20, 1.08; P < 0.01, respectively).
Conclusions
Results show a positive relation between family cooking and FV intake and preference in high-risk, minority children.
Keywords: childhood obesity, obesity, nutrition, cooking, dietary intake, vegetable preference, vegetable exposure, fruit intake
Introduction
In 2011–2014, 17.5% of children in the USA aged 6–11 y were classified as having obesity (1). A greater percentage of Hispanic children of this age group are affected by obesity than their non-Hispanic white counterparts (25.0% and 13.6%, respectively) (1–3). Low socioeconomic status (SES) is also linked to increased obesity prevalence in youth (4). This is a serious concern, as childhood obesity is associated with a multitude of health problems such as cardiovascular disease, type 2 diabetes (T2D), and other metabolic diseases (2, 5–7) both in childhood and later in life. Many studies have examined the effects of fruit and vegetable (FV) intake on weight gain; however, the results are mixed and vary significantly. Some studies show null results, whereas others demonstrate that increased FV intake is associated with decreased weight gain and obesity (8–10). Although the findings for FV intake and its mitigating effect on weight gain are inconclusive, FV intake has been shown to be inversely associated with T2D risk, visceral fat, liver fat, and insulin resistance in Hispanic children (11, 12). Additionally, FV consumption may reduce the risk of metabolic diseases (10, 13).
The majority of children in the USA do not meet the dietary guidelines for FV, and Hispanic children and children from low SES households are at an even greater risk of not meeting these guidelines (13–16). FV consumption is predicted by FV preference (17), and food preferences are formed during childhood (18). It has been shown that repeated exposure to a particular food is correlated with developing a preference for that food (19). Children typically do not like vegetables, so it is essential to expose them to vegetables as a means of increasing their preference for vegetables early on (20). Fruit and vegetable consumption is beneficial to overall health and needs to be integrated into the diets of US children, especially high-risk children, in order to decrease obesity and obesity-related diseases in this population. Finding novel ways to improve FV intake in these high-risk populations is warranted.
Although the majority of school-based cooking interventions show promise in effectively improving vegetable preference (VP) and consumption in children, a few studies have shown no difference in vegetable consumption between intervention participants and controls (8, 21–23). One reason for these inconsistent results may be because of the degree of cooking activities in these interventions differs widely. Food preparation skills have been identified as an important factor in improving FV consumption, and a lack of these skills is a barrier to healthy food preparation and consumption (24). One study found that cooking classes increase FV consumption in children, and numerous other studies have found that children who cook with their parents eat more FV than children whose parents cook without their child's involvement (25–28). School-based gardening interventions have also shown inconsistent results in reporting interventional effects on increasing FV consumption among children (8). A review of literature posited that future garden interventions may benefit from adding a parental component (8).
Because parents play such a key role in determining what a child consumes, it is necessary to engage both children and parents in efforts to improve children's dietary intake (14). Numerous parent behaviors have been identified as key contributors to improving child dietary intake, such as providing access to vegetables at home and preparing meals together with their children (14, 29). Parental engagement of their children in food preparation/cooking activities as well as making healthy options available for their children could be a prudent way to improve the dietary intake of a child.
School-based cooking and gardening interventions that have involved children and their parents, particularly those low-income and minority families, appear to be a promising strategy to get children to prepare meals with their parents at home (29). Although many school-based intervention studies include cooking activities in their curriculum and show improvements in VP and consumption in children (8, 21–23, 30), few studies have examined the effects of cooking skills and increased cooking in the home on FV preference and intake. The aim of this cross-sectional study was to examine the associations between baseline child cooking involvement (CCI) with FV preferences and intake in low-income Hispanic 3rd grade students in the Texas, Grow! Eat! Go! (TGEG) randomized controlled trial (RCT) (29, 31). It was hypothesized that greater CCI would be associated with greater preferences for and intake of fruits and vegetables as well as greater vegetable exposure (VE).
Methods
Study design
Baseline data from the TGEG intervention were used for this study. TGEG was a 4-way group RCT in which 28 schools from 4 counties in Texas were randomly assigned to 1 of the following groups: 1) Coordinated School Health (CSH) only (control group), 2) CSH plus gardening and nutrition intervention (Learn! Grow! Eat! Go! or LGEG group), 3) CSH plus physical activity intervention (Walk Across Texas or WAT group), and 4) CSH plus LGEG plus WAT (combined group). In Texas, state policy requires all elementary schools to implement a specific Texas Education Agency-approved Coordinated School Health program (Texas Education Code § 38.0141). Schools that had selected the Coordinated Approach to Child Health (CATCH) were recruited for the TGEG study to allow for comparability of the study schools. This research was approved by the Texas A&M University Institutional Review Board (# IRB 2011–0012) and the University of Texas Health Sciences IRB, the Committee for the Protection of Human Subjects (#HSC-SPH-10-0733). All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants included in the study.
School eligibility criteria
Schools were eligible for this study if they met the following criteria: 1) classified as a Title I school (≥40% of the students live in low-income households), 2) located within 4 geographically distinct areas in Texas (Central Texas, Brazos Valley, Coastal South Texas, and South East Texas), 3) CATCH implemented as chosen CSH program (32), 4) district, principal, and 3rd grade teacher commitment, and 5) willingness to allow data collection.
Subjects
The TGEG study aimed to recruit 50 student/parent dyads from each school to achieve a total sample size of 1600 dyads. Study packets were sent home with 3rd grade students at the selected schools at the beginning of the school year in 2013 (cohort 1) and in 2014 (cohort 2), which included consent forms to be signed by parents. To be eligible for the study, students had to meet the following criteria: 1) enrollment in 3rd grade at a selected school and 2) willingness to complete the student survey at 4 time points throughout the study. Students were not eligible if they were on a special diet or if their first language was not English or Spanish. Parents had to be able to read English or Spanish and be a parent or primary caretaker of a 3rd grade student. All children received the intervention; thus, parents did not have to participate in order for their child to participate in the study. Children gave assent at the first data collection session and also received a small incentive (i.e. ruler, measuring spoons, etc.). Parents did not receive incentives for participating in the study. The current analyses only used baseline data and more detailed information on the intervention groups and the actual interventions are published elsewhere (29, 32).
Measures
The TGEG research team collected anthropometric and survey data from all 3rd grade students with a signed parental consent. Data collection occurred during the school day at a time arranged with each school's administrative staff. Prior to the start of data collection, each child was asked to complete an assent form. All data collections were conducted by trained research staff that were proficient in both English and Spanish. Child height was assessed using a stadiometer (Seca, Birmingham, UK) CDC reference values (5). CCI, VE, VP, vegetable intake (VI), and fruit intake (FI) were assessed via the Child Survey, which was developed using previously validated questionnaires including the School Physical Activity and Nutrition (SPAN) Survey (33), the GIMME5 Survey (34), and the Marathon Kids Survey (35), with additional questions that address cooking created specifically for this study. The Child Survey was available in both English and Spanish languages. VI was assessed using questions asking about foods consumed the prior day. VP and VE for 19 different vegetables were assessed using the questions “do you like to eat…” and “have you eaten…”, respectively. More detailed information on measure development, self-reported variables, and student-parent interaction variables are published elsewhere (29). Table 1 provides a complete list of the questions that were used in these analyses.
TABLE 1.
Texas, Grow! Eat! Go! Key outcome variables and cooking questions
| Outcome variable | Example item | #Items | Response options |
|---|---|---|---|
| Child Survey | |||
| Vegetable preference | Do you like to eat…? (list of 19 vegetables) | 19 | 0–1 (0 = no, 1 = yes) |
| Vegetable exposure | Have you eaten…? (list of 19 vegetables) | 19 | 0–1 (0 = no, 1 = yes) |
| Vegetable intake | Yesterday, did you eat any orange vegetables like carrots, squash, or sweet potatoes? | 4 | 0–3 (0 = none, 1 = 1 time yesterday, 2 = 2 times yesterday, 3 = 3 or more times yesterday) |
| Fruit intake | Yesterday, did you eat fruit? Fruits are all fresh, frozen, canned or dried fruits. DO NOT COUNT fruit juice | 1 | 0–3 (0 = none, 1 = 1 time yesterday, 2 = 2 times yesterday, 3 = 3 or more times yesterday) |
| Child cooking involvement | How often do you help make food with members of your family? | 1 | 0–2 (0 = never or almost never, 1 = sometimes, 2 = almost always or always) |
| Parent Survey | |||
| Parent support for child cooking | During the week, did you do the following with your child? Prepared food together | 2 | 0–1 (0 = no, 1 = yes) |
Statistical analysis
Among our 3rd grade sample, participation rates varied per school with a mean participation rate of 56% (participation scores ranged from 24% to 90%). The goal of the TGEG study was to recruit 50 child/parent dyads per school. This goal was met in 56% of the schools; 64% of the schools had ≥40 child/parent dyads. Sociodemographic data were collected on a sample of 1326 students. After accounting for missing data, a sample size of 1231 consisting of complete data was used for all analyses. Outcome variables (VP, VE, VI, FI) as well as outcome residuals were assessed for normality using histograms and box plots. Kurtosis and skewness of outcome residuals were also examined. Dependent variables did not violate normality; thus, all variables included in these analyses were normally distributed. Separate linear regression models were run to examine the relations between CCI (independent variable) and VP, VE, and VI (dependent variables). A priori covariates for all analyses included: TGEG treatment group, age, sex, and race/ethnicity. SPSS Statistics for Macintosh, Version 25.0 (IBM Corp.) was used for all analyses. A Bonferroni correction post hoc analysis for all dependent variables was conducted to account for multiple comparisons and an adjusted P value of P = 0.0125 was used to denote significance.
Results
Demographic information, anthropometrics and BMI status, VI, FI, VP and exposure scores, and CCI at baseline are presented in Table 2. Study participants were 49% male and 43% Hispanic with an average age of 8.3 y, and 49% of the participants had overweight or obesity.
TABLE 2.
Texas, Grow! Eat! Go! Child baseline characteristics1
| Characteristics | Total (%) or mean ± SD |
|---|---|
| Demographics | |
| Male | 603 (49.0) |
| Age, y | 8.3 ± 0.6 |
| Free/reduced lunch | 700 (56.9) |
| Race/ethnicity2 | |
| Hispanic | 502 (42.8) |
| White | 233 (19.9) |
| African American | 205 (17.5) |
| Other3 | 232 (19.8) |
| Anthropometrics | |
| Height, cm | 132.6 ± 6.5 |
| Weight, kg | 34.1 ± 9.8 |
| BMI, kg/m2 | 19.3 ± 4.3 |
| Overweight or obese, ≥85th percentile | 598 (48.6) |
| Dietary intake and preference | |
| Vegetable intake, times/d | 2.6 ± 2.5 |
| Fruit intake, times/d | 2.7 ± 1.9 |
| Vegetable preference | 8.9 ± 4.1 |
| Vegetable exposure | 12.3 ± 4.0 |
| Child Cooking Involvement | |
| Never or almost never | 235 (18.2) |
| Sometimes | 577 (44.8) |
| Almost always or always | 477 (37.0) |
Adapted with permission from Evans et al. (BMC Public Health 2016); n = 1231.
Ethnicity, n = 1172.
Other = American Indian or Alaskan Native, Native Hawaiian or Pacific Islander, identifies with >1 race, or Asian (parent-reported).
Table 3 displays linear regression results. Significant associations were found between always cooking with your family and VP, VI, and FI (P = 0.0125 for all models). Compared with children that were never involved in family cooking, children that reported always being involved in family cooking had higher VP (β = 3.26; 95% CI: 1.67–4.86; P < 0.01); higher VE (β = 2.26; 95% CI: 0.67–3.85; P < 0.01); and higher vegetable and fruit consumption (β = 2.45; 95% CI: 1.47–3.44; P < 0.01, and β = 0.93; 95% CI: 0.48, 01.39; P < 0.01, respectively). When a child was sometimes involved in family cooking compared with never being involved in family cooking, VI and fruit consumption were higher (β = 1.47; 95% CI: 0.51, 2.42; P < 0.01, and β = 0.64; 95% CI: 0.20, 1.08; P < 0.01, respectively). Figure 1 depicts the comparison of family cooking and the various vegetables and fruit categories. There were no interaction effects of race/ethnicity or sex with family cooking involvement on any of the dependent variables; therefore, linear regression models were not run on data stratified by race/ethnicity or sex.
TABLE 3.
Linear regression results of main effects and interaction effects of sex, ethnicity, treatment group, and child cooking involvement on vegetable preference, vegetable exposure, vegetable intake, and fruit intake
| Vegetable preference | Vegetable exposure | Vegetable intake | Fruit intake | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | P value1 | B | 95% CI | P value1 | B | 95% CI | P value1 | B | 95% CI | P value1 | |
| Sex | — | — | 0.92 | — | — | 0.34 | — | — | 0.51 | — | — | 0.57 |
| Race/ethnicity2 | — | — | 0.30 | — | — | 0.85 | — | — | 0.31 | — | — | 0.00 |
| Hispanics | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Other | 0.51 | (−0.49, 1.51) | 0.32 | 0.80 | (−0.20, 1.80) | 0.12 | 0.31 | (−0.31, 0.92) | 0.33 | 0.20 | (−0.80, 0.17) | 0.10 |
| African Americans | 0.36 | (−0.59, 1.31) | 0.46 | 0.14 | (−0.81, 1.09) | 0.78 | 0.02 | (−0.57, 0.61) | 0.95 | 0.06 | (−0.70, 1.62) | 0.20 |
| White | −0.63 | (−1.70, 0.44) | 0.28 | 0.40 | (−0.66, 1.47) | 0.46 | −0.46 | (−1.12, 0.20) | 0.17 | −0.19 | (0.29, 0.67) | 0.41 |
| TGEG treatment3 | — | — | 0.23 | — | — | 0.85 | — | — | 0.65 | — | — | 0.43 |
| Family cooking | — | — | <0.01 | — | — | <0.01 | — | — | <0.01 | — | — | <0.01 |
| Never | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Sometimes | 1.61 | (0.07, 3.15) | 0.04 | 1.47 | (−0.70, 3.00) | 0.06 | 1.47 | (0.51, 2.42) | <0.01 | 0.64 | (0.20, 1.08) | <0.01 |
| Always | 3.26 | (1.67, 4.86) | <0.01 | 2.26 | (0.67, 3.85) | <0.01 | 2.45 | (1.47, 3.44) | <0.01 | 0.93 | (0.48, 1.39) | <0.01 |
| Race/ethnicity × CCI interaction | — | — | 0.17 | — | — | 0.17 | — | — | 0.42 | — | — | 0.62 |
| Sex × CCI interaction | — | — | 0.56 | — | — | 0.26 | — | — | 0.83 | — | — | 0.78 |
Post hoc analysis Bonferroni correction adjusted P values to determine statistical significance for dependent variables (P = 0.0125); significant P values (<0.0125) are bolded.
Ethnicity: 1) Other (which includes the following: American Indian or Alaskan Native, Native Hawaiian or Pacific Islander, Other, identifies with >1 race, and Asian), 2) African American, 3) White, and 4) Hispanic.
TGEG treatment included 4 treatment groups: 1) Coordinated School Health (CSH) only (control group), 2) CSH plus gardening and nutrition intervention (Learn! Grow! Eat! Go! or LGEG group), 3) CSH plus physical activity intervention (Walk Across Texas or WAT group), and 4) CSH plus LGEG plus WAT (combined group).
95% CI, 95% confidence interval; B, Beta Statistic, CCI, child cooking involvement; Ref, reference group; TGEG, Texas, Grow! Eat! Go!
FIGURE 1.
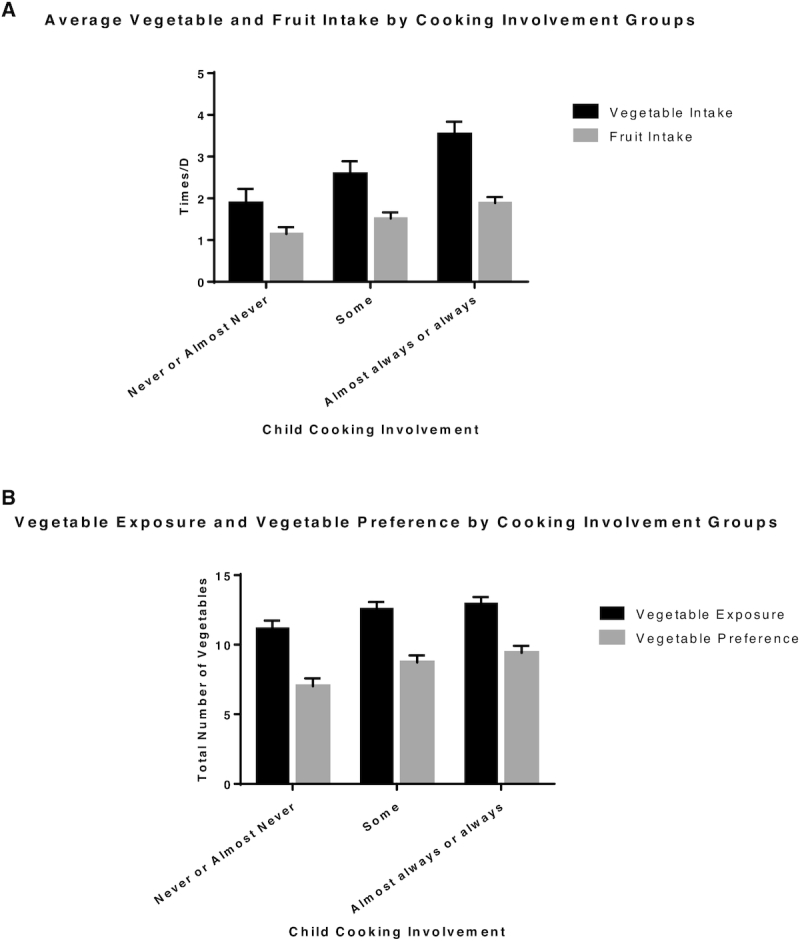
(A) Comparison of child cooking involvement groups with average vegetable intake and average fruit intake; (B) comparison of child cooking involvement groups with vegetable exposure and vegetable preference.
Discussion
Our results showed a positive association between children who prepared food with their families and FV consumption, demonstrating that this may be an effective strategy to improve dietary intake of healthy foods in this high-risk population. Studies have shown the link between exposure to a food and preference for that food; thus, improving a child's willingness to taste a vegetable as well as improving their preferences for that vegetable are crucial steps in getting children to consume more vegetables (18, 19).
School-based cooking interventions show promise in raising parental awareness about healthy foods and encouraging parents to make meals with their children at home (29). One study from Switzerland, randomly assigned 47 children (aged 6–10 y) to either the “child cooks” condition, where the child helped the parent prepare a lunch meal, or the “parent cooks” condition, where the parent cooked alone, but the lunch meal was identical. Results showed that children in the “child cooks” condition ate 76% more salad at the subsequent meal than children in the “parent cooks” condition (19). Similarly, a study conducted with 3398 5th grade children found that children who were more involved in preparing meals at home with their parents compared with those not involved ate an additional serving of fruits and vegetables (36). These results are consistent with the findings of the present study, demonstrating that children cooking with their parents at home had higher intakes of FV. The aforementioned studies also highlight the importance of parental involvement, as parental involvement plays a key role in influencing the FV consumption of their children (29). A systematic review examining the influence of gardening interventions on FV consumption found that increases in FV consumption were not consistently found among the 13 review studies (37–49). The review surmised that perhaps the lack of access to FV in the home may have resulted in no intervention effects on FV consumption and suggested that future garden interventions for children may benefit from adding a parental component (8).
The mechanism by which cooking increases child FV intake can be explained by cognitive factors such as attitudes and self-efficacy. Cooking interventions have been shown to significantly increase attitudes towards cooking and self-efficacy (22, 30, 50). Increases in food preparation have also been linked to greater fruit and VP and self-efficacy for cooking and healthy eating (36, 51). Another factor influencing a child's food choice is parental modeling. Parents play a critical role in determining what their child eats, and parental behaviors such as making healthful options like fruits and vegetables available at home as well as preparing meals together with their children (29) have been linked to improvements in children's dietary intake. Mothers are often presumed to be the nutritional gatekeepers of the home environment; however, studies have found that fathers also play a role in the nutritional content of foods in the home (52, 53). Developing a deeper understanding of the role both parents play in improving a child's dietary intake and the interplay of psychosocial factors on improving a child's dietary intake is warranted.
Cooking interventions are gaining popularity as a means to get children in the kitchen and subsequently improve their dietary intake, but the components and strategies used in these interventions vary widely. Sometimes the children are taught food preparation skills in a hands-on fashion and sometimes children watch cooking demonstrations. Because cooking with children can be laborious as well as quite costly, the cooking component tends to be watered down when interventions are scaled up (54). Our findings suggest that hands-on cooking and involvement in food preparation are associated with higher FV intake, indicating that cooking should be a primary focus of future interventions that target improving dietary intake in children, despite the potential cost and labor intensiveness. Our study also highlights the importance of parental involvement in cooking interventions, as this critical component should not be overlooked when developing such programs.
This study has a few limitations that need to be addressed. The dietary behaviors of participants were assessed using a questionnaire that only asked about foods eaten “yesterday.” The potential problem exists that the previous day's intake is not reflective of a child's overall dietary intake. Also, the young age of the students poses the potential issue of a lack of reading comprehension and full understanding of the questions being asked (55–57). However, survey questions were field tested in the target population. Response bias may have also been an additional limitation of this study. Socially desirable response (SDR) or providing responses to present oneself in a more “healthy” image has been found in dietary intake research (58, 59). In an effort to reduce any potential SDR and limit the impact of overreporting “healthier” foods on the results, this study used the following recommended procedures of: 1) protecting respondent anonymity, 2) assuring respondents that there were no right or wrong answers to the survey questions, and 3) asking respondents to answer all survey questions as truthfully as possible (60).
Children do not eat enough fruits and vegetables, which are essential to health and the prevention of disease (10, 13). Thus, it is important to determine the most effective ways to increase FV consumption. It is especially critical to improve FV intake in high-risk, low-income populations, as these children are at a disproportionately higher risk of developing obesity and obesity-related diseases. This study shows that involving high-risk, minority children in food preparation at home may be positively associated with the intake of fruits and vegetables as well as willingness to try and preference for vegetables. Since home meal preparation is inversely associated with per capita food expenses, cooking at home is a feasible strategy to improve dietary intake without increasing expenses for low-income, Hispanic families (27). Further interventions that target parents and children cooking together at home, especially in Hispanic and/or low-income populations are warranted.
ACKNOWLEDGEMENTS
The authors’ contributions were as follows—NR, JW, and AVB: designed and conducted the research; FMA: performed statistical analyses and interpreted results; JND: assisted with statistical analyses; FMA, JND, and AKM: primarily drafted the manuscript; FMA, JND, AKM, MJL, SV, RG, NR, JW, and AVB: had primary responsibility for final content; and all authors read and approved the final manuscript.
Notes
Texas, Grow! Eat! Go! was funded by the Agriculture and Food Research Initiative, (grant 2011-68001-30138) from the USDA National Institute of Food and Agriculture, Integrated Research, Education, and Extension to Prevent Childhood Obesity, with partial funding from the Michael & Susan Dell Foundation through the Michael & Susan Dell Center for Healthy Living, The University of Texas School of Public Health, Austin Regional Campus.
Author disclosures: The authors report no conflicts of interest.
Abbreviations used: CATCH, Coordinated Approach to Child Health; CCI, child cooking involvement; CSH, Coordinated School Health; FI, fruit intake; FV, fruit and vegetable; LGEG, Learn, Grow, Eat & Go!; RCT, randomized controlled trial; SDR, socially desirable response; SES, socioeconomic status; TGEG, Texas, Grow! Eat! Go!; T2D, type 2 diabetes; VE, vegetable exposure; VI, vegetable intake; VP, vegetable preference; WAT, Walk across Texas.
References
- 1. Ogden CL, Carroll MD, Lawman HG, Fryar CD, Kruszon-Moran D, Kit BK, Flegal KM. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. JAMA. 2016;315:2292–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Goran MI, Walker R, Le K-A, Mahurkar S, Vikman S, Davis JN, Spruijt-Metz D, Weigensberg MJ, Allayee H. Effects of PNPLA3 on liver fat and metabolic profile in Hispanic children and adolescents. Diabetes. 2010;59:3127–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Davis JN, Martinez LC, Spruijt-Metz D, Gatto NM. LA Sprouts: a 12-week gardening, nutrition, and cooking randomized control trial improves determinants of dietary behaviors. J Nutr Educ Behav. 2016;48:2–11. e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Frederick CB, Snellman K, Putnam RD. Increasing socioeconomic disparities in adolescent obesity. Proc Natl Acad Sci. 2014;111:1338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, Wei R, Curtin LR, Roche AF, Johnson CL. 2000. CDC growth charts for the United States; methods and development. Vital Health Stat 11. 2002;246:1–190. [PubMed] [Google Scholar]
- 6. Daniels SR, Arnett DK, Eckel RH, Gidding SS, Hayman LL, Kumanyika S, Robinson TN, Scott BJ, St. Jeor S, Williams CL. Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation. 2005;111:1999–2012. [DOI] [PubMed] [Google Scholar]
- 7. Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. 1998;101:518–25. [PubMed] [Google Scholar]
- 8. Savoie-Roskos MR, Wengreen H, Durward C. Increasing fruit and vegetable intake among children and youth through gardening-based interventions: a systematic review. J Acad Nutr Diet. 2017;117:240–50. [DOI] [PubMed] [Google Scholar]
- 9. He K, Hu FB, Colditz GA, Manson JE, Willett WC, Liu S. Changes in intake of fruits and vegetables in relation to risk of obesity and weight gain among middle-aged women. Int J Obes. 2004;28:1569–74. [DOI] [PubMed] [Google Scholar]
- 10. Boeing H, Bechthold A, Bub A, Ellinger S, Haller D, Kroke A, Leschik-Bonnet E, Müller MJ, Oberritter H, Schulze M et al.. Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr. 2012;51:637–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Cooper AJ, Sharp SJ, Lentjes MAH, Luben RN, Khaw K-T, Wareham NJ, Forouhi NG. A prospective study of the association between quantity and variety of fruit and vegetable intake and incident type 2 diabetes. Diabetes Care. 2012;35:1293–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Cook LT, O'Reilly GA, Goran MI, Weigensberg MJ, Spruijt-Metz D, Davis JN. Vegetable consumption is linked to decreased visceral and liver fat and improved insulin resistance in overweight Latino youth. J Acad Nutr Diet. 2014;114:1776–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Namenek Brouwer RJ, Benjamin Neelon SE. Watch me grow: a garden-based pilot intervention to increase vegetable and fruit intake in preschoolers. BMC Public Health. 2013;13:363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kratt P, Reynolds K, Shewchuk R. The role of availability as a moderator of family fruit and vegetable consumption. Health Educ Behav. 2000;27:471–82. [DOI] [PubMed] [Google Scholar]
- 15. Kim SA, Moore LV, Galuska D, Wright AP, Harris D, Grummer-Strawn LM, Merlo CL, Nihiser AJ, Rhodes DG. Vital signs: fruit and vegetable intake among children – United States, 2003–2010. Morb Mortal Wkly Rep. 2014;63:671–6. [PMC free article] [PubMed] [Google Scholar]
- 16. Dave JM, Evans AE, Saunders RP, Watkins KW, Pfeiffer KA. Associations among food insecurity, acculturation, demographic factors, and fruit and vegetable intake at home in Hispanic children. J Am Diet Assoc. 2009;109:697–701. [DOI] [PubMed] [Google Scholar]
- 17. Bere E, Klepp K-I.. Changes in accessibility and preferences predict children's future fruit and vegetable intake. Int J Behav Nutr Phys Act. 2005; ;2:15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Kirby SD, Baranowski T, Reynolds KD, Taylor G, Binkley D. Children's fruit and vegetable intake: socioeconomic, adult-child, regional, and urban-rural influences. J Nutr Educ. 1995;27:261–71. [Google Scholar]
- 19. Birch LL, Marlin DW. I don't like it; I never tried it: effects of exposure on two-year-old children's food preferences. Appetite. 1982;3:353–60. [DOI] [PubMed] [Google Scholar]
- 20. Fildes AMA, van Jaarsveld CHM, Wardle J, Cooke L. Parent-administered exposure to increase children's vegetable acceptance: a randomized controlled trial. J Acad Nutr Diet. 2014;114:881–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Caraher M, Seeley A, Wu M, Lloyd S. When chefs adopt a school? An evaluation of a cooking intervention in English primary schools. Appetite. 2013;62:50–9. [DOI] [PubMed] [Google Scholar]
- 22. Cunningham-Sabo L, Lohse B.. Cooking with Kids positively affects fourth graders' vegetable preferences and attitudes and self-efficacy for food and cooking. Child Obes. 2013;9:549–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Morris JL, Zidenberg-Cherr S.. Garden-enhanced nutrition curriculum improves fourth-grade school children's knowledge of nutrition and preferences for some vegetables. J Am Diet Assoc. 2002;102:91–3. [DOI] [PubMed] [Google Scholar]
- 24. Hyland R, Stacy R, Adamson A, Moynihan P. Nutrition-related health promotion through an after-school project: the responses of children and their families. Soc Sci Med. 2006;62:758–68. [DOI] [PubMed] [Google Scholar]
- 25. van der Horst K, Ferrage A, Rytz A. Involving children in meal preparation. Effects on food intake. Appetite. 2014;79:18–24. [DOI] [PubMed] [Google Scholar]
- 26. Guo SS, Huang C, Maynard LM, Demerath E, Towne B, Chumlea WC, Siervogel RM. Body mass index during childhood, adolescence and young adulthood in relation to adult overweight and adiposity: the Fels Longitudinal Study. Int J Obes. 2000;24:1628–35. [DOI] [PubMed] [Google Scholar]
- 27. Tiwari AM, Aggarwal A, Tang W, Drewnowski A. Cooking at home: a strategy to comply with U.S. Dietary Guidelines at no extra cost. Am J Prev Med. 2017;52:616–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Brown BJ, Hermann JR.. Cooking classes increase fruit and vegetable intake and food safety behaviors in youth and adults. J Nutr Educ Behav. 2005;37:104–5. [DOI] [PubMed] [Google Scholar]
- 29. Evans A, Ranjit N, Hoelscher D, Jovanovic C, Lopez M, McIntosh A, Ory M, Whittlesey L, McKyer L, Kirk A et al.. Impact of school-based vegetable garden and physical activity coordinated health interventions on weight status and weight-related behaviors of ethnically diverse, low-income students: study design and baseline data of the Texas, Grow! Eat! Go! (TGEG) cluster-randomized controlled trial. BMC Public Health. 2016;16:973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Landry MJ, Markowitz AK, Asigbee FM, Gatto NM, Spruijt-Metz D, Davis JN. Cooking and gardening behaviors and improvements in dietary intake in Hispanic/Latino youth. Child Obes. 2019;15:262–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Evans A, Ranjit N, Fair CN, Jennings R, Warren JL. Previous gardening experience and gardening enjoyment is related to vegetable preferences and consumption among low-income elementary school children. J Nutr Educ Behav. 2016;48:618–24.e1. [DOI] [PubMed] [Google Scholar]
- 32. Coordinated Approach To Child Health (CATCH). [Cited 2019 May 6] [Internet]; Available from: https://sph.uth.edu/research/centers/dell/project.htm?project = eddbb8f0-a00a-4385-8e34-148e1712573c.
- 33. Thiagarajah K, Fly AD, Hoelscher DM, Bai YM, Lo KM, Leone AM, Shertzer JAM. Validating the food behavior questions from the elementary school SPAN questionnaire. J Nutr Educ Behav. 2008;40:305–10. [DOI] [PubMed] [Google Scholar]
- 34. Davis M, Baranowski T, Resnicow K, Baranowski J, Doyle C, Smith M, Wang DT, Yaroch A, Hebert D. Gimme 5 fruit and vegetables for fun and health: process evaluation. Health Educ Behav. 2000;27:167–76. [DOI] [PubMed] [Google Scholar]
- 35. Springer AE, Kelder SH, Ranjit N, Hochberg-Garrett H, Crow S, Delk J. Promoting physical activity and fruit and vegetable consumption through a community-school partnership: the effects of Marathon Kids® on low-income elementary school children in Texas. J Phys Act Health. 2012;9::739–53. [DOI] [PubMed] [Google Scholar]
- 36. Chu YL, Storey KE, Veugelers PJ. Involvement in meal preparation at home is associated with better diet quality among Canadian children. J Nutr Educ Behav. 2014;46:304–8. [DOI] [PubMed] [Google Scholar]
- 37. Davis JN, Ventura EE, Cook LT, Gyllenhammer LE, Gatto NM. LA Sprouts: a gardening, nutrition, and cooking intervention for Latino youth improves diet and reduces obesity. J Am Diet Assoc. 2011;111:1224–30. [DOI] [PubMed] [Google Scholar]
- 38. Brouwer RJN, Neelon SEB.. Watch Me Grow: a garden-based pilot intervention to increase vegetable and fruit intake in preschoolers. BMC Public Health. 2013;13:363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Castro DC, Samuels M, Harman AE. Growing healthy kids: a community garden-based obesity prevention program. Am J Prev Med. 2013;44:S193–S9. [DOI] [PubMed] [Google Scholar]
- 40. Lautenschlager L, Smith C.. Understanding gardening and dietary habits among youth garden program participants using the Theory of Planned Behavior. Appetite. 2007;49:122–30. [DOI] [PubMed] [Google Scholar]
- 41. McAleese JD, Rankin LL.. Garden-based nutrition education affects fruit and vegetable consumption in sixth-grade adolescents. J Am Diet Assoc. 2007;107:662–5. [DOI] [PubMed] [Google Scholar]
- 42. Meinen A, Friese B, Wright W, Carrel A. Youth gardens increase healthy behaviors in young children. J Hunger Environ Nutr. 2012;7:192–204. [Google Scholar]
- 43. Parmer SM, Salisbury-Glennon J, Shannon D, Struempler B. School gardens: an experiential learning approach for a nutrition education program to increase fruit and vegetable knowledge, preference, and consumption among second-grade students. J Nutr Educ Behav. 2009;41:212–7. [DOI] [PubMed] [Google Scholar]
- 44. Wang MC, Rauzon S, Studer N, Martin AC, Craig L, Merlo C, Fung K, Kursunoglu D, Shannguan M, Crawford P. Exposure to a comprehensive school intervention increases vegetable consumption. J Adolesc Health. 2010;47:74–82. [DOI] [PubMed] [Google Scholar]
- 45. Ratcliffe MM, Merrigan KA, Rogers BL, Goldberg JP. The effects of school garden experiences on middle school-aged students’ knowledge, attitudes, and behaviors associated with vegetable consumption. Health Promot Pract. 2011;12:36–43. [DOI] [PubMed] [Google Scholar]
- 46. Christian MS, Evans CE, Nykjaer C, Hancock N, Cade JE. Evaluation of the impact of a school gardening intervention on children's fruit and vegetable intake: a randomized controlled trial. Int J Behav Nutr Phys Act. 2014;11:99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Duncan MJ, Eyre E, Bryant E, Clarke N, Birch S, Staples V, Sheffield D. The impact of a school-based gardening intervention on intentions and behaviour related to fruit and vegetable consumption in children. J Health Psychol. 2015;20:765–73. [DOI] [PubMed] [Google Scholar]
- 48. Clark AM, DesMeules M, Luo W, Duncan AS, Wielgosz A. Socioeconomic status and cardiovascular disease: risks and implications for care. Nat Rev Cardiol. 2009;6:712–22. [DOI] [PubMed] [Google Scholar]
- 49. Hanbazaza MA, Triador L, Ball GD, Farmer A, Maximova K, Nation AF, Willows ND. The impact of school gardening on Cree children's knowledge and attitudes toward vegetables and fruit. Can J Diet Pract Res. 2015;76:133–9. [DOI] [PubMed] [Google Scholar]
- 50. Bisset SL, Potvin L, Daniel M, Paquette M. Assessing the impact of the primary school-based nutrition intervention Petits cuistots–parents en réseaux. Can J Public Health. 2008;99:107–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Woodruff SJ, Kirby AR.. The associations among family meal frequency, food preparation frequency, self-efficacy for cooking, and food preparation techniques in children and adolescents. J Nutr Educ Behav. 2013;45:296–303. [DOI] [PubMed] [Google Scholar]
- 52. Stein RI, Epstein LH, Raynor HA, Kilanowski CK, Paluch RA. The influence of parenting change on pediatric weight control. Obes Res. 2005;13:1749–55. [DOI] [PubMed] [Google Scholar]
- 53. Johannsen DL, Johannsen NM, Specker BL. Influence of parents’ eating behaviors and child feeding practices on children's weight status. Obesity. 2006;14:431–9. [DOI] [PubMed] [Google Scholar]
- 54. Cunningham-Sabo L, Lohse B.. Cooking with Kids positively affects fourth graders' vegetable preferences and attitudes and self-efficacy for food and cooking. Childhood Obesity (Print). 2013;9:549–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Livingstone MBE, Robson P, Wallace J. Issues in dietary intake assessment of children and adolescents. Br J Nutr. 2004;92:S213–S22. [DOI] [PubMed] [Google Scholar]
- 56. Magarey A, Watson J, Golley RK, Burrows T, Sutherland R, Mcnaughton SA, Denney-Wilson E, Campbell K, Collins C. Assessing dietary intake in children and adolescents: considerations and recommendations for obesity research. Int J Pediatr Obes. 2011;6:2–11. [DOI] [PubMed] [Google Scholar]
- 57. Walker JL, Ardouin S, Burrows T. The validity of dietary assessment methods to accurately measure energy intake in children and adolescents who are overweight or obese: a systematic review. Eur J Clin Nutr. 2018;72:185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Scagliusi FB, Polacow VO, Artioli GG, Benatti FB, Lancha AH Jr.. Selective underreporting of energy intake in women: magnitude, determinants, and effect of training. J Am Diet Assoc. 2003;103:1306–13. [DOI] [PubMed] [Google Scholar]
- 59. Tooze JA, Subar AF, Thompson FE, Troiano R, Schatzkin A, Kipnis V. Psychosocial predictors of energy underreporting in a large doubly labeled water study. Am J Clin Nutr. 2004;79:795–804. [DOI] [PubMed] [Google Scholar]
- 60. Podsakoff PM, MacKenzie SB, Lee J-Y, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88:879–903. [DOI] [PubMed] [Google Scholar]