

Abstract
Multidimensional Inventory Check List of Symptoms (SCL-90-r) is based on self-evaluation and it has been used for determination of level of: somatisation, obsessive-compulsive symptoms, interpersonal sensitivity, depression, anxiety, hostility, phobias, paranoia and psychosis at persons which are exposed to long term emotional and physical stress. Our goal was to determine relations of physical trauma and psychological changes at persons with lower extremities amputations and to determine factors which influence those changes. Thirty seven persons with lower extremities amputations were examined. The sample included 26 (70,2 %) veterans and 11 (29,7 %) civilians with diseases related amputations. They voluntarily filled Check List of Symptoms SCL-90-r. Symptoms Inventory includes 9 dimensions of primary symptoms: SCL1-somatisation, SCL2-obsessive-compulsive symptoms, SCL3-interpersonal sensitivity, SCL4-depression, SCL5-anxiety, SCL6-hostility, SCL7-phobias, SCL8-paranoia, SCL9-psychosis and SCL10-extra scale. Inventory includes 90 statements, each evaluated with five-level scale of disorder. Every answer is graded with 04-points. Thirty seven persons with lower extremities amputations and average chronological age 46,2 ± 10,92 years were analyzed. Considering marital status 30 (81,1 %) of them were married, 4 (10,8 %) were not married and 3 (8,1 %) were widowers. Considering level of amputation 27 of them (73,0 %) had amputation below knee, 5 (13,5 %) of them amputation above knee and 5 of them (13,5 %) foot amputation. SCL-90-r in both groups determined high level of sensitivity, anxiety, hostility and paranoia. Veterans showed higher level of paranoia comparing to civilians (p<0,002), and younger veterans and married ones had higher level of paranoia comparing to other veterans (p<0,01). Persons with amputations below and above knee showed higher level of paranoia comparing those with foot amputation (p<0,001). Persons with lower extremities amputations have considerably more expressed sensitivity, anxiety, hostility and paranoia. These dimensions are related to age, marital status and level of amputation. These determinants are very helpful for planning and creation of psychological support and rehabilitation of persons with lower extremities amputations.
Keywords: amputation, SCL-90-r, physical trauma
INTRODUCTION
Multidimensional Inventory Check List of Symptoms (SCL-90-r) is based on self-evaluation and it has been used for determination of level of: somatisation, obsessive-compulsive symptoms, interpersonal sensitivity, depression, anxiety, hostility, phobias, paranoia and psychosis with persons who are exposed to long term emotional and physical stress. Individuals who experience mutilation without previously being ill or exposed to stress go through psychological crisis mutilation as a result of illness or trauma represents strong psychological trauma that can cause a spectrum of different psychological reactions (1). According to the same author, psychological reactions of mutilated patients are divided in four phases of grievance:
Phase of acute psychological reactions (or phase of acute crisis) that occurs immediately after the trauma and is expressed as nihilism, depressive impressions, suicidal thoughts and actions, hysterical reaction, etc.
Phase of creation of emotional balance.
Late phase of psychological reactions.
Phase of adaptation which occurs after psychological reactions discontinue, and in which phase the patient is adapting to new reality.
Amputation is not only a loss of a part of the body, it also results in the loss of body integrity and it has a profound impact on patient’s mental status (2). Problems en-countered in this regard depend more on attributes and personality of a specific patient that the level of amputation (3). The goal of this work is to determine relation between physical trauma and psychological changes with persons with lower extremities amputations and to determine factors which influence those changes.
SUBJECTS AND METHODS
Thirty seven persons with lower extremities amputations were examined. The sample included 26 (70,2%) veterans and 11 (29,7 %) civilians with disease related amputations. They voluntarily filled Check List of Symptoms SCL-90-r (4). Symptoms Inventory includes 9 dimensions of primary symptoms: SCL1-somatisation, SCL2-obsessive-compulsive symptoms, SCL3-in-terpersonal sensitivity, SCL4-depression, SCL5-anxiety, SCL6-hostility, SCL7-phobias, SCL8-paranoia, SCL9-psychosis and SCL10-extra scale. The inventory includes 90 statements, each evaluated with five-level scale of disorder. Every answer is graded with 04-points. Beside SCL-90-r subjects have filed personal questionnaires. Statistics made in SPSS 10.0 for Windows.
RESULTS AND DISCUSSION
Thirty seven persons with lower extremities amputations and average age of 46,2 ± 10,92 were analyzed, which includes 11 civilians (average age 52,7 ± 4,2) and 26 individuals with war-related amputation (average age 43,5 ± 1,6) (Figure 1). In accordance with marital status, there were 30 (81,1 %) married examinees, 4(10,8 %) single and 3 widower (8,1 %) (Table 1). In accordance with amputation level, 27 (73,0 %) examinees have had below-knee amputation, 5 (13,5 %) have had aboveknee amputation and 5 (13,5 %) have had foot amputation (Table 2). In many studies in the world, authors followed psychological reaction persons with amputation, and conclusion is that they have normal life after long time in spite lot of physical limitations (5). For all samples average time is 10,8 years after amputation. In accordance with SCL-90-r, both groups had high level of sensitivity, anxiety, hostility and paranoia (Figure 2, 3, 4, 5). Paranoia is more visible with veterans than civilians (p<0,002); younger veterans and those married expressed higher level of paranoia (p<0,01) (Figure 6 and 7). Paranoia is more expressed by examinees with below-knee and above-knee amputation than by examinees with foot amputation (p< 0,001) (Figure 8).
FIGURE 1.

Distribution of examinees by the age groups
TABLE 1.
Distribution of examinees as per marital status
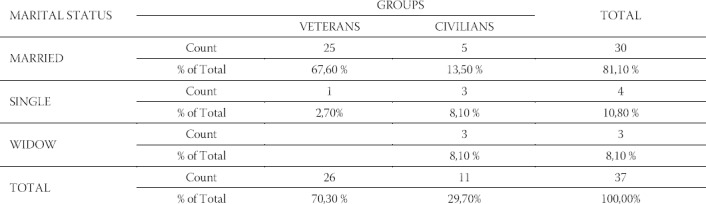
TABLE 2.
Distribution of examinees by amputation level
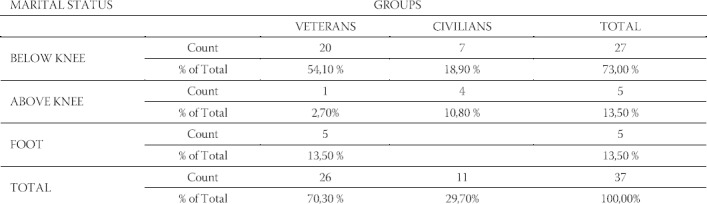
FIGURE 2.
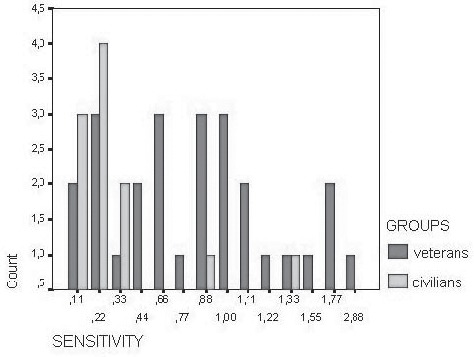
Distribution of examinees as per level of sensitivity
FIGURE 3.
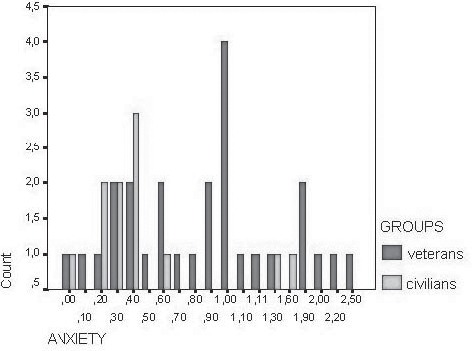
Distribution of examinees as per level of anxiety
FIGURE 4.
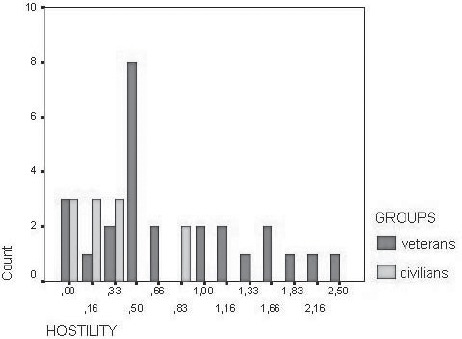
Distribution of examinees as per level of hostility
FIGURE 5.
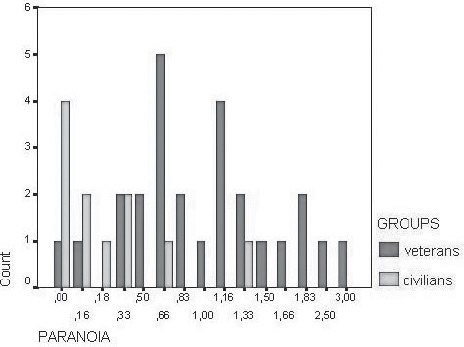
Distribution of examinees as per level of paranoia
FIGURE 6.
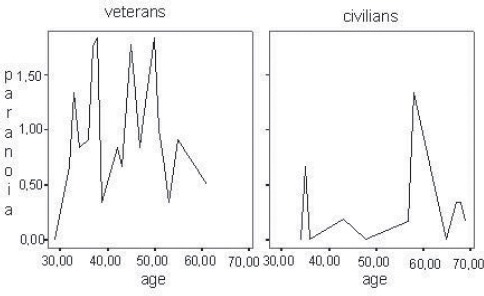
Correlation between level of paranoia and examinees age group
FIGURE 7.
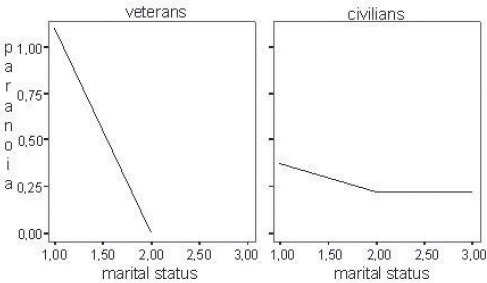
Correlation between marital status and examinees paranoia
FIGURE 8.
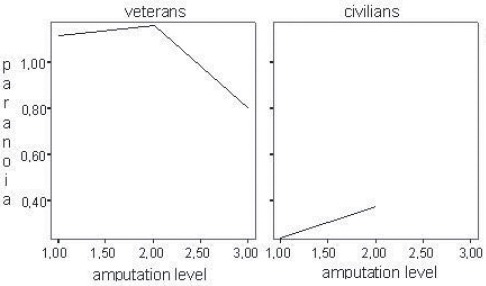
Correlation between amputation level and examinees level of paranoia
CONCLUSION
Persons with lower extremities amputations express significant levels of sensitivity, anxiety, hostility and paranoia. These dimensions are related to age, marital status and level of amputation. These determinants are very helpful for planning and creation of psychological support and rehabilitation of persons with lower extremities amputations.
REFERENCES
- 1.Peršić-Brida M. Kriza suočavanja sa invaliditetom. In: urednici Jakovljević M, Kulenović M, Jakupčić M., editors. Krizna stanja: Klinika – Konzultacija – Intervencija. Zagreb: Medicinski fakultet; l986. pp. 83–86. [Google Scholar]
- 2.Moro LJ, Frančišković T. Organizacija skrbi za bolesnike oboljele od posttraumatskog stresnog poremećaja. Tuzla: Zbornik radova sedmih (prvih poslijeratnih) psihijatrijskih dana Bosne i Hercegovine; 1999. pp. 165–174. [Google Scholar]
- 3.Muminagić S. Ratna amputacija, Tiskarna Jože Moškrić. Ljubljana. 1996:1517. [Google Scholar]
- 4.Derogatis LR. SCL-90-r administration, scoring and procedures manual – for the r (revised) version. Eigendruc: Johns Hopkins University School of Medicine; l977. [Google Scholar]
- 5.Dougherty PJ. Long – Term folow -up study of bilateral above the knee amputees from the Vietnam War. J. Bone. Joint. Surg. Am. 1999;81(10):1384–1390. doi: 10.2106/00004623-199910000-00003. [DOI] [PubMed] [Google Scholar]