
Figure 1.
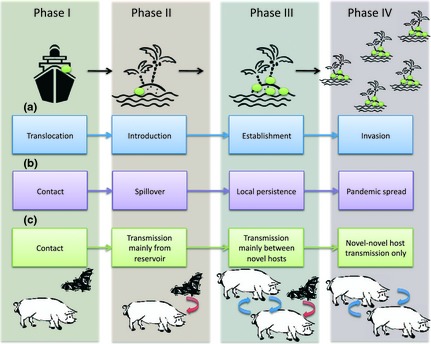
Phases of invasion and emergence. Arrow‐linked boxes show the sequence of processes involved in (a) biological invasion (e.g. Kolar & Lodge 2001); (b,c) emerging infectious diseases (EID): (b) the demographic perspective (e.g. Childs, Richt & Mackenzie 2007; Hatcher & Dunn 2011), (c) the evolutionary perspective (e.g. Wolfe, Dunavan & Diamond 2007). Vertically, the aligned phases (as shaded) correspond; we will refer to these as Phases I to IV. Transition from one phase to the next is influenced by different factors; these factors are to some extent common to both invasions and EIDs, and an examination of parallels may shed light on potential control opportunities. Phase 1: contact between reservoir and novel hosts may be frequent; it may arise or be increased as a result of introduction of a new reservoir host; contact rate may increase as a result of environmental change; contact rate may be enhanced through parasite manipulation of host behaviour. Phase 2: spillover/introduction is affected by rate of bombardment with the novel parasite (propagule pressure), the suitability of the novel host or habitat (i.e. evolutionary considerations, such as local adaptation, and environmental characteristics, such as climate suitability). Phase 3: establishment/local persistence/novel intraspecific transmission; for EIDs, this requires that each infected host of the novel species generates more than one secondary case of infection (i.e. R 0 for the parasite >1). This will be affected by evolutionary factors (local adaptation; host or habitat competency) and also depends on (host) population or habitat structure. Phase 4: pandemic spread/invasion/novel intraspecific‐only transmission. For EIDs, this also requires R 0 > 1, but the distribution of R 0 also matters (skewed distributions with superspreaders can lead to more rapid spread); successful transition also depends on parasite (or host) evolution; for instance adaptation to the novel host/environment. Pandemic emergence is strongly linked to global transport and travel.