
Fig. 2.
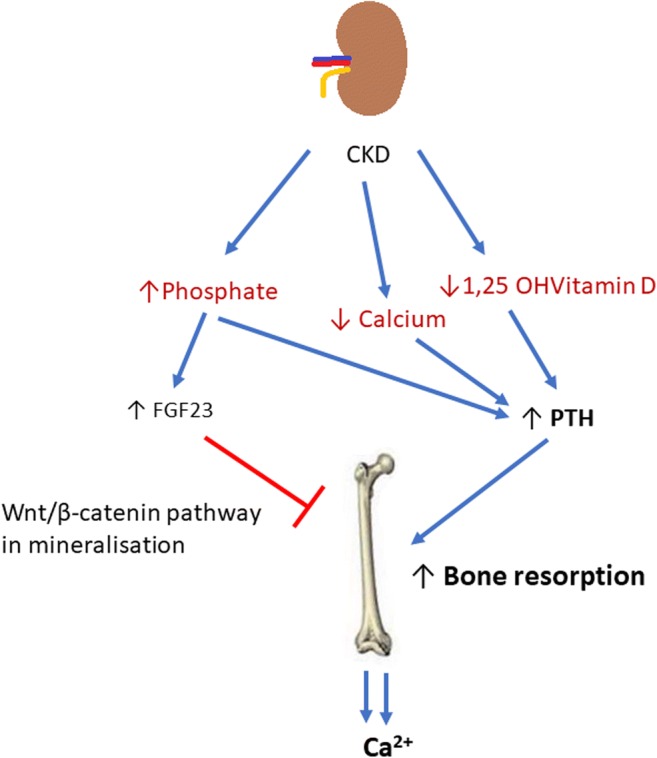
In chronic kidney disease (CKD), hypocalcaemia, low 1,25 OH vitamin D levels and hyperphosphataemia develop. In an attempt to increase phosphaturia, and thus decrease serum phosphate levels, FGF23 production increases. Raised FGF23 may directly inhibit Wnt signalling pathways which are needed in bone mineralisation. Low 1,25OHVitD and low serum calcium lead to increased PTH production. This in turn causes increased bone turnover with the aim of restoring normocalcaemia, by mobilising calcium out of bone. The reduced production of active vitamin D from the kidneys perpetuates hypocalcaemia further fuelling this cycle. This demineralisation affects bone quality as a whole leading to an increased risk of fractures and decreased bone strength