

Summary
In Switzerland ‘Secret’ is a folk medicine called upon for burns. It has belonged to UNESCO’s intangible cultural heritage since 2012. It is supposed to ease pain and accelerate the healing process of burns. As the practice is widely used in the population, this observational study investigated the opinion of caregivers and patients from the National Burn Center of Lausanne. Qualitative observational study based on a survey including ten questions aimed at identifying the professionals’ perception of the phenomenon. Questions were developed from repeated encounters in the burn center. Data collection took five months. Thirty-six healthcare professionals (HP) and 12 selected patients (or parents for minors) discharged after burns were interviewed on a voluntary basis: all of the HPs knew about ‘Secret’ from the workplace, and 26 from home: 33 were convinced that it might be useful and reduce pain. The perceived efficiency of the practice (36 respondents) differs depending on professional category and personal experience. Only one HP considered the practice to be dangerous. The nurses and auxiliary nurses expressed that it should be used more widely. The 12 patients considered it as a complementary step, not a replacement for medical care. Health professionals globally considered this practice safe and helpful. The patients were interested in using parallel approaches and were careful about their expectations. This openness is probably an indication that HPs believe that acceptance of the culture and beliefs of patients and their families might positively affect response to treatment, whatever the burn size.
Keywords: folk medicine, burn care, pain management
Abstract
Il existe en Suisse une médecine traditionnelle dénommée « secret » dédiée aux brûlures (supposée avoir des effets analgésiques et cicatrisants) inscrite au patrimoine immatériel de l’UNESCO depuis 2012. Dans la mesure où elle est très largement utilisée, nous avons conduit une étude observationnelle sur l’opinion qu’en ont les soignants et les patients du CTB national de Lausanne. Nous avons utilisé un questionnaire à dix items, développé après des entretiens plus informels. Trente six professionnels et 12 patients (ou parents quand le patient était mineur), interrogés après leur sortie, ont volontairement participé à l’étude. Tous les professionnels avaient entendu parler de « secret » soit au travail soit chez eux (26). Trente trois étaient persuadés de son utilité analgésique, 1 seul le considérant comme dangereux. Cette opinion varie selon la catégorie professionnelle et l’expérience personnelle, les infirmières et aide- soignantes estimant qu’il devrait être plus largement utilisé. Les patients estimaient que « secret » était un adjuvant ne devant pas remplacer la prise en charge médicalisée. Les professionnels considéraient que « secret » est simple et utile. Les patients étaient intéressée par cette approche parallèle, tout en gardant une certaine retenue quant à ce qu’ils pouvaient en attendre. Cette ouverture d’esprit suggère que les professionnels pensent que la prise en compte de la culture et des croyances des patients et de leur famille peut promouvoir l’efficacité du traitement conventionnel, quelle que soit la surface brûlée.
Introduction
Alternative medicine options are popular in Switzerland, mainly because patients appreciate a global, holistic approach complementary to traditional medicine for their treatment plans and rehabilitation. Many patients that have been treated in the Burn Centre of the CHUV, which admits approximately 200 patients per year, have contacted alternative medical practices for healing, without any exact data being available. Following a positive popular ballot about complementary medical practice acceptance by insurers in Switzerland (2009), the Lausanne Faculty of Biology and Medicine introduced a course on alternative medical practices into the core teaching. In 2012, the use of this Folk Medicine was registered in the UNESCO Intangible Cultural Heritage List which was submitted by two Swiss States, Fribourg and Jura.1,2 It is more openly discussed and debated in the French-speaking western part of Switzerland ranging from Delémont in the Jura to Geneva, including Fribourg and Valais. Now that this phenomenon is more openly discussed, other neighbouring countries such as France and Italy are gently emerging with anecdotes of their own experiences.
In French these healers are known as the “faiseurs de Secret” (‘Secret Makers’), and by various other names, such as “barreurs de feu”, “panseurs de Secret” and “coupeurs de feu” (in English these would translate to ‘barriers against fire’, ‘Secret healers’, and ‘fire cutters’ respectively).1 The fact that they are categorized as ‘healers’ implies that they do not have diplomas for their art and there is no organisation or association established to control or validate their procedures. In general, these people are considered to have a gift that was transmitted to them, and they want to help others freely. These healers are of all ages but more often 50 years old or above, from all regions, even though rural regions seem to have a more authentic connotation. They can either perform the healing technique as a classical consultation, or simply by telephone. They are not paid, however they appreciate simple thank you gestures and updates on the outcome of their patients following any intervention. Even though this altruism is inspired by Christian practices and association with Saints, it is not necessarily related to religious beliefs. Moreover, the Catholic Church disapproves of healers using prayers and that this practice is not strictly performed by clergy members.
Secrets are formulas or prayers that have to be repeated with a certain intention. Multiple pathologies are involved, such as warts, muscle strain, sciatic nerve, migraine, eczema, psoriasis, zooster, earache, angina, stress, hemorrhoids, hemorrhages and burns: there is even a free app with direct access to the list of “Secret Healers” in Switzerland and France.3 Several prayers for burns have been published, one by the Abbé Julio in 1907 (St. Maurice, Valais, Switzerland),4 and another more thorough one by Derivaz and Clerc in 2014.5
The aim of this observational study was to investigate the opinion and degree of acceptation for this practice by medical staff and patients in the Hospital.
Methods
The interviews were based on a survey that was created by the authors, not validated by any authority, as no such investigation has yet been carried out to our knowledge. It was based on informal discussions, and addressed the worries that had been raised previously in the Centre. Informed consent was waived by the Ethics Committee, considering the absence of any medical information and the type of questions, and the fact that the participants were free to answer or refuse to participate.
Participants
Healthcare professionals (HPs) were selected on a voluntary participation basis. The study benefited from the support of the head-nurses and the medical doctors (MDs) from both the Intensive Care (hereafter “ICU”) and Plastic, Reconstructive and Hand Surgery (hereafter “Plastics”) services. The inclusion criterion for the professionals was their employment for at least six months in one of the two services. Patients were selected by WR and AdBR from the ambulant consultation of the plastic surgery follow-up of burn patients, based on their interest in the question and their free will to participate. The inclusion criteria were that they had a previous stay in the burn centre, a minimum of 15 years of age and were able to speak French, German or English and remember their experience in burn care. Two parents of burned children were included because their child was underage.
Questionnaire
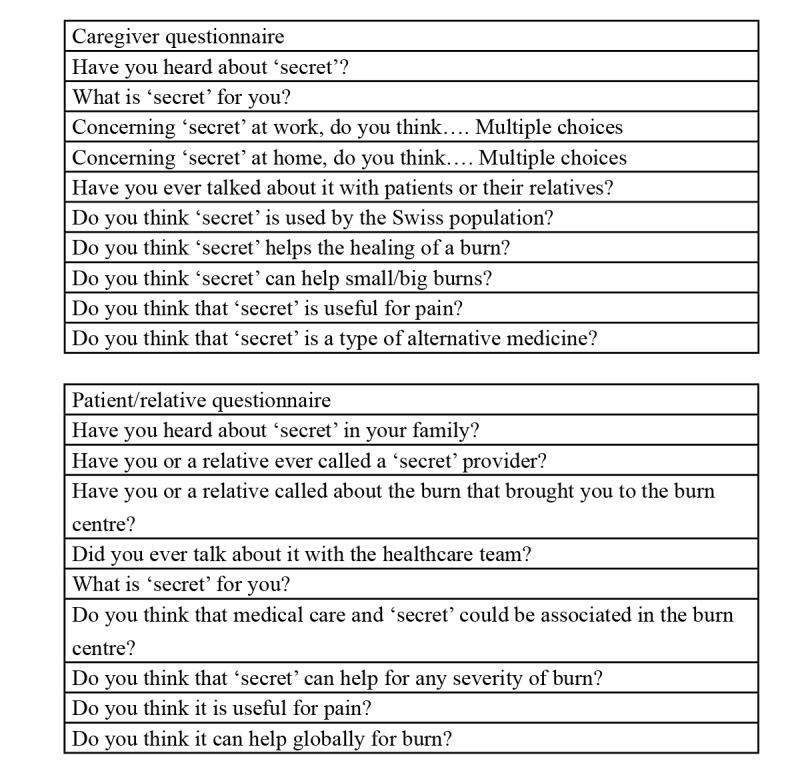
(Table I) shows the questions that the healthcare professionals and patients were asked. The questionnaire aimed to collect the opinion of the participants, as well as their knowledge and expectations. The surveys were used as a basis for a semi-structured interview with each subject, all conducted by the same person. These interviews, conducted face-toface (with professionals) or over the phone (with patients), contained the same further explanations for each question and exploitation of more in-depth questions. Each interview lasted 20 minutes for healthcare professionals and 10 minutes for patients.
Statistical analysis
The answers to direct questions were given scores and summarized. Fisher test was used to analyze categorical variables. We considered a p value <0.05 as significant.
Table I. Questions asked to professionals and to patients.
Results
This study was carried out between November 2013 and March 2014. Two additional patient interviews were conducted in March 2018. The data are presented with the number of positive responses to each of the questions. Results of interviews with the healthcare professionals were also subdivided into subgroups to have a better perception of the diversity (profession, sex and nationality).
Healthcare professionals
Altogether 36 HPs agreed to participate: 47 professionals either refused, were absent, or had not worked long enough to participate (13 in Plastic and 34 in the ICU). The professionals included 11 MDs, 14 nurses, 5 physiotherapists and 6 auxiliary nurses of different nationalities (Table II). Of these, 25 were Swiss citizens, while the others were 10 European Union citizens and one Canadian. All the HPs were already aware of ‘Secret’ in their work experience, but only 26 had heard of it through family and friend circles. Moreover, 33 of the HPs thought that the use of ‘Secret’ is useful, useful meaning serving some intended purpose (Fig. 1). A total of 33 also believed that this practice helps reduce pain.
Table II. Characteristics of the health professional survey participants.
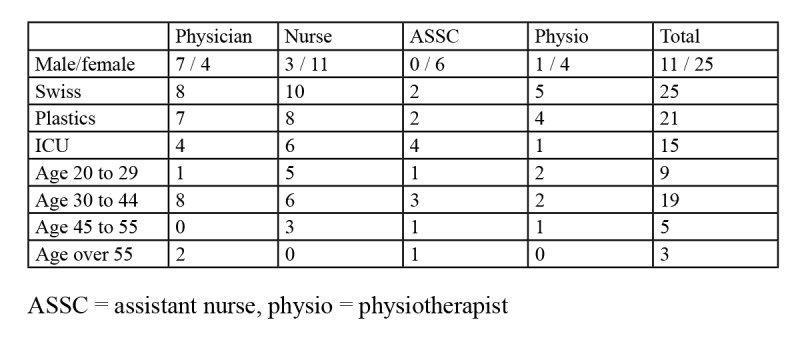
Fig. 1A. Professional opinion on the general usefulness of ‘Secret’.
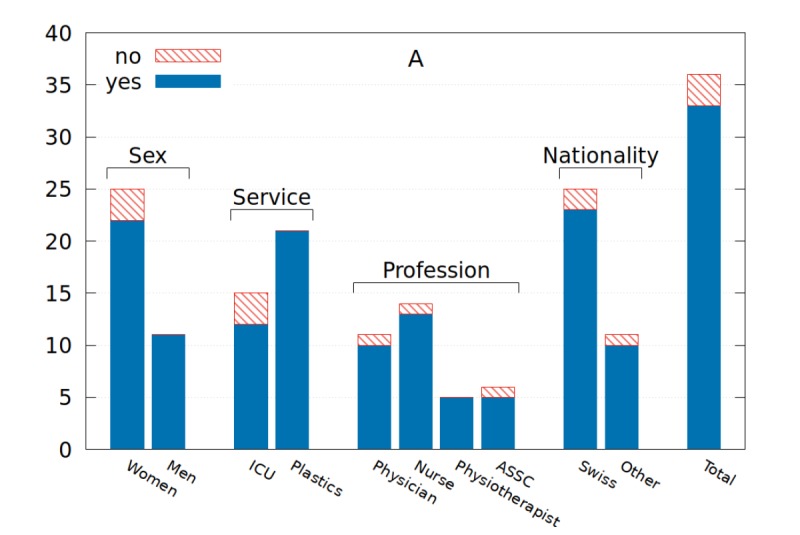
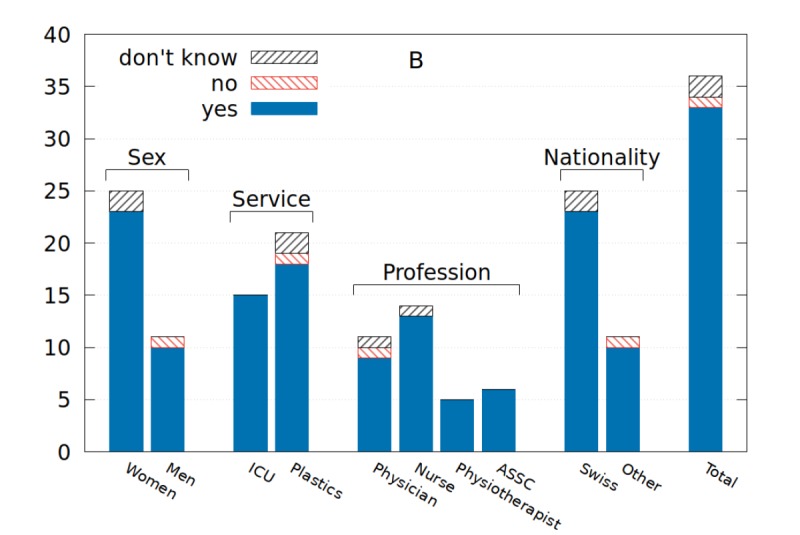
Fig. 1B. Personal opinion on the general usefulness of ‘Secret’.

Regarding efficacy, meaning the ability to produce a result, in their professional environment 25 HPs thought that it was efficient, but perception differed by service: 17/21 (81%) of the Plastics were positive compared to only 7/11 (64%) in the ICU (Fig. 2).
Fig. 2A. Professional opinion on the general efficacy of ‘Secret’.
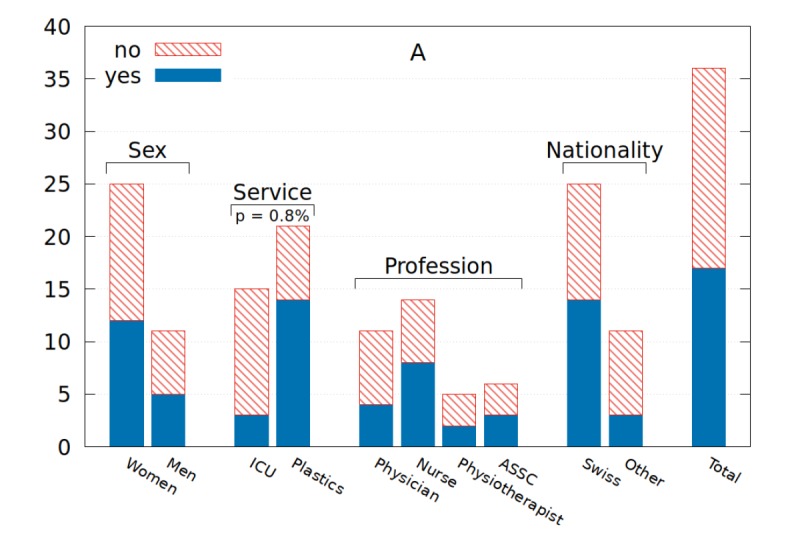
Fig. 2B. Personal opinion on the general efficacy of ‘Secret’.
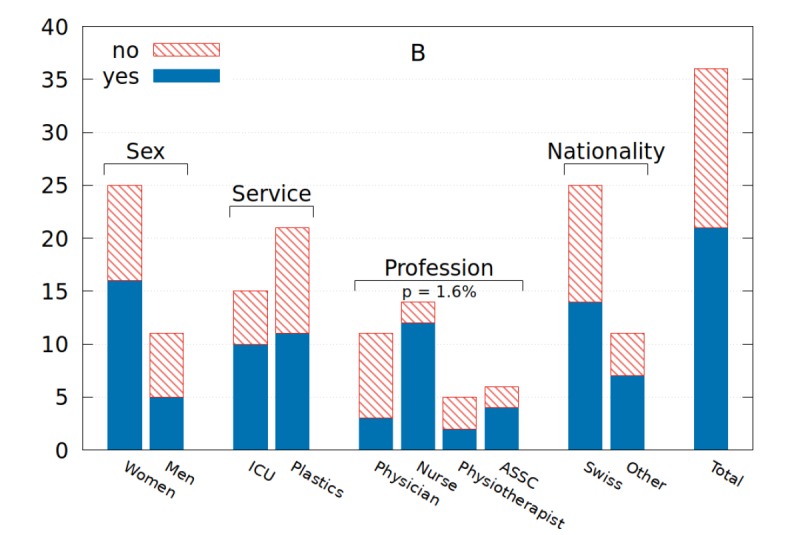
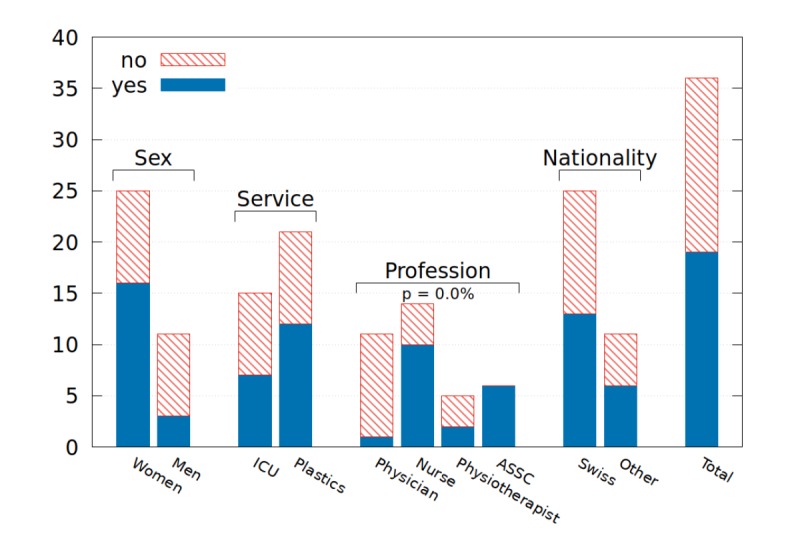
If we consider potential benefits by burn size, 26 of the HPs thought that the effect might be strongest on small burns compared to 12 for large surface burns (Fig. 3). There was a significant difference (p=0.013) in opinion among the professions: only 4/11 MDs responded positively compared to 22/25 other professionals. When asked if ‘Secret’ had no effect, only four out of the 36 HPs (3 MDs, 1 nurse) replied that there was no real effect (p= 0.025) (Fig. 4).
Fig. 3A. Caregiver opinion on the efficacy of ‘Secret’ according to the size of the burn: (A) small.
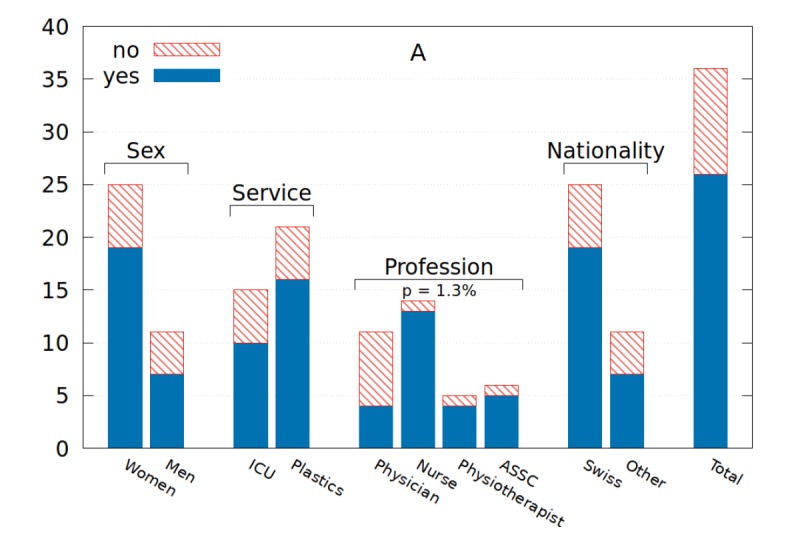
Fig. 3B. Caregiver opinion on the efficacy of ‘Secret’ according to the size of the burn: (B) large.
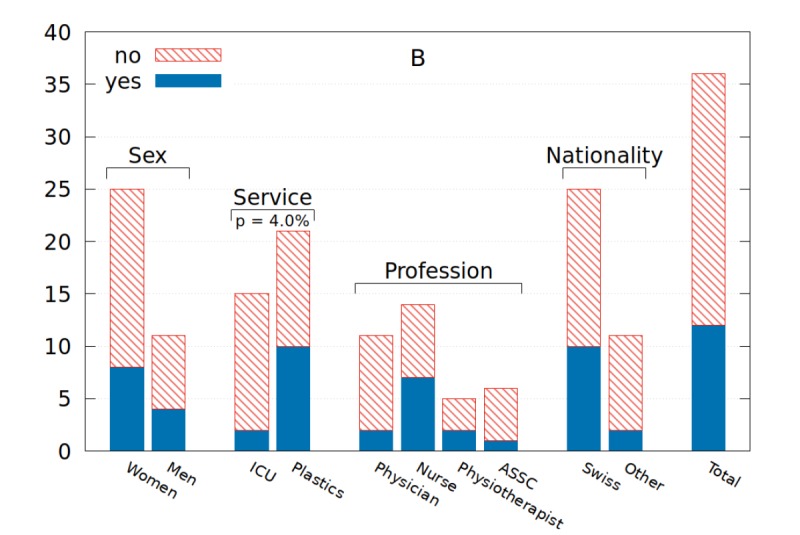
Fig. 4A. Professional opinion on the absence of effect.
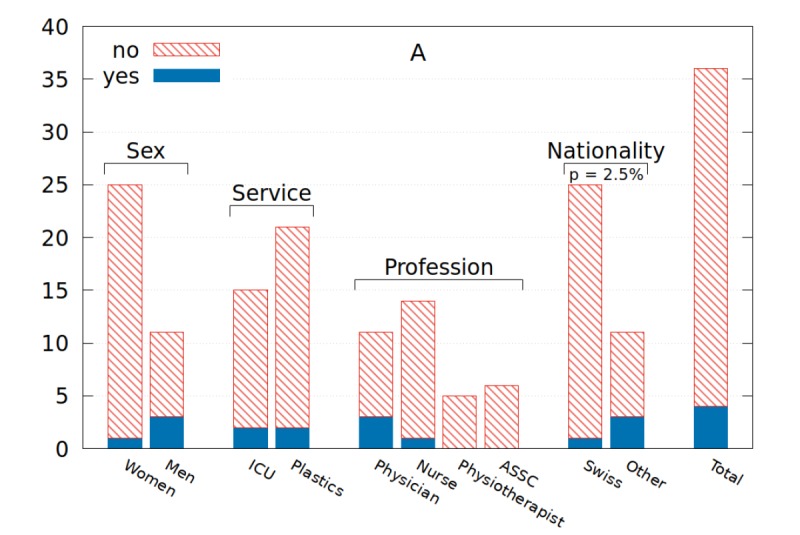
Fig. 4B. Personal opinion on the absence of effect.
Utility questions were broken down as follows: 1) Does ‘Secret’ help the overall healing of the burn? 2) Does ‘Secret’ help the patient with burn pain management? Fourteen HPs thought that ‘Secret’ would aid healing, and nine didn’t know (Fig. 5A). A large number (33 HPs) thought that ‘Secret’ was very useful for pain management with no difference between groups (Fig. 5B).
Fig. 5A. Professional opinion on ‘Secret’ helping: (A) the overall healing process.
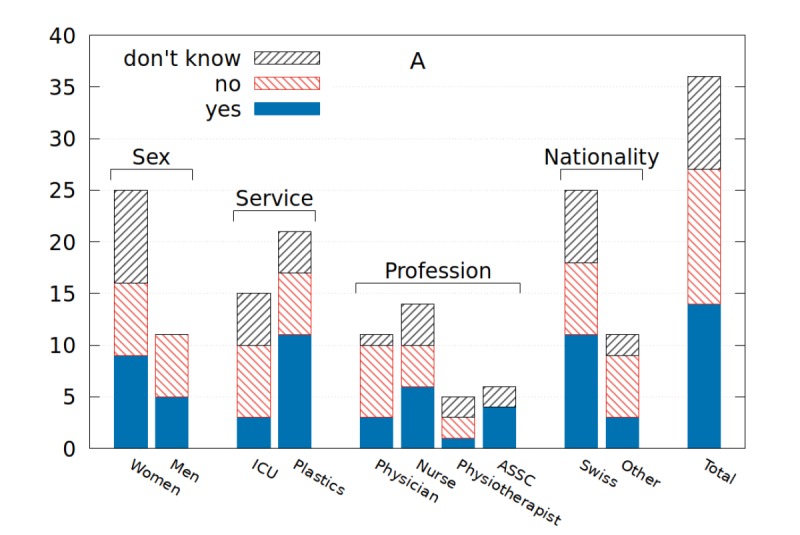
Fig. 5B. Professional opinion on ‘Secret’ helping: (B) patient pain management.
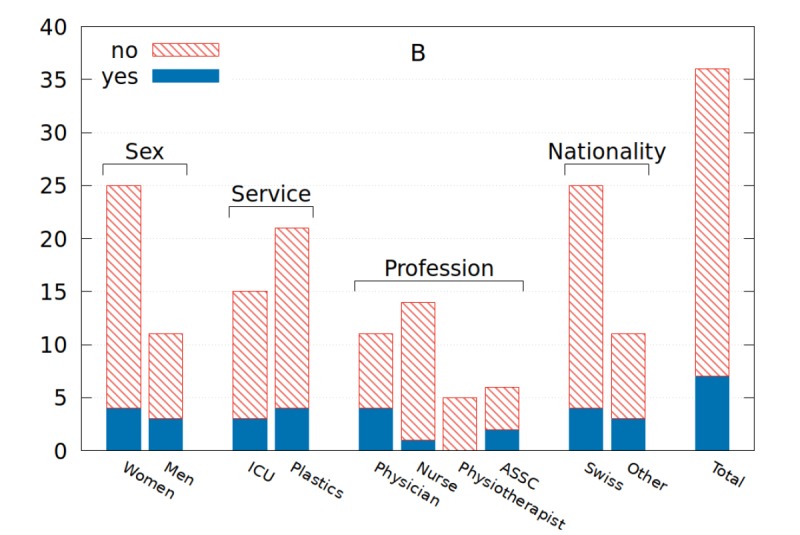
When HPs were asked whether ‘Secret’ helps to keep hope, 31 were positive. Twenty-four of the HPs thought that allowing the use of ‘Secret’ helped to integrate the family in the overall health care process and treatment progression of the patient. Thirty-one of the healthcare professionals believed this was related to cultural tradition (data not shown). Only one HP thought the practice was dangerous (Fig. 6), with nine stating that it should remain outside of the hospital setting: there was a strong difference of opinion between men and women on this question, seven out of 11 men and two out of 25 women (p = 0.01). Along the same lines, 19 HPs thought that ‘Secret’ should be used on a larger scale (Fig. 7). There was an important difference of opinion on this question between men and women, with seven out of 11 men replying positively, and only two out of 25 women. Eighteen of all the interviewed HPs believed that this practice is widely used when one of their family members or acquaintances has been involved in a burn accident. It was reported that 23 HPs had discussed this subject with their patients and families, and it was not usually them that introduced the subject into the discussion.
Fig. 6A. Professional opinion on the dangerousness of the use of ‘Secret’.

Fig. 6B. Personal opinion on the dangerousness of the use of ‘Secret’.

Fig. 7. Professional opinion on whether ‘secret’ should be used more often.
Patients and relatives
The 12 patients and relatives (eight men, four women, all < 65 years) included in the study were all Swiss. Eleven of them had called upon ‘Secret’ following burn injuries that had led them to the Burn Center. One patient had to be excluded from the interviews due to language incompatibility. Six patients had discussed this intervention with the healthcare professionals and two of these had appreciated the possibility to discuss it more in detail during their treatment. When asked about pain management, six patients thought the use of ‘Secret’ helped diminish their pain and five thought it helped the overall efficacy of healing of their burn.
When asked about the overall benefits of this practice, half of the patients/relatives thought that there was a good global effect on burn wound healing and half did not have an opinion on the matter. We asked if the patients thought that ‘Secret’ might be useful on a smaller or larger burn wound: 8/12 thought that it was effective for small burns, and 7/12 thought it might also work for large surface burns: all the others answered that they did not know.
Discussion
This study attempted to examine the importance and impact of the use of ‘Secret’ in the Lausanne Burn Centre. Although limited to qualitative questionnaires and to a voluntary participation, we have shown that the phenomenon is well known and tolerated in the medical setting by most healthcare professionals, patients and their families. It is not considered dangerous; most of the healthcare professionals even consider it useful. Some believe in these practices, whereas others consider it to merely have a sort of placebo effect.
Concerning the practice at hand, its clinical benefit might be linked to the mystery in which it is shrouded. The issue of efficacy remains uncertain among the healthcare professionals. On one hand, the opinions of professionals and patients were in agreement, but on the other hand, contradictory answers were collected regarding efficacy of the practice on different sizes of burn wounds (Fig. 3). The most notable divergence in opinion was observed when dealing with professionals from the Plastic Surgery and the Intensive Care Services. Addressing the benefits of this practice, in the eyes of most HPs these consist of pain relief (Fig. 5), renewed hope for the patient, and a greater involvement of the patient’s family.
On the healthcare side, caregivers do not think that ‘Secret’ might be dangerous (Fig. 6) or that it should remainoutside hospitals, rather half of them think it should be used more often (Fig. 7). It is notable that the caregiver profession (nurse, MD, auxiliary nurse, physiotherapist) has an influence on their opinion regarding efficacy and utility.
On the patient side, the survey shows that they welcome this kind of intervention, mainly in the hope it will reduce overall pain and aid a more rapid recovery. Most feel that they benefit from it. However, it is clear that for most interviewed patients the practice of ‘Secret’ is merely a complementary step towards their well-being, which cannot replace conventional medical care. The practice can be qualified, as one healthcare professional said, as: “an option to be offered once the patient is already being taken care of. It is free, and if it can help without harming, it improves the patient mood.” Furthermore, it has been discovered that patients seek advice from members of the medical staff. Given the limited number of patients interviewed, it was not possible to determine if age or origin plays a significant role in the noted differences of opinion. Nevertheless, the fact that 11 out of 12 patients called for ‘Secret’ portrays that the practice is well established in popular tradition, and it is important to have general courses in Medical studies to raise awareness of Alternative Medicine Practices.
The search for a scientific and/or rational explanation for the assumed benefits of ‘Secret’ leads directly to the notion of stress. Burn patients and their families experience a severe state of mental distress, considering issues like death, mutilation or permanent handicap. The healer appears in this context as an alternative source of hope, whose positive effect also works on the patient’s loved ones. By attenuating the family’s stress, the healer reduces the family’s anguish, which largely impacts the patient himself.6 Analysis of the effects of stress must be conducted on two essential levels: dealing with pain and wound healing. Regarding pain, it has been proven that treatment with a sedative anxiolytic potentiates the pharmacological effects of opiates.7 Therefore, it would be possible to associate the healer’s role in perceived pain reduction in the context of anxiety and stress for the patient and Healthcare Professional. Moreover, some observed reductions in pain intensity remain unexplained and need research.
Regarding wound healing, evidence shows a strong link between stress and tissue repair, particularly for ulcers and chronic wounds.8 Circulating cortisol and epinephrine levels have a direct incidence, via vasomotor effects, tissue biology and infectious agents.9 The patient’s belief in ‘Secret’s’ beneficial effects and the fact that the patient or family reaches out to Folk Medicine increases confidence, which might drastically reduce the stress level.10,11 This reduction in the patient’s stress could help to achieve optimal and more rapid wound healing. It has been shown that adequate pain treatment after hernia repair leads to increased production of metalloproteinase in the wound, with reduction of inflammation and a more rapid closure.8 Similar observations have been made for hypnosis, which is used in the Centre.12
Help is expected from the healers, not in a strictly medical area, but without transferring all hope in this option. In his M.D. Thesis conducted in High Savoy,13 Dr. Nicolas Perret showed that in a population believing in ‘Secret’ and accepting the healer’s intervention, pain reduction could be observed for 87% of patients (reduction of 45 ± 15% for 30% of the group and >60% for 57% of the group). Focusing the patient’s attention on something other than their pain, by means of alternative reality for example, has also shown a significant reduction in their pain and stress levels,14 speeding up their recovery and shortening their stay in the hospital. These elements all show that trust and confidence reduce stress and pain. “The placebo effect encourages us not to use a placebo, but to work with non-specific factors that can modulate any therapeutic process. All practitioners must know how to potentiate specific factors of a therapeutic action by a quality patient-doctor relationship, which can induce complementary non-specific factors” as stated in French by Guy-Coichard and Boureau.15
‘Secret’ is fairly well accepted among the general population and, as shown by this survey, also by professionals: this is not necessarily the case among doctors, as shown by the necessity of the centre’s leading team to justify the practice in the local medical journal in 2005.16
Our study has important limitations. Firstly, the questionnaire is not validated but developed within the service, based on recurrent questions that were asked within the HPS group. Secondly, the population sample is small, but cannot be extended due to the service side: answers were based on a voluntary population. Finally, the study did not aim to address the efficacy of ‘Secret’, which may be addressed with a prospective study.
Conclusion
The Burn Centre admits patients that have suffered a traumatic event and who are in a deep state of stress, anguish and pain. In these extreme conditions, it is not uncommon for patients and their family to seek assistance outside the boundaries of Western medical care. Compared to the stressful and highly technical ICU context, a form of care given over the phone to a population who has lived immersed in these beliefs is not an obstacle, but contributes to stress reduction. This preliminary observation opens the door to future anthropologic and medical investigations regarding the potential and overall use of similar phenomena and experience worldwide. We would like to end this work by quoting two major statisticians. Altman and Bland stated that: “While it is usually reasonable not to accept a new treatment unless there is positive evidences in its favor, when issues of public health are concerned we must question whether the absence of evidence is a valid enough justification for inaction”.17
Acknowledgments
Conflict of interest.No financial support or other conflict of interest relevant to this article is reported by the authors.
Acknowledgements.The Authors would like to acknowledge the support of the burn patients interviewed and the entire team of the Lausanne Burn Centre.
References
- 1.Jenny M. Favre. Lausanne: 2009. Le nouveau guide des guérisseurs de suisse romande. [Google Scholar]
- 2.Federal Office of Culture. [Last modification: 04.06.2018]; [accessed 05.09.2019];The secret. Available at: http://www.lebendigetraditionen.ch/traditionen/00154/index.html?lang=en . [Google Scholar]
- 3.SA AlpSoft. Faiseurs de secret. Available from: http://alpmobi.ch/app/17 . [Google Scholar]
- 4.Julio A. Prières Merveilleuses - Pour la guérison de toutes les maladies physiques et morales. Bussière. 1995 [Google Scholar]
- 5.Derivaz F, Clerc F. Favre. Lausanne, Switzerland: 2014. Faiseurs de secrets et dons de guérisoncomment ça marche? [Google Scholar]
- 6.Wiesendanger H, Werthmuller L, Reuter K, Walach H. Chronically ill patients treated by spiritual healing improve in quality of life: results of a randomized waiting-list controlled study. J Altern Complement Med. 2001;7:45–51. doi: 10.1089/107555301300004529. [DOI] [PubMed] [Google Scholar]
- 7.Clerc F, Derivaz F. Favre SA. Lausanne: 2015. Faiseurs de sercrets et dons de guérison, comment ça marche? [Google Scholar]
- 8.Broadbent E, Petrie KJ, Alley PG, Booth RJ. Psychological stress impairs early wound repair following surgery. Psychosom Med. 2003;65:865–869. doi: 10.1097/01.psy.0000088589.92699.30. [DOI] [PubMed] [Google Scholar]
- 9.Galinski M, Dolveck F, Combes X, Limoges V. Management of severe acute pain in emergency settings: ketamine reduces morphine consumption. Am J Emerg Med. 2007;25:385–390. doi: 10.1016/j.ajem.2006.11.016. [DOI] [PubMed] [Google Scholar]
- 10.Moffatt CF, Franks PJ, Doherty DC, Smithdale R, Steptoe A. Psychological factors in leg ulceration: a case-control study. Br J Dermatol. 2009;161:750–756. doi: 10.1111/j.1365-2133.2009.09211.x. [DOI] [PubMed] [Google Scholar]
- 11.Mohammadi AA, Bakhshaeekia A, Alibeigi P. Hasheminasab MJ et al.: Efficacy of propranolol in wound healing for hospitalized burn patients. J Burn Care Res. 2009;30:1013–1017. doi: 10.1097/BCR.0b013e3181b48600. [DOI] [PubMed] [Google Scholar]
- 12.Berger MM, Davadant M, Marin C, Pinget C. Impact of a pain protocol including standardized opioid prescription, opioid rotation and hypnosis on pain levels and clinical evolution after major burns. Intensive Care Med. 2008;34 (suppl 1) [Google Scholar]
- 13.Perret N. Faculty of Medicine. Vol. 192. Grenoble: 2009. [Place of the fire cutters in the ambulant and hospital treatment of burns in High Savoy in 2007]. Place des coupeurs de feu dans la prise en charge ambulatoire et hospitalière des brûlures en Haute-Savoie en 2007. Available at: https://dumas.ccsd.cnrs.fr/dumas-00630683/document . [Google Scholar]
- 14.Morris LD, Louw QA, Grimmer-Somers K. The effectiveness of virtual reality on reducing pain and anxiety in burn injury patients: a systematic review. Clin J Pain. 2009;25:815–826. doi: 10.1097/AJP.0b013e3181aaa909. [DOI] [PubMed] [Google Scholar]
- 15.Guy-Coichard C, Boureau F. Understand placebo effect to better treat pain. Rev Med Interne. 2005;26:226–232. doi: 10.1016/j.revmed.2004.11.002. [DOI] [PubMed] [Google Scholar]
- 16.Chioléro R, Maravic P, Berger MM, Raffoul W. De l’usage du «secret» au Centre des brûlés du CHUV. Courrier du Médecin Vaudois. 2005 [Google Scholar]
- 17.Altman DG, Bland JM. Absence of evidence is not evidence of absence. BMJ. 1995;311X:485. doi: 10.1136/bmj.311.7003.485. [DOI] [PMC free article] [PubMed] [Google Scholar]