
eFigure 33-29.
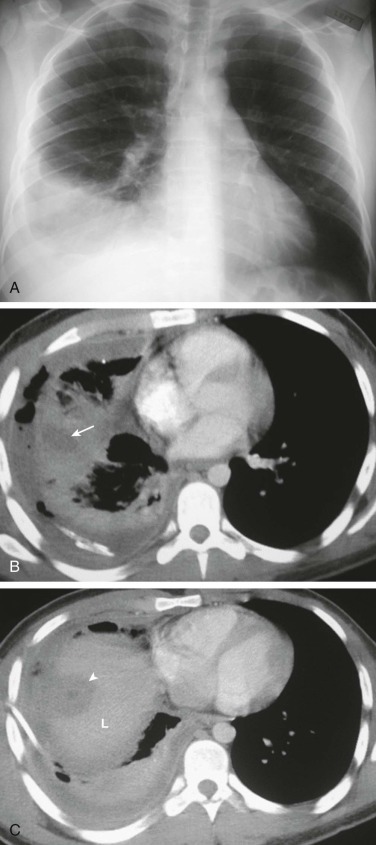
An infectious cause of “nonresponding” pneumonia: amebic pleuropulmonary infection.
A, Frontal chest radiograph in a 23-year-old man with fever and chest pain shows right lower lobe consolidation and a small-to-moderate right pleural effusion, presumed to represent pneumonia and parapneumonic effusion. B and C, Axial chest CT after the patient failed to respond to therapy for community-acquired pneumonia was performed to assess right pleural fluid drainage following thoracostomy tube placement (the thoracostomy tube is visible posteriorly in B). Chest CT performed through the right lower lung (B) shows consolidation with central low-attenuation (arrow), the latter consistent with a pulmonary abscess or area of necrosis. Chest CT through the extreme lung base and upper abdomen (C) shows a low attenuation focus (arrowhead) in the cranial liver (L), also consistent with an abscess. The liver and lung lesions are in close proximity to one another, suggesting that the liver lesion may have extended through the diaphragm to produce the lung findings; such behavior is typical of an amebic abscess. Further evaluation revealed that the patient recently immigrated to the United States from Mexico, and stool analysis recovered Entamoeba histolytica trophozoites.
(Courtesy Michael Gotway, MD.)