

Abstract
Background
Nausea, retching and vomiting are very commonly experienced by women in early pregnancy. There are considerable physical, social and psychological effects on women who experience these symptoms. This is an update of a review of interventions for nausea and vomiting in early pregnancy last published in 2014.
Objectives
To assess the effectiveness and safety of all interventions for nausea, vomiting and retching in early pregnancy, up to 20 weeks’ gestation.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group’s Trials Register, the Cochrane Complementary Medicine Field's Trials Register (19 January 2015) and reference lists of retrieved studies.
Selection criteria
All randomised controlled trials of any intervention for nausea, vomiting and retching in early pregnancy. We excluded trials of interventions for hyperemesis gravidarum, which are covered by another Cochrane review. We also excluded quasi‐randomised trials and trials using a cross‐over design.
Data collection and analysis
Four review authors, in pairs, reviewed the eligibility of trials and independently evaluated the risk of bias and extracted the data for included trials.
Main results
Forty‐one trials involving 5449 women, met the inclusion criteria. These trials covered many interventions, including acupressure, acustimulation, acupuncture, ginger, chamomile, lemon oil, mint oil, vitamin B6 and several antiemetic drugs. There were no included studies of dietary and other lifestyle interventions. Evidence regarding the effectiveness of P6 acupressure, auricular (ear) acupressure and acustimulation of the P6 point was limited. Acupuncture (P6 or traditional) showed no significant benefit to women in pregnancy. The use of ginger products may be helpful to women, but the evidence of effectiveness was limited and not consistent, though three recent studies support ginger over placebo. There was only limited evidence from trials to support the use of pharmacological agents including vitamin B6, Doxylamine‐pyridoxoine and other anti‐emetic drugs to relieve mild or moderate nausea and vomiting. There was little information on maternal and fetal adverse outcomes and on psychological, social or economic outcomes.
We were unable to pool findings from studies for most outcomes due to heterogeneity in study participants, interventions, comparison groups, and outcomes measured or reported. The methodological quality of the included studies was mixed. Risk of bias was low related to performance bias, detection bias and attrition bias for most studies. Selection bias risk was unclear for many studies and almost half of the studies did not fully or clearly report all pre‐specified outcomes.
Authors' conclusions
Given the high prevalence of nausea and vomiting in early pregnancy, women and health professionals need clear guidance about effective and safe interventions, based on systematically reviewed evidence. There is a lack of high‐quality evidence to support any particular intervention. This is not the same as saying that the interventions studied are ineffective, but that there is insufficient strong evidence for any one intervention. The difficulties in interpreting and pooling the results of the studies included in this review highlight the need for specific, consistent and clearly justified outcomes and approaches to measurement in research studies.
Keywords: Female, Humans, Pregnancy, Acupuncture Therapy, Acupuncture Therapy/methods, Antiemetics, Antiemetics/therapeutic use, Morning Sickness, Morning Sickness/etiology, Morning Sickness/therapy, Nausea, Nausea/etiology, Nausea/therapy, Phytotherapy, Phytotherapy/methods, Pregnancy Complications, Pregnancy Complications/therapy, Randomized Controlled Trials as Topic, Treatment Outcome, Vitamin B 6, Vitamin B 6/therapeutic use, Vitamin B Complex, Vitamin B Complex/therapeutic use, Vomiting, Vomiting/etiology, Vomiting/therapy
Plain language summary
Interventions for nausea and vomiting in early pregnancy
Nausea, retching or dry heaving, and vomiting in early pregnancy are very common and can be very distressing for women. Many treatments are available to women with 'morning sickness', including drugs and complementary and alternative therapies. Because of concerns that taking medications may adversely affect the development of the fetus, this review aimed to examine if these treatments have been found to be effective and safe.
This review found a lack of high‐quality evidence to back up any advice on which interventions to use. We examined 41 randomised controlled trials that included 5449 women in early pregnancy. These studies examined the effectiveness of many treatments including acupressure to the P6 point on the wrist, acustimulation, acupuncture, ginger, chamomile, vitamin B6, lemon oil, mint oil, and several drugs that are used to reduce nausea or vomiting. Some studies showed a benefit in improving nausea and vomiting symptoms for women, but generally effects were inconsistent and limited. Overall, studies had low risk of bias related to blinding and reporting on all participants in the studies. However some aspects of the studies were reported incompletely in a way that meant how participants were allocated to groups was unclear and not all results were fully and clearly reported. Most studies had different ways of measuring the symptoms of nausea and vomiting and therefore, we could not look at these findings together. Few studies reported maternal and fetal adverse outcomes and there was very little information on the effectiveness of treatments for improving women's quality of life.
Background
Description of the condition
Nausea and vomiting are commonly experienced by women in early pregnancy. Prevalence rates of between 50% and 80% are reported for nausea, and rates of 50% for vomiting and retching (Miller 2002; Woolhouse 2006). A recent meta‐analysis of reported rates of these symptoms confirms a mean rate of 70%, with widely varying rates (between 35% and 91%) across reports (Einarson 2013). Retching (or dry heaving, without expulsion of the stomach's contents) has been described as a distinct symptom that is increasingly measured separately to vomiting and nausea (Lacasse 2008; O'Brien 1996; Zhou 2001).
The misnomer 'morning sickness', which is colloquially used to describe nausea, vomiting and retching of pregnancy, belies the fact that symptoms can occur at any time of the day. Pregnant women experience nausea, vomiting and retching mostly in the first trimester, between six and 12 weeks, but this can continue to 20 weeks and persists after this time for up to 20% of women (Jewell 2003b; Miller 2002).
Hyperemesis gravidarum, which is characterised by severe and persistent vomiting, is less common, affecting between 0.3% and 3% of pregnant women (Eliakim 2000; Jewell 2003b; Miller 2002). Within their meta‐analysis of prevalence reports, a mean rate of 1.1% is identified by Einarson 2013, with a range of 0.3% to 3.6% across the included studies. Hyperemesis gravidarum is defined in different ways, though a widely used definition describes it as “intractable vomiting associated with weight loss of more than 5% of prepregnancy weight, dehydration and electrolyte imbalances which may lead to hospitalisation” (Miller 2002). Ketosis is also commonly included as a consequence of hyperemesis gravidarum (Kousen 1993; Quinlan 2003). Including inpatient hospitalisation in the definition of hyperemesis gravidarum is problematic (Swallow 2002), as some instances may be alleviated or controlled by outpatient interventions (Bsat 2003b). Within the operational definitions of hyperemesis gravidarum, there is generally a focus on the effects of the vomiting (dehydration, ketosis, weight loss). The lack of a standard definition has implications for the measurement of outcomes in controlled studies.
It is important to exclude pathological causes of nausea and vomiting before concluding that this is specific to pregnancy. Pregnant women being treated for nausea, vomiting and retching of pregnancy should have other pathological causes of nausea and vomiting (such as peptic ulcers, cholecystitis, gastroenteritis, appendicitis, hepatitis, genito‐urinary (e.g. pyelonephritis), or metabolic and neurological disorders) considered and excluded before a diagnosis of nausea, vomiting and retching of pregnancy is given (Davis 2004; Koch 2002; Quinlan 2003).
Thought to be associated with rising levels of human chorionic gonadotropin (hCG) or oestrogens, the causes of nausea, vomiting and retching of pregnancy remain unknown (Goodwin 2002). Vestibular, gastrointestinal, olfactory and behavioural factors may influence the woman’s response to the hormonal changes (Goodwin 2002). Social, psychological and cultural influencing factors have also been studied (Buckwalter 2002; Chan 2011; O'Brien 1999). The number of previous pregnancies and the number of fetuses both seem to affect the risk of nausea and vomiting of pregnancy (Einarson 2007; Louik 2006). Conditions with higher levels of hCG (multiple pregnancies and molar pregnancies (hydatidiform mole)) have been associated with more prevalent and more severe nausea and vomiting of pregnancy. Based on observational studies, nausea, vomiting and retching in the first trimester were thought to be associated with a decreased risk of miscarriage, preterm delivery, low birthweight, stillbirth, and fetal and perinatal mortality (Czeizel 2004; Weigel 1989), although a later study challenged these claims (Louik 2006).
There are several scales used to measure the symptoms of nausea, vomiting and retching in pregnancy. The Rhodes Index of Nausea, Vomiting and Retching (three subscales: nausea, vomiting and retching), comprising eight items, measures levels and distress caused by these symptoms. A possible score range is eight to 40 representing no symptoms to maximal symptoms; the cut‐off point for severe symptoms is 33. Originally created by Rhodes (Rhodes 1984) to measure the nausea and vomiting symptoms associated with chemotherapy, this index has been validated in studies of nausea and vomiting of pregnancy (O'Brien 1996; Zhou 2001). The Pregnancy‐Unique Quantification of Emesis and Nausea (PUQE), comprises three subscales covering nausea, vomiting and retching during the past 12 hours. Symptoms are measured using a five‐point Likert scale; possible range three to 15, representing no symptoms to maximal symptoms; the cut‐off point for severe symptoms is 13. This scale was developed by clinician‐researchers at the Canadian Motherisk Program (Koren 2002a) studying nausea and vomiting in pregnancy and validated using the Rhodes Index (see next paragraph) and independent variables (Koren 2002b; Koren 2005; Lacasse 2008). The McGill Nausea Questionnaire measures nausea only. This questionnaire includes a qualitative measure (sets of verbal, affective and other descriptors of nausea); a nausea rating index (nine sets of words ranked in order of increasing severity); an overall nausea index; and a visual analogue scale (VAS) (no nausea to extreme nausea, 10 cm scale). It was developed by Melzack for cancer chemotherapy and validated for use in studies of nausea and vomiting in pregnancy (Lacroix 2000; Melzack 1985). The Nausea and Vomiting of Pregnancy Instrument includes three questions, one each about nausea, vomiting and retching in the past week; possible range is zero to 15; the cut‐off point for severe symptoms is eight. Reliability and validity have been adequately described (Swallow 2002; Swallow 2005). Finally, a VAS (graded zero to 10, or zero to 100) can be used to record severity of nausea (Can Gurkan 2008; Pongrojpaw 2007b; Vutyavanich 1995).
Description of the intervention
Women are commonly offered advice about the (usually) self‐limiting nature of the condition and advised to avoid foods, smells, activities or situations that they find nauseating and to eat small frequent meals of dry, bland foodstuffs (Davis 2004; Ornstein 1995). Many remedies are suggested for nausea and vomiting in early pregnancy, including pharmaceutical and non‐pharmaceutical interventions.
Pharmaceutical treatments include anticholinergics, antihistamines, dopamine antagonists, vitamins (B6 and B12), H3 antagonists or combinations of these substances (Koren 2002a; Kousen 1993; Magee 2002a; Quinlan 2003). The teratogenic effects (ability to disturb the growth or development of the embryo or fetus) of pharmaceutical medications used in the past to control these symptoms (such as thalidomide) have led to caution about prescribing and taking medications in the first trimester. Doxylamine has been used in various formulations: as dicyclomine, doxylamine and pyridoxine (US trade name, Bendectin); as dicyclomine, doxylamine and pyridoxine (UK trade name, Debendox); and as doxylamine and pyridoxine (Canadian trade name, Diclectin). This drug was withdrawn from the US market because of the legal costs incurred by its manufacturers, despite a lack of legal rulings against it (Brent 2002; Koren 2002a; Ornstein 1995). It is approved by Health Canada for use in Canada and received FDA approval for use in pregnancy in April 2013, under the trade name of Diclegis (Slaughter 2014).
Because of historical concerns about pharmaceuticals in early pregnancy and the general rise in the use of complementary and alternative therapies, non‐pharmaceutical treatments are increasingly used to treat nausea and vomiting in pregnancy. They may be perceived as 'natural' and therefore safe or having lower risk than medications. These include herbal remedies (ginger, chamomile, peppermint, raspberry leaf), acupressure, acustimulation bands and acupuncture, relaxation, autogenic feedback training, homeopathic remedies (Nux vomica, Pulsatilla), massage, hypnotherapy, dietary interventions, activity interventions, emotional support, psychological interventions and behavioural interventions/modifications (Aikins Murphy 1998; Davis 2004; Jewell 2003b; Niebyl 2002; Wilkinson 2000). Acupressure is a noninvasive variation of acupuncture that involves the application of constant pressure to specific points or areas. P6 (or Neiguan point) acupressure is proposed to treat symptoms of nausea and vomiting (O'Brien 1996). The P6 point is located on the medial aspect of the forearm, at a specific point near the wrist.
How the intervention might work
Each pharmaceutical and non‐pharmaceutical intervention described above is proposed to treat nausea and vomiting in pregnancy according to its specific mode of action. However, the exact mechanism of action for many of these interventions is poorly understood. Pharmceutical interventions act by targeting specific receptors in the body that are involved in nausea and vomiting. These include anticholinergics, antihistamines, dopamine antagonists, H3 antagonists, combinations of these substances, and vitamins (B6 and B12). Their use in treating nausea and vomiting in other populations or conditions has led to their use in early pregnancy. Thus, successful symptomatic relief in other populations (e.g. patients undergoing chemotherapeutic interventions for cancer), has led to their use in pregnancy. Similarly, the non‐pharmaceutical interventions proposed to treat nausea and vomiting in early pregnancy are used to treat those symptoms in other populations or have a history of being used traditionally in pregnancy.
Why it is important to do this review
There are considerable physical and psychological effects on women who experience nausea and vomiting in pregnancy, with altered family, social or occupational functioning (Attard 2002; Chou 2003; Chou 2008; O'Brien 1992; O'Brien 1997; Swallow 2004). Nausea and vomiting affect women’s daily activities and their relationships (Atanackovic 2001; Attard 2002; Magee 2002b). The distress and functional limitations caused by nausea without vomiting are increasingly acknowledged (Davis 2004; Wood 2013). Women have reported that they would like their symptoms and ensuing distress acknowledged to a greater degree by health professionals (Locock 2008). Quality of life effects are becoming more of a focus in research (Munch 2011) and reviews (Wood 2013). Studies have also highlighted the economic burden on women and society from these symptoms, mainly due to lost productivity and healthcare costs (Attard 2002; Piwko 2007; Piwko 2013).
Studies report that healthcare professionals frequently recommend non‐pharmaceutical treatments (Bayles 2007; Westfall 2004), and women frequently use them (Ernst 2002b; Hall 2011; Tiran 2002). Alongside this growth in their use, there are concerns about the efficacy and safety of non‐pharmaceutical treatments (Ernst 2002a; Ernst 2002b; Tiran 2002; Tiran 2003), as they are less rigorously tested and regulated than pharmaceutical remedies. In addition, women and professionals are more likely to underestimate their possible risks (Tiran 2002; Tiran 2003; Tiran 2012).
Objectives
To assess the effectiveness and safety of all interventions used for nausea, vomiting and retching in early pregnancy, up to 20 weeks’ gestation.
Methods
Criteria for considering studies for this review
Types of studies
We included all randomised controlled trials of any intervention for nausea, vomiting and retching in early pregnancy. We excluded trials of interventions for hyperemesis gravidarum, which is being covered by another Cochrane review (Boelig 2013). We have not included quasi‐randomised trials and trials using a cross‐over design. We have included studies reported in abstracts only, provided that there was sufficient information in the abstract, or available from the author, to allow us to assess eligibility and risk of bias.
Types of participants
Women experiencing nausea, vomiting and/or retching in pregnancy (but not hyperemesis gravidarum), where recruitment to a trial took place up to 20 weeks' gestation.
Types of interventions
We included all interventions for nausea, vomiting and/or retching. Comparisons included:
intervention versus placebo;
one intervention versus a different type of intervention.
Types of outcome measures
Primary outcomes
Symptomatic relief
Reduction or cessation in nausea, vomiting and/or retching. We examined outcomes measured by all commonly used, validated instruments.
The primary outcome of reduction in symptoms, encompasses non‐worsening of symptoms (including up to those of hyperemesis gravidarum).
Adverse maternal and fetal/neonatal outcomes
Adverse fetal/neonatal outcomes
Fetal or neonatal death. This includes spontaneous abortion, stillbirth (death of a fetus of at least 500 g weight or after 20 weeks' gestation); neonatal death (death of a baby born alive, within 28 days of birth).
Congenital abnormalities (an abnormality of prenatal origin, including structural, genetic and/or chromosomal abnormalities and biochemical defects, but not including minor malformations that do not require medical treatment) (South Australian Health Commission 1999; Zhou 1999).
Low birthweight (less than 2.5 kg).
Early preterm birth (before 34 weeks' gestation).
Adverse maternal outcomes
Pregnancy complications (antepartum haemorrhage, hypertension, pre‐eclampsia (hypertension ≥ 140/90 mm Hg (millimetres of mercury), proteinuria ≥ 0.3 g/L from the 20th week of pregnancy).
Secondary outcomes
Quality of life
Quality of life outcomes encompass emotional, psychological, and physical well‐being; women's assessment of the pregnancy experience; or women's ability to cope with the pregnancy. They can be measured using the General Health Questionnaire (GHQ), other generic Quality of Life (QoL), well‐being (mental health), and coping tools (Attard 2002; Chou 2003; Lacasse 2008; Swallow 2004; Swallow 2005), or a validated pregnancy‐specific Quality of Life instrument (Magee 2002b).
Economic costs
Direct financial costs to women (purchase of treatments).
Productivity costs (time off work).
Healthcare system costs (provision of services, consultation time, staff time) (Attard 2002; Koren 2005; Piwko 2007).
Search methods for identification of studies
The following methods section of this review is based on a standard template used by the Cochrane Pregnancy and Childbirth Group.
Electronic searches
We searched the Cochrane Pregnancy and Childbirth Group’s Trials Register by contacting the Trials Search Co‐ordinator (19 January 2015).
The Cochrane Pregnancy and Childbirth Group’s Trials Register is maintained by the Trials Search Co‐ordinator and contains trials identified from:
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE (Ovid);
weekly searches of Embase (Ovid);
monthly searches of CINAHL (EBSCO);
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL, MEDLINE, Embase and CINAHL, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service can be found in the ‘Specialized Register’ section within the editorial information about the Cochrane Pregnancy and Childbirth Group.
Trials identified through the searching activities described above are each assigned to a review topic (or topics). The Trials Search Co‐ordinator searches the register for each review using the topic list rather than keywords.
Because of the non‐pharmaceutical interventions which are recommended for nausea and vomiting in early pregnancy, we also contacted the Cochrane Complementary Medicine Field's Trials Search Co‐ordinator to identify any other trials in their Trials Register (see:Appendix 1).
Searching other resources
We searched the reference lists of retrieved studies
We did not apply any language or date restrictions.
Data collection and analysis
For methods used in the previous version of this review, seeMatthews 2014.
For this update, the following methods were used for assessing the 21 reports that were identified as a result of the updated search.
The following methods section of this review is based on a standard template used by the Cochrane Pregnancy and Childbirth Group.
Selection of studies
Two review authors independently assessed for inclusion all the potential studies identified as a result of the search strategy. We resolved any disagreement through discussion or, if required, we consulted a third review author.
Data extraction and management
We designed a form to extract data. For eligible studies, two review authors extracted the data using the agreed form. We resolved discrepancies through discussion or, if required, we consulted a third review author. Data were entered into Review Manager software (RevMan 2014) and checked for accuracy.
When information regarding any of the above was unclear, we planned to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Any disagreement was resolved by discussion or by involving a third assessor.
(1) Random sequence generation (checking for possible selection bias)
We described for each included study the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
We described for each included study the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk of bias.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
We described for each included study the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that studies were at low risk of bias if they were blinded, or if we judged that the lack of blinding unlikely to affect results. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
low, high or unclear risk of bias for participants;
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
We described for each included study the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or could be supplied by the trial authors, we planned to re‐include missing data in the analyses which we undertook.
We assessed methods as:
low risk of bias (e.g. no missing outcome data; missing outcome data balanced across groups);
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
low risk of bias (where it is clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review have been reported);
high risk of bias (where not all the study’s pre‐specified outcomes have been reported; one or more reported primary outcomes were not pre‐specified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
We described for each included study any important concerns we had about other possible sources of bias.
(7) Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias, according to the criteria given in the Handbook (Higgins 2011). With reference to (1) to (6) above, we planned to assess the likely magnitude and direction of the bias and whether we considered it likely to impact on the findings. In future updates, we will explore the impact of the level of bias through undertaking sensitivity analyses ‐ see Sensitivity analysis.
Assessment of quality of the evidence
For this update we planned to assess the quality of the evidence using the GRADE approach (Schunemann 2009) in order to assess the quality of the body of evidence relating to the specific outcomes. It was planned that GRADE profiler (GRADEpro 2014) would be used to import data from Review Manager 5.3 (RevMan 2014) in order to create ’Summary of findings’ tables. A summary of the intervention effect and a measure of quality for each of the above outcomes would have been produced using the GRADE approach. The GRADE approach uses five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence for each outcome. The evidence can be downgraded from 'high quality' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates or potential publication bias. However due to the variety in intervention preparations, outcome measurement timing and instruments, a 'Summary of findings' table was not created for this update. This will be re‐examined in future updates.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented results as summary risk ratio with 95% confidence intervals.
Continuous data
We used the mean difference if outcomes were measured in the same way between trials. We used the standardised mean difference to combine trials that measured the same outcome, but used different methods.
Unit of analysis issues
Cluster‐randomised trials
We did not identify any cluster‐randomised trials on this topic. If we had identified such trials, and they were otherwise eligible for inclusion, we would have included them and analysed them with individually‐randomised trials using the methods to adjust event rates and sample sizes set out in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). If we identify such trials for inclusion in future versions of the review, we will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely. We will also acknowledge heterogeneity in the randomisation unit and perform a subgroup analysis to investigate the effects of the randomisation unit.
Cross‐over trials
We did not include any cross‐over trials.
Dealing with missing data
For included studies, we noted levels of attrition. In future updates, if more eligible studies are included, we will explore the impact of including studies with high levels of missing data in the overall assessment of treatment effect by using sensitivity analysis.
For all outcomes, we carried out analyses, as far as possible, on an intention‐to‐treat basis i.e. we attempted to include all participants randomised to each group in the analyses. The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We visually examined the forest plots for each analysis to look for obvious heterogeneity and used the I² and Tau² statistics to quantify statistical heterogeneity among the trials. If we identified moderate or substantial heterogeneity (an I² greater than 50% and a Tau² greater than zero), we used a random‐effects model in meta‐analyses and have indicated the values of I² and Tau² and the P value for the Chi² test for heterogeneity. For outcomes where there are high levels of heterogeneity, we would advise caution in the interpretation of results.
Assessment of reporting biases
In future updates, if there are 10 or more studies in the meta‐analysis, we will investigate reporting biases (such as publication bias) using funnel plots. We will assess funnel plot asymmetry visually. If asymmetry is suggested by a visual assessment, we will perform exploratory analyses to investigate it.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2014). We used fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: i.e. where trials were examining the same intervention, and the trials’ populations and methods were judged sufficiently similar.
If there was clinical heterogeneity sufficient to expect that the underlying treatment effects differed between trials, or if substantial statistical heterogeneity was detected, we used random‐effects meta‐analysis to produce an overall summary if an average treatment effect across trials was considered clinically meaningful. In this update (2015), the majority of analyses were conducted using fixed‐effect. In future updates, where we use random‐effects, the summary will be treated as the average of the range of possible treatment effects and we will discuss the clinical implications of treatment effects differing between trials. If the average treatment effect is not clinically meaningful, we will not combine trials. If we use random‐effects analyses, the results will be presented as the average treatment effect with 95% confidence intervals, and the estimates of Tau² and I².
Subgroup analysis and investigation of heterogeneity
Had we identified substantial heterogeneity, we planned to investigate it using subgroup analyses and sensitivity analyses and to consider whether an overall summary was meaningful, and if it was, to use random‐effects analysis to produce it. In this version of the review, data were not available to carry out the planned subgroup analysis.
In future updates, we will carry out subgroup analyses by type of intervention, where comparability of trials and data allow.
We will use the following primary outcomes in subgroup analysis.
Symptomatic relief (reduction or cessation of nausea, vomiting and/or retching).
Adverse fetal and neonatal outcomes.
Adverse maternal outcomes.
We will assess subgroup differences by interaction tests available within RevMan (RevMan 2014). We will report the results of subgroup analyses quoting the Chi² statistic and P value, and the interaction test I² value.
Sensitivity analysis
We planned to perform sensitivity analyses where appropriate, for example where there was risk of bias associated with the quality of some of the included trials, or to explore the effects of fixed‐effect or random‐effects analyses for outcomes with statistical heterogeneity. However, as studies examined a variety of interventions we were able to pool only very limited data from a small number of studies. In updates of the review, if more data become available we will carry out planned sensitivity analyses.
Results
Description of studies
Results of the search
The search strategy identified 112 reports (66 in the 2010 review, 25 new reports for the 2014 update and 21 new reports in 2015). These reports represented 86 studies (some of the studies resulted in more than one publication). Of the 86 studies, 41 met the inclusion criteria for the review, we excluded 29, eight are awaiting further assessment, and eight studies are ongoing. Four new studies have been included in this update.
Included studies
Participants
All of the studies recruited women with symptoms of nausea (with or without vomiting), although we specifically excluded studies focusing on women with hyperemesis gravidarum. The severity of symptoms was not always made clear, and it is possible that some of the included studies may have recruited some women with more severe symptoms. One study included separate data for those women with the most severe nausea and vomiting (Rosen 2003), though not in a form that allowed us to analyse these separately as part of subgroup analysis.The stage of pregnancy at which women were recruited to studies varied, although predominantly women were recruited during the first trimester (less than 12 weeks’ gestation). In one study (Fan 1995), women with gestational ages of more than eight weeks were included, but the upper limit was not specified. One study recruited women up to 20 weeks (McGuiness 1971), one up to 24 weeks (O'Brien 1996) and one up to 36 weeks (Price 1964). Although most of the women in these trials were in the first trimester and, therefore, we did not wish to exclude the studies, separate figures were not provided on those women with nausea later in pregnancy, and so we were not able to exclude these women from the analyses.
Interventions
The included studies examined a range of interventions.
The effectiveness of acupressure to the P6 acupressure point was examined in seven studies; in five of these the use of acupressure wrist bands was compared with placebo (Belluomini 1994; Khavandizadeh 2010; Norheim 2001; O'Brien 1996; Werntoft 2001), and in one with vitamin B6 (Jamigorn 2007) (in this study women in both groups also received a placebo intervention). One study (Saberi 2014) compared P6 acupressure (via a wristband), ginger and control (no intervention); for the purpose of this review 'no intervention' was considered as placebo. Another study compared acupressure on the KID21 (Youmen) point on the abdomen with sham acupressure on the abdomen (Rad 2012). In that study all women had also taken 40 mg vitamin B6 twice daily.
One study examined the use of acustimulation to the P6 acupressure point (Rosen 2003). Another study compared auricular (on the ear) acupressure with placebo (Puangsricharern 2008). Two trials compared acupuncture with sham acupuncture (Knight 2001; Smith 2002); in one of these (Smith 2002), separate groups received traditional and P6 acupuncture.
The use of ginger (prepared as syrup, capsules or powder within biscuits) to relieve nausea was examined in 13 studies; in five of these ginger was compared with a placebo preparation (Basirat 2009; Keating 2002; Ozgoli 2009; Vutyavanich 2001; Willetts 2003). In three studies ginger was compared with an anti‐emetic (dimenhydrinate) (Pongrojpaw 2007a), metoclopramide (Mohammadbeigi 2011) (and both were compared with placebo) and Doxinate (doxylamine with pyridoxine) (Biswas 2011). In one study (Modares 2012), ginger was compared with chamomile, and both with placebo. As above, Saberi 2014 compared ginger to P6 acupressure and control (no intervention). In four studies the comparison group received vitamin B6 (Chittumma 2007; Ensiyeh 2009; Smith 2004; Sripramote 2003).
Mint oil was compared with placebo in one study (Pasha 2012), and lemon oil inhalation compared with placebo in another study (Yavari 2014).
In two studies the intervention group received vitamin B6 (pyridoxine), which was compared with placebo preparations (Sahakian 1991; Vutyavanich 1995). One study (Wibowo 2012) compared a high dose of vitamin B6 (10 mg) with a low dose of vitamin B6 (1.28 mg) daily. Babaei 2014 compared vitamin B6 to dimenhydrinate.
One study examined the use of moxibustion compared with traditional Chinese herbs (Fan 1995).
Ten studies examined the use of antiemetic drugs: six compared placebo tablets with active treatment (fluphenazine (Price 1964), hydroxyzine hydrochloride (Erez 1971), or thiethylperazine (Newlinds 1964)). Three studies examined doxylamine in various formulations: as dicyclomine, doxylamine and pyridoxine (US trade name, Bendectin) in Geiger 1959; as dicyclomine, doxylamine and pyridoxine (UK trade name, Debendox) in McGuiness 1971; and as doxylamine and pyridoxine (Canadian trade name, Diclectin) in Koren 2010. The three brands are used interchangeably, but earlier preparations of Bendectin contained dicyclomine as well as doxylamine and pyridoxine, as was the case in Geiger 1959 and McGuiness 1971. Oliveira 2014 compared ondansetron with doxylamine‐pyridoxine. One study (Bsat 2003a), looked at the effectiveness of three different anti‐emetics (metoclopramide with vitamin B6, prochlorperazine and promethazine) and another study (Ghahiri 2011) compared ondansetron with metoclopramide. One study compared low and high doses of pyridoxine hydrochloride (Wibowo 2012).
Outcomes
All of the studies collected outcome data on persistence of nausea symptoms or relief from nausea. Nevertheless, pooling data from studies was complicated by the variability in the way outcome data were collected and reported. The Pregnancy Unique Quantification of Emesis (PUQE) scale was used in three studies (Koren 2010; Wibowo 2012; Yavari 2014). The Rhodes Index of Nausea, Vomiting and Retching was used in 13 studies (Babaei 2014; Belluomini 1994; Chittumma 2007; Jamigorn 2007; Modares 2012; Mohammadbeigi 2011; O'Brien 1996; Puangsricharern 2008; Rosen 2003; Saberi 2014; Smith 2002; Smith 2004; Willetts 2003). Not all studies collected or reported data on all dimensions (duration, frequency, distress) of the three subscales (nausea, vomiting, retching) included in the index. In eight studies ordinal data were collected (Bsat 2003a; Erez 1971; Fan 1995; Geiger 1959; Knight 2001; McGuiness 1971; Newlinds 1964; Price 1964). In these studies women were asked, for example, to rate symptoms on a five‐point Likert‐type scale or to describe the relief from symptoms on a three‐point scale. We have converted some of the data from studies using such scales into binary data to incorporate them into the review.
In 17 studies a visual analogue scale (VAS) was used (Keating 2002; Knight 2001) (for overall effectiveness rating); Khavandizadeh 2010; Basirat 2009; Biswas 2011; Ensiyeh 2009; Norheim 2001; Oliveira 2014; Ozgoli 2009; Pasha 2012; Pongrojpaw 2007a; Rad 2012; Sahakian 1991; Sripramote 2003; Vutyavanich 1995; Vutyavanich 2001; Werntoft 2001). The wording on each VAS differed slightly, though in most cases women were asked to rate their symptoms on a 10 cm (or 100 mm) line, with zero representing no symptom(s) (for example, no nausea) and 10 representing the worst symptom(s) (for example, the worst possible nausea). No authors provided details of validity or reliability testing of the VAS used. One study reported frequency of nausea episodes (Ghahiri 2011).
Many studies reported the number of vomiting episodes recorded by women each day (Basirat 2009; Biswas 2011; Bsat 2003a; Ensiyeh 2009; Ghahiri 2011; Keating 2002; Ozgoli 2009; Pongrojpaw 2007a; Rad 2012; Sahakian 1991; Sripramote 2003; Vutyavanich 1995; Vutyavanich 2001; Werntoft 2001), in addition to those above that used the Rhodes Index, which also measures frequency of vomiting. One study used 'East Oncology' criteria for rating severity of vomiting (Khavandizadeh 2010). One study measured the use of rescue medication (Jamigorn 2007), and two others the use of over‐the‐counter and prescribed medication (Puangsricharern 2008; Rosen 2003). One study measured continued (blinded) use of medication following the trial and concurrent use of alternate therapies such as aromatherapy and yoga (Koren 2010).
In this review we chose to describe outcomes relating to women's experience of nausea and vomiting at approximately three days after the start of treatment, as many of the studies provided data at this time point. We judged that this was a clinically meaningful point as most medication and other interventions would be expected to have achieved some effect within this timeframe. Where this information was not available, we chose the closest time point to three days that was reported. In the Characteristics of included studies tables, we have set out the time points when outcome data on symptoms were collected and reported in relation to the commencement of treatment. This information is important, as for many women symptoms are likely to resolve over time with or without treatment, particularly as the pregnancy progresses beyond the first trimester. In studies where outcome data were collected weekly over three or four weeks (e.g. Ghahiri 2011; Smith 2002; Smith 2004), we considered that differences between groups would be more difficult to detect at later follow‐up points, and for these studies we have used symptom data from the earlier assessments (e.g. after seven days) in the data and analyses tables. Some studies included only later time points and therefore we have reported these (e.g. Koren 2010; Wibowo 2012).
As well as symptomatic relief, our primary outcomes also included maternal and fetal/neonatal adverse effects. Six studies reported adverse fetal outcomes (Ensiyeh 2009; Erez 1971; Koren 2010; Smith 2002; Vutyavanich 2001; Willetts 2003). Adverse maternal outcomes (such as preterm labour or spontaneous abortion) were reported for six studies (Ensiyeh 2009; Koren 2010; Smith 2002; Smith 2004; Vutyavanich 2001; Willetts 2003). Worsening of symptoms was reported in two studies (Bsat 2003a; Rosen 2003). Three studies reported on maternal weight loss/gain, which we had not prespecified as a maternal outcome (Jamigorn 2007; Keating 2002; Rosen 2003); this could be viewed as being related to symptom control, but is presented with the secondary outcomes in the results section. In addition, 10 studies described the side effects of treatment such as headache, heartburn or sleepiness (Babaei 2014; Chittumma 2007; Erez 1971; Ghahiri 2011; Koren 2010; Knight 2001; McGuiness 1971; Pongrojpaw 2007a; Sripramote 2003; Willetts 2003).
Our secondary outcomes included quality of life of women during pregnancy, and economic costs (directly to women, productivity costs, and costs to the healthcare system). Two studies (Smith 2002; Smith 2004) measured Quality of LIfe using the MOS 36 Short Form Health Survey (SF36). One study (Knight 2001) used the Hospital Anxiety and Depression Scale. One study measured subjective feeling of well‐being (using a binary yes/no response) (Biswas 2011). One study (Koren 2010) measured economic costs, as time loss from employment.
See the Characteristics of included studies tables for more information on participants, interventions and outcomes measured.
Studies awaiting further assessment and ongoing studies
Eight studies are awaiting further assessment; all of these were reported in brief abstracts, and our initial attempts to contact authors, or to identify subsequent publications were not successful (Adamczak 2007; Babaee 2010; Hsu 2003; Mamo 1995; Paridokht 2010; Smith 1991). We were unable to translate two studies (Abedian 2014; Narenji 2014) for this update and the abstracts in English did not contain enough data for inclusion of the study. If we identify further reports from these studies we will re‐assess eligibility.
Eight studies are ongoing. Seven of these are registered with the Iranian Registry of Clinical Trials (IRCT) (Dehkordi 2013; Faramarzi 2013; Farhadifar 2011; Keshavarz 2014; Ozgoli 2011; Ozgoli 2014; Safajou 2014). All authors have been contacted and no results for these studies are available as of March 2015. The studies registered with IRCT cover a range of interventions with the following comparisons: Cydonia oblonga (quince) versus vitamin B6 (Dehkordi 2013); ondansetron versus psychotherapy versus control (Faramarzi 2013); ginger versus metoclopramide versus placebo (Farhadifar 2011); lavender versus mint oil versus placebo (Keshavarz 2014); cardamom versus placebo (Ozgoli 2011). Koren 2014 is comparing Diclegis versus placebo for adolescents and Ozgoli 2014; is comparing inhaled peppermint aroma with a control group using aromatherapy with sweet almond oil.
Excluded studies
After assessment of study eligibility we excluded 29 studies identified by the search strategy, for reasons described in the Characteristics of excluded studies tables. The main reason we excluded studies was because they were not randomised trials, or they used a cross‐over design. Seven studies used quasi‐randomised designs, for example, allocation according to day of the week, registration number, visit date, or alternate allocation (Baum 1963; Can Gurkan 2008; Diggory 1962; Dundee 1988; Fitzgerald 1955; Liu 2014; Winters 1961); such studies are at high risk of bias, and therefore were not included in the review. Two studies were single‐arm trials (Reyhani 2013; Shahbazzadegan 2006). In three studies it was not clear to us that there was any sort of random allocation to groups (Conklin 1958; Lask 1953; Steele 2001). Eight studies used a cross‐over design (Anjum 2002; Bayreuther 1994; Cartwright 1951; De Aloysio 1992; Evans 1993; Hyde 1989; King 1955; Wheatley 1977); such designs are not usually appropriate during pregnancy when symptoms may not be stable over time.
We excluded five studies as they focused on women with hyperemesis gravidarum, a group that we had decided to exclude from the review (Heazell 2006; Mehrolhasani 2012; McCarthy 2014; Kadan 2009; Pasha 2010). Two of these studies are ongoing (Kadan 2009; Pasha 2010). We excluded one study because it was reported in a trial registry, and we found no evidence that the study had taken place; we carried out a search of databases to look for any publications from the study without success (Luz 1987). One study did not focus on the relief of nausea, but rather on hypocorticalism in pregnancy (Ferruti 1982); and finally, one trial record describes a study that looked at pre‐emptive treatment (before any symptoms appear) with a combination of pyridoxine hydrochloride and doxylamine succinate (Diclectin) in a subsequent pregnancy for women who had experienced severe symptoms of nausea/vomiting of pregnancy (or hyperemesis gravidarum) in a previous pregnancy (Koren 2006).
Risk of bias in included studies
The risk of bias was assessed for all studies and results were mixed across the domains of bias. Selection bias risk was unclear for many studies. Risk of bias was low related to performance bias, detection bias and attrition bias for most studies. Almost half of the studies did not fully or clearly report all pre‐specified outcomes (reporting bias), while only a few studies were assessed to have other sources of bias.
Allocation
Sequence generation
In 14 of the included studies the method used to generate the randomisation sequence was not described or was not clear (Babaei 2014; Erez 1971; Fan 1995; Geiger 1959; Ghahiri 2011; Khavandizadeh 2010; McGuiness 1971; Mohammadbeigi 2011; Newlinds 1964; Ozgoli 2009; Pongrojpaw 2007a; Price 1964; Rad 2012; Werntoft 2001). The study by Belluomini 1994 was described as having a balanced block design, but it was not clear how the sequence order was generated or what the block size was; we have assessed this trial as low risk.
All the remaining studies were assessed as having adequate methods to generate the randomisation sequence and low risk of bias: five studies used external randomisation services (Jamigorn 2007; Koren 2010; Smith 2002; Smith 2004; Willetts 2003), 10 studies used computer‐generated sequences (Biswas 2011; Bsat 2003a; Keating 2002; Knight 2001; O'Brien 1996; Oliveira 2014; Pasha 2012; Rosen 2003; Wibowo 2012; Yavari 2014) (although the small block size in the Knight 2001 study (four) may have meant the sequence could be anticipated); and the remaining nine studies reported the use of tables of random numbers (Basirat 2009; Chittumma 2007; Ensiyeh 2009; Puangsricharern 2008; Saberi 2014; Sahakian 1991; Sripramote 2003; Vutyavanich 1995; Vutyavanich 2001). One study (Modares 2012) reported allocation by 'lottery using coloured cards', implying random sequence generation. One study (Norheim 2001) used block randomisation in blocks of 20.
Allocation concealment
In 25 studies the methods used to conceal the study group allocation were not described or were not clear (Babaei 2014; Belluomini 1994; Biswas 2011; Bsat 2003a; Ensiyeh 2009; Erez 1971; Fan 1995; Geiger 1959; Ghahiri 2011; Keating 2002; Khavandizadeh 2010; Modares 2012; Mohammadbeigi 2011; Newlinds 1964; Norheim 2001; Ozgoli 2009; Pasha 2012; Pongrojpaw 2007a; Price 1964; Puangsricharern 2008; Rad 2012; Saberi 2014; Sahakian 1991; Werntoft 2001; Wibowo 2012). One study used coloured cards, but it is not clear how they were used (Modares 2012). In the remaining studies, we judged that the methods were adequate and of low risk of bias; five studies used an external randomisation service (Jamigorn 2007; Koren 2010; Smith 2002; Smith 2004; Willetts 2003); six used sealed opaque sequentially numbered envelopes (Chittumma 2007; Knight 2001; O'Brien 1996; Rosen 2003; Sripramote 2003; Vutyavanich 2001); in six placebo‐controlled trials, coded drug boxes, packaging or containers were used (Basirat 2009; McGuiness 1971; Oliveira 2014; Price 1964; Vutyavanich 1995; Yavari 2014).
Blinding
Most of the studies included in the review were placebo‐controlled and of low risk of bias. Some studies were of high risk of bias, where blinding was not possible or not attempted. In one study the medications compared had different shapes and therefore blinding was not possible (Ghahiri 2011). In two studies the routes of treatment administration (oral, injection, etc.) were different and double/multiple placebo control was not attempted (Bsat 2003a; Fan 1995). In two studies (O'Brien 1996; Werntoft 2001) there were three arms: intervention, placebo and no treatment, so blinding was not possible for the 'no treatment group'. Puangsricharern 2008 and Saberi 2014 did not attempt blinding.
The success of blinding was not reported in most trials. Where the treatment involved acupressure, acustimulation, or acupuncture, blinding may not have been convincing to women or clinical staff. In one acupuncture trial (Knight 2001), the author reported that there was no attempt to blind clinical staff, but women were described as being blind to group allocation. In five studies, the authors examined whether blinding was actually effective. In two of these (Chittumma 2007; Knight 2001) blinding appeared to be effective (assessed as low risk) while in the other three (Norheim 2001; Smith 2002; Smith 2004) women seemed aware of their group allocation, and risk of bias for these was judged as being unclear. Yavari 2014 was assessed as of unclear risk of performance bias due to the intervention having a lemon scent and the control having no scent.
In all studies, all symptomatic outcomes were self‐assessed by women, whether recorded by women themselves or a researcher, making triple blinding impossible. On this basis, all studies had low risk of detection bias.
Incomplete outcome data
The amount of missing outcome data in most of these studies was generally low, with attrition levels below 10%; in these studies most women were available for follow‐up, although there were missing data for some outcomes. The reasons for attrition in studies with relatively low rates of loss to follow‐up varied and five studies stated that women were lost to follow‐up for reasons that may have related to study outcomes (e.g. because they developed more severe symptoms, did not comply with taking study medication, or had adverse events) (Bsat 2003a; Jamigorn 2007; Keating 2002; O'Brien 1996). These are judged as low risk due the low attrition rate.
Studies judged to be at high risk of attrition bias had rates of attrition of 20% or higher. They were: Knight 2001 (20%), Newlinds 1964 (20%), Sahakian 1991 (20.2%, attrition per group not stated), Smith 2002 (24% by week four of a four‐week study) and Belluomini 1994 (33%). In one study (McGuiness 1971), the number of women randomised was not clear, making it impossible for us to assess attrition. In another study (Werntoft 2001), the approximate number of questionnaires (n = 80) given out was stated, and the study stopped when 20 per group returned them, but it is not known how many per group had been given out, and therefore, attrition cannot be accurately measured. In one study (Modares 2012), it was stated that those who dropped out from the study were replaced by a new member, though it does not state the timing or extent of such replacements, and the risk of bias is judged as unclear.
Intention‐to‐treat (ITT) analysis was reported for two studies (Jamigorn 2007 (dropouts counted as treatment failures) and Knight 2001). Vutyavanich 2001 included three placebo dropout participants in the results, assuming relief equal to best improvement in the placebo group.
Selective reporting
Almost half of the included studies did not fully or clearly report all pre‐specified outcomes and were judged to be at high risk of reporting bias. Not all subscales were reported for instruments such as the Rhodes Index (Belluomini 1994) or other measures (Ensiyeh 2009; Knight 2001). Data from only selected time points (often start and end points, which vary considerably across trials) were presented in some studies (Belluomini 1994; Keating 2002; Khavandizadeh 2010; Koren 2010; Modares 2012; Wibowo 2012). For Koren 2010, data were recorded daily but only PUQE score changes from baseline to end point (at 15 days) were reported, though 'day by day area under the curve for change in PUQE from baseline' was also reported. In one study, results were presented using the number of assessments of outcomes (280 assessments for 35 participants in the control group and 256 assessments for 32 participants in treatment group), rather than the number of participants (Ozgoli 2009). Statements in the text about results were not always backed up with numerical results (e.g. Belluomini 1994 (re results from days eight to 10); Bsat 2003a (re drug use and compliance). As stated above (Included studies), few studies described side effects from treatment or adverse events for mothers or babies. In six studies we had difficulty interpreting outcome data as they were presented only, or largely, in graphical form (Bsat 2003a; Jamigorn 2007; Norheim 2001; O'Brien 1996; Pasha 2012; Willetts 2003). Some studies (Pongrojpaw 2007a; Sahakian 1991; Smith 2002) provided a large amount of outcome data, for example, mean scores on several dimensions of scales recorded over several days. Interpreting such data is not simple, and increases the risk of spurious statistically significant findings. For Rosen 2003 the results for participants with mild to severe symptoms were presented together and it is unclear if this introduces bias in reporting; also some results are only reported in graphical form.
Other potential sources of bias
One study judged to be at high risk stopped early; in this trial it was stated that approximately 80 women were randomised, but the study was ended when 20 women in each of three groups had returned their data collection forms (Werntoft 2001).
Other studies were of unclear risk of bias: in the Price 1964 trial, some baseline imbalance between study groups in terms of gestational age at recruitment was reported, and in the Puangsricharern 2008 study there were differences in baseline demographic characteristics, with the control group participants having higher education and income levels than the treatment group. In one study (Geiger 1959), two women were included in both the treatment and control groups, as they received medication on two separate occasions when they visited the clinic during the study period. In several studies (for example, Jamigorn 2007 and Rosen 2003), women were free to take other medication, which may have had a bearing on outcomes; without information on what other medication women were using, it is difficult to interpret these data. Chittumma 2007 reported that women took additional ginger and anti‐emetic products during the trial. Smith 2002 only reported that women in the control group received vitamin B6 advice and it is not clear if the intervention group also received this advice. In the Bsat 2003a study, two drugs were given to Group A; this treatment was found to be most effective; it is not possible to identify whether one or both agents were effective. The authors note that combining two agents that may also both work independently may raise questions of fairness ‐ this was done to mirror local practices; it was unclear who and where drugs were administered (e.g. intramuscular (IM) injections on an "as required" basis). In Willetts 2003 it is stated in the discussion that treatment continued for ginger group for eight days and the placebo group took ginger for four days and all were given two weeks' supply following the end of the trial. Only the data for four days were analysed, hence the findings of the follow‐up assessment (for the 81 women who completed the main study) should be viewed with caution. No direct attempt can be made to infer cause or association between the findings and the use of ginger over the eight‐day period of the principal study.
Figure 1 and Figure 2 show the summary and graph of methodological quality, respectively. These highlight that, across studies, low risk of bias for most studies on several criteria such as performance, detection, attrition and other sources of bias. There is a lack of clarity on some 'Risk of bias' criteria, particularly in relation to selection and reporting bias.
1.
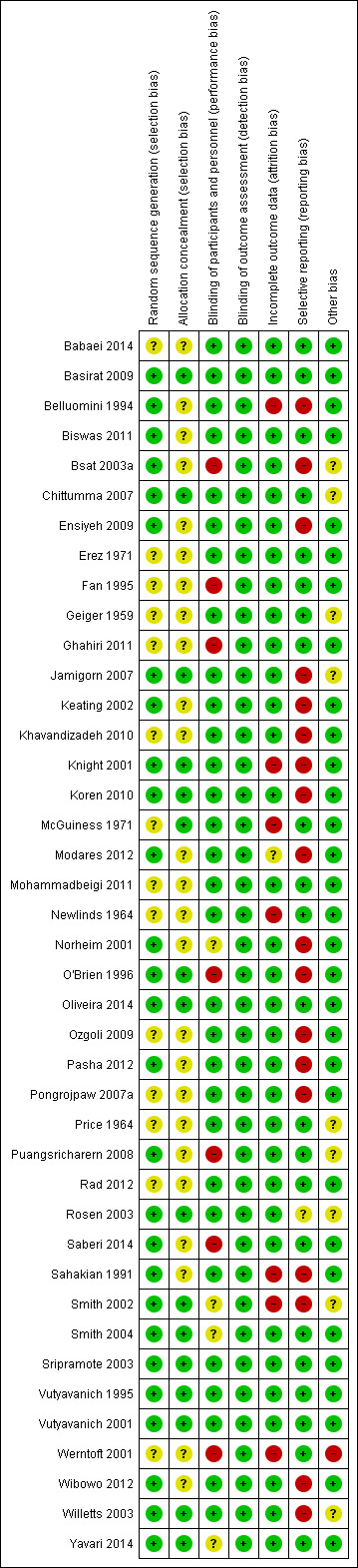
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
2.
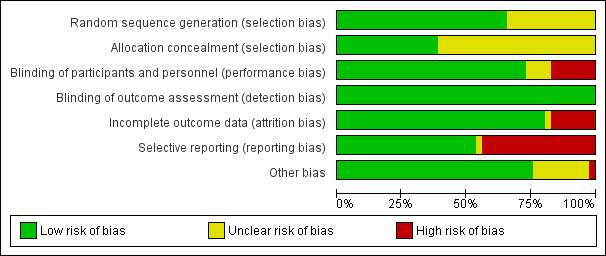
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
Effects of interventions
Interventions for nausea and vomiting in early pregnancy: 41 studies with 5449 women
Primary outcomes
The primary outcomes for this review were as follows.
Symptomatic relief (specifically a reduction or cessation in nausea, retching and/or vomiting).
-
Adverse maternal and fetal/neonatal outcomes.
Adverse maternal outcomes included pregnancy complications (antepartum haemorrhage, hypertension, pre‐eclampsia).
Adverse fetal/neonatal outcomes included fetal or neonatal death, congenital abnormalities, low birthweight or early preterm birth.
Secondary outcomes
The secondary outcomes for this review were as follows.
Quality of life
Economic costs
P6 Acupressure versus placebo (five studies with 601 women)
Six studies (Belluomini 1994; Khavandizadeh 2010; Norheim 2001; O'Brien 1996; Saberi 2014; Werntoft 2001) compared P6 acupressure to placebo, and we have included data from five of these in the data tables.
Primary outcomes
Symptomatic relief
One study with 100 women showed evidence of a statistically significant effect for acupressure (Khavandizadeh 2010), on severity of nausea (mean difference (MD) ‐1.70, 95% confidence interval (CI) ‐2.41 to ‐0.99, Analysis 1.1) and vomiting (MD ‐0.90, 95% CI ‐1.06 to ‐0.74, Analysis 1.7) after four days of treatment.
1.1. Analysis.
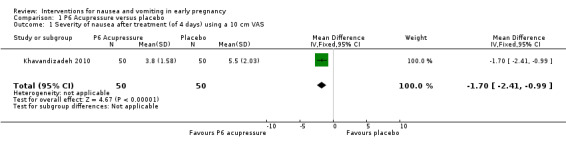
Comparison 1 P6 Acupressure versus placebo, Outcome 1 Severity of nausea after treatment (of 4 days) using a 10 cm VAS.
1.7. Analysis.
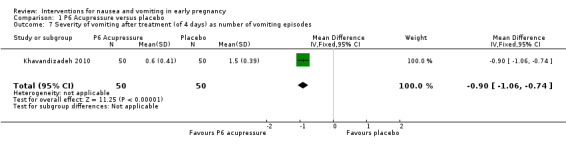
Comparison 1 P6 Acupressure versus placebo, Outcome 7 Severity of vomiting after treatment (of 4 days) as number of vomiting episodes.
Results from another study with data for 97 women (Norheim 2001), found no statistically significant difference between groups for improving (i.e. reducing) the intensity of symptoms (risk ratio (RR) 0.78, 95% CI 0.44 to 1.39, Analysis 1.2). After three days of treatment there was no strong evidence that, compared with placebo, the treatment improved nausea in the Werntoft 2001 trial, 40 women (MD 0.10, 95% CI ‐1.49 to 1.69, Analysis 1.3). Similarly, results from Saberi 2014 in a study of 93 women comparing P6 acupressure to no intervention (and ginger, reported below) found no statistically significant difference on total Rhodes Index score on day three of intervention (MD ‐1.48, 95% ‐4.10 to 1.14, Analysis 1.6). Using scores averaged over one to three days for 60 women, results from the Belluomini 1994 study did not show that acupressure improved scores on the nausea and vomiting subscales, or on the total Rhodes Index score (for nausea MD 0.39, 95% CI ‐0.80 to 1.58, Analysis 1.4, for vomiting MD 0.26, 95% CI ‐1.06 to 1.58, Analysis 1.8, for total Rhodes score MD 1.17, 95% CI ‐1.52 to 3.86, Analysis 1.5).
1.2. Analysis.
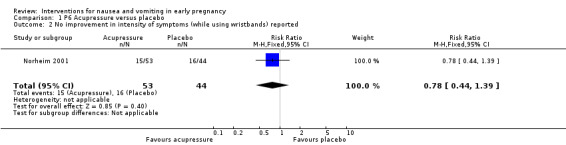
Comparison 1 P6 Acupressure versus placebo, Outcome 2 No improvement in intensity of symptoms (while using wristbands) reported.
1.3. Analysis.
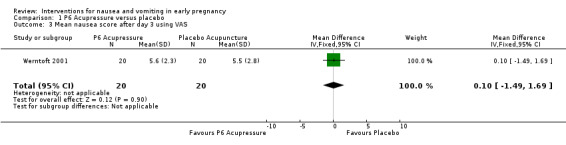
Comparison 1 P6 Acupressure versus placebo, Outcome 3 Mean nausea score after day 3 using VAS.
1.6. Analysis.
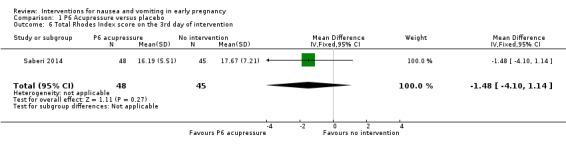
Comparison 1 P6 Acupressure versus placebo, Outcome 6 Total Rhodes Index score on the 3rd day of intervention.
1.4. Analysis.
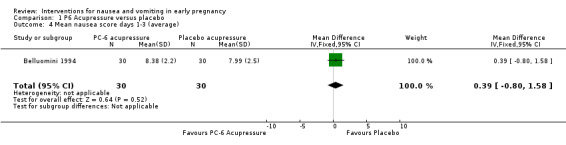
Comparison 1 P6 Acupressure versus placebo, Outcome 4 Mean nausea score days 1‐3 (average).
1.8. Analysis.
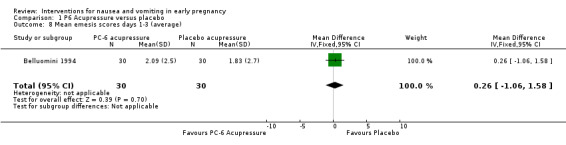
Comparison 1 P6 Acupressure versus placebo, Outcome 8 Mean emesis scores days 1‐3 (average).
1.5. Analysis.
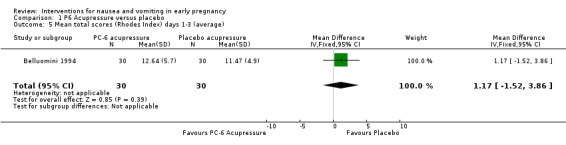
Comparison 1 P6 Acupressure versus placebo, Outcome 5 Mean total scores (Rhodes Index) days 1‐3 (average).
One further study (O'Brien 1996) compared P6 acupressure and placebo, but data from this study were not in a form that allowed us to enter them into RevMan tables. The authors reported no statistically significant differences between treatment and placebo groups for symptom relief.
Adverse maternal and fetal/neonatal outcomes
Only one study reported adverse maternal outcomes, and none fetal/neonatal outcomes. Norheim 2001 reported that 63% of participants in the acupressure group and 90% in the placebo group reported problems (including pain, numbness, soreness and hand‐swelling) using the wristband. Three women (two in the treatment group, one in the placebo group) said they felt more sick during the study period.
Secondary outcomes
Quality of life
No studies reported quality of life outcomes.
Economic costs
No studies reported economic costs.
P6 Acupressure versus vitamin B6 (one study with 66 women)
Primary outcomes
Symptomatic relief
Jamigorn 2007 compared P6 acupressure with vitamin B6 and the results showed no statistically significant difference between the two interventions for improvement of nausea on day three (data obtained from authors) (MD 0.20, 95% CI ‐2.24 to 2.64, Analysis 2.1). The authors also reported on the use of rescue medication (which may be a proxy measure for lack of symptom relief); results favoured P6 acupressure (MD ‐2.20, 95% CI ‐3.98 to ‐0.42, Analysis 2.2).
2.1. Analysis.
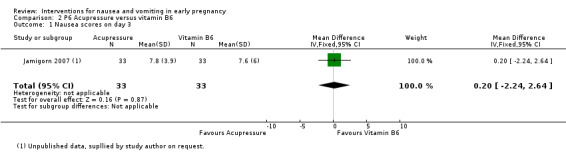
Comparison 2 P6 Acupressure versus vitamin B6, Outcome 1 Nausea scores on day 3.
2.2. Analysis.
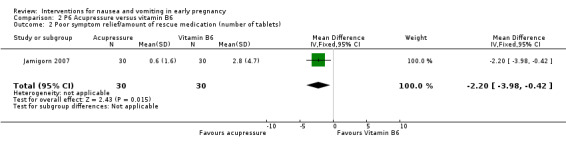
Comparison 2 P6 Acupressure versus vitamin B6, Outcome 2 Poor symptom relief/amount of rescue medication (number of tablets).
Adverse maternal and fetal/neonatal outcomes
No adverse maternal or fetal/neonatal outcomes were reported.
Secondary outcomes
Quality of life
No studies reported quality of life outcomes.
Economic costs
No studies reported economic costs.
KID21 point (Youmen) acupressure versus sham acupressure (one study with 80 women)
Primary outcomes
Symptomatic relief
One study (Rad 2012) compared Youmen acupressure with sham acupressure, but as only medians and interquartile ranges (IQRs) are reported, data could not be entered into RevMan 2014 analyses tables.The authors reported a statistically significant difference favouring Youmen acupressure over sham acupressure, on day four.
Adverse maternal and fetal/neonatal outcomes
Adverse maternal and fetal/neonatal outcomes were not reported.
Secondary outcomes
Quality of life
Quality of life outcomes were not reported.
Economic costs
Economic costs were not reported.
Auricular acupressure versus placebo (one study with 91 women)
Primary outcomes
Symptomatic relief
One study compared auricular acupressure (administered by participants by pressing on magnetic balls taped to an acupressure point on the ear) with placebo (no treatment) (Puangsricharern 2008). The authors reported that they used mean total Rhodes Index score and total number of vomiting episodes from days four to six to measure treatment effect. They subsequently concluded that there were no significant differences between groups (though average Rhodes scores across these days were not directly reported). The treatment started on day three (for the acupressure group) and the results for the total Rhodes score at day six (three days after treatment started) appeared to favour the treatment group, although scores were lower in this group at baseline so results are difficult to interpret (MD ‐3.60, 95% CI ‐6.62 to ‐0.58, Analysis 3.1). There were no differences between groups for the number of anti‐emetic drugs used (MD ‐ 0.10, 95% CI ‐0.37 to 0.17, Analysis 3.2).
3.1. Analysis.
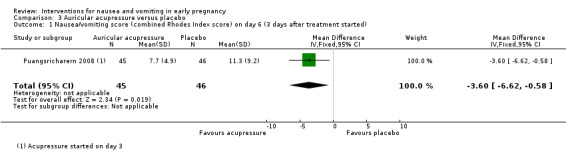
Comparison 3 Auricular acupressure versus placebo, Outcome 1 Nausea/vomiting score (combined Rhodes Index score) on day 6 (3 days after treatment started).
3.2. Analysis.
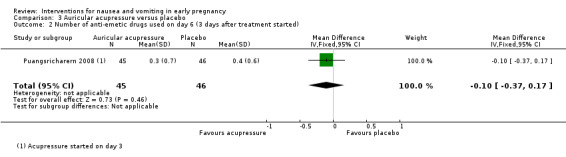
Comparison 3 Auricular acupressure versus placebo, Outcome 2 Number of anti‐emetic drugs used on day 6 (3 days after treatment started).
Adverse maternal and fetal/neonatal outcomes
Adverse maternal and fetal/neonatal outcomes were not reported.
Secondary outcomes
Quality of life
Quality of life outcomes were not reported.
Economic costs
Economic costs were not reported.
Acustimulation versus placebo (one study with 230 women)
Primary outcomes
Symptomatic relief
Rosen 2003 compared low‐level nerve stimulation therapy over the volar aspect of the wrist at the P6 point with placebo. In this study, nausea symptoms were recorded over three weeks, with weekly assessments of changes from baseline. The author reported the "time‐averaged" change in the Rhodes Index total experience scale over the entire three‐week study period, and suggested that there was more improvement over time in the active treatment group (change score 6.48 (95% CI 5.31 to 7.66) versus 4.65 (95% CI 3.67 to 5.63) in the placebo group (data not shown in analysis tables). In this study, both groups experienced improved scores over the evaluation period, and data (presented in graphical form in the study report) were not simple to interpret. Results for women in the Rosen 2003 study with mild to moderate symptoms were described in an abstract by De Veciana 2001, and in another brief abstract results were reported for those women with severe symptoms (Miller 2001). However, neither abstract provided usable data for subgroup analysis.
Adverse maternal and fetal/neonatal outcomes
Rosen 2003 reported on weight gain, dehydration and ketonuria. There was significantly more weight gain and less dehydration in the treatment group (MD 1.70, 95% CI 0.23 to 3.17, Analysis 4.1; RR 0.24, 95% CI 0.07 to 0.83, Analysis 4.2, respectively), but there was no significant difference for ketonuria at the end of the trial period (RR 0.48, 95% CI 0.15 to 1.55, Analysis 4.3). The authors reported that there was no significant difference between groups on entry to the trial for ketonuria, though those most likely to withdraw from the study had ketonuria at entry (but at a non‐significant level).
4.1. Analysis.
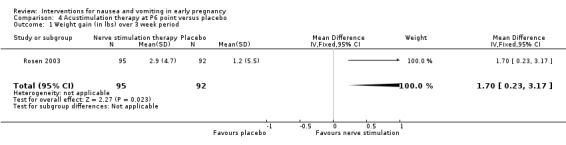
Comparison 4 Acustimulation therapy at P6 point versus placebo, Outcome 1 Weight gain (in lbs) over 3 week period.
4.2. Analysis.
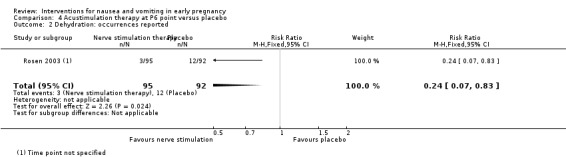
Comparison 4 Acustimulation therapy at P6 point versus placebo, Outcome 2 Dehydration: occurrences reported.
4.3. Analysis.
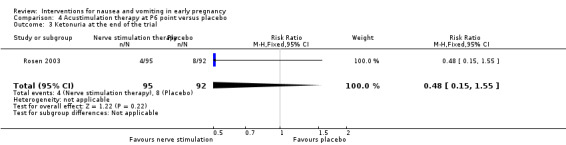
Comparison 4 Acustimulation therapy at P6 point versus placebo, Outcome 3 Ketonuria at the end of the trial.
Secondary outcomes
Quality of life
Quality of life outcomes were not reported.
Economic costs
Economic costs were not reported.
Acupuncture versus placebo (two studies with 648 women)
Primary outcomes
Symptomatic relief
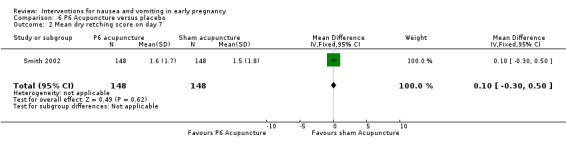
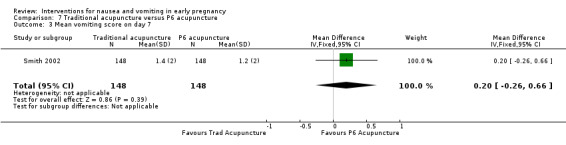
One trial with data for 296 women compared traditional acupuncture, P6 acupuncture, sham acupuncture and no treatment (Smith 2002). The data tables show three comparisons: between both traditional and P6 acupuncture and sham acupuncture, and between traditional and P6 acupuncture. Most of the results show no significant differences (Analysis 5.2; Analysis 5.3; Analysis 6.1; Analysis 6.2; Analysis 6.3; Analysis 7.1; Analysis 7.2; Analysis 7.3) for relief from nausea, dry retching and vomiting. Knight 2001 also compared acupuncture versus placebo but the data were not in a form that allowed us to enter them in RevMan 2014 analyses tables; the authors used median scores because of the skewness of the data. They report no statistically significant differences between the control and intervention groups for symptom relief.
5.2. Analysis.
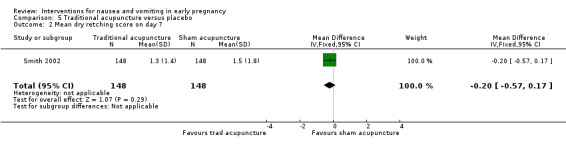
Comparison 5 Traditional acupuncture versus placebo, Outcome 2 Mean dry retching score on day 7.
5.3. Analysis.
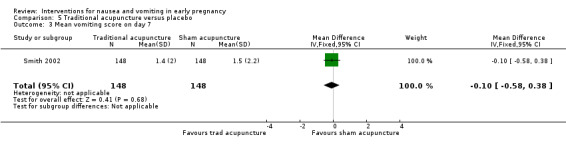
Comparison 5 Traditional acupuncture versus placebo, Outcome 3 Mean vomiting score on day 7.
6.1. Analysis.
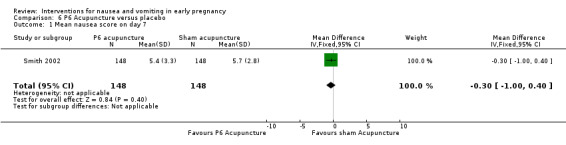
Comparison 6 P6 Acupuncture versus placebo, Outcome 1 Mean nausea score on day 7.
6.2. Analysis.
Comparison 6 P6 Acupuncture versus placebo, Outcome 2 Mean dry retching score on day 7.
6.3. Analysis.
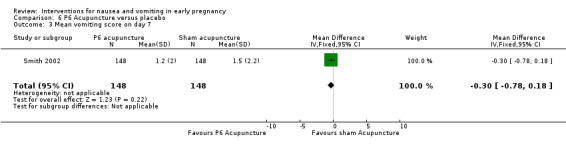
Comparison 6 P6 Acupuncture versus placebo, Outcome 3 Mean vomiting score on day 7.
7.1. Analysis.
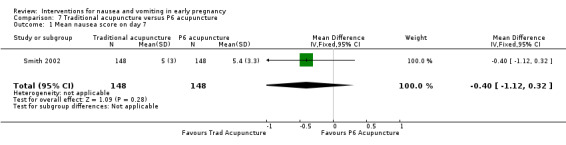
Comparison 7 Traditional acupuncture versus P6 acupuncture, Outcome 1 Mean nausea score on day 7.
7.2. Analysis.
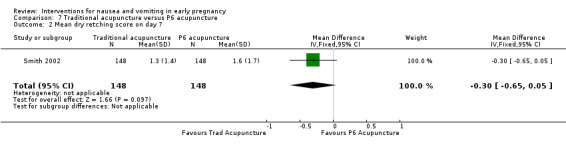
Comparison 7 Traditional acupuncture versus P6 acupuncture, Outcome 2 Mean dry retching score on day 7.
7.3. Analysis.
Comparison 7 Traditional acupuncture versus P6 acupuncture, Outcome 3 Mean vomiting score on day 7.
Adverse maternal and fetal/neonatal outcomes
No adverse maternal or fetal/neonatal outcomes were reported.
Secondary outcomes
Quality of life
Smith 2002 and Smith 2004 used the MOS 36 Short Form Health Survey. Smith 2002 reported the change in mean scores on the SF36 Form (Quality of Life) for the four groups receiving traditional acupuncture, P6 acupuncture, sham acupuncture and no treatment, respectively. They reported eight sets of results for three time points and highlighted that there was a group effect on the social function and mental health SF36 domains, favouring traditional acupuncture in both cases. Smith 2004 also reported changes in mean scores across eight domains of the SF‐36, with a significant difference, favouring ginger, found only in two domains: social function and physical role function.
Knight 2001 used the Hospital Anxiety and Depression Scale (HADS) and reported median scores for the intervention and control groups, but the data were not in a form that allowed us to enter them in RevMan 2014 analyses tables. The authors reported that for both anxiety and depression scores, there was no evidence for a group effect or a group‐time effect, but there was for a time effect (in favour of acupuncture). However, both scores dropped over the course of the study for both groups. The median rating of global effectiveness was the same for both groups.
Economic costs
Neither study reported economic costs.
Moxibustion versus Chinese drugs (one study with 302 women)
Primary outcomes
Symptomatic relief
Fan 1995 reported that in a study comparing moxibustion with Chinese drugs, symptoms for all women in both groups either "improved" or were "cured".
Adverse maternal and fetal/neonatal outcomes
Adverse maternal and fetal/neonatal outcomes were not reported.
Secondary outcomes
Quality of life
Quality of life outcomes were not reported.
Economic costs
Economic costs were not reported.
Ginger versus placebo (seven studies with 578 women)
Ginger was compared with placebo in eight studies (Basirat 2009; Keating 2002; Modares 2012; Mohammadbeigi 2011; Ozgoli 2009; Saberi 2014 ; Vutyavanich 2001; Willetts 2003), although one study did not provide data on symptomatic relief in a way which we could use (Willetts 2003).
Primary outcomes
Symptomatic relief
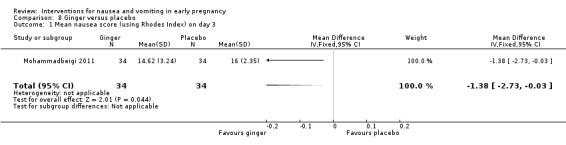
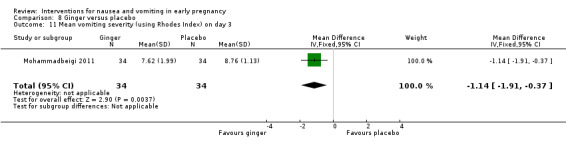
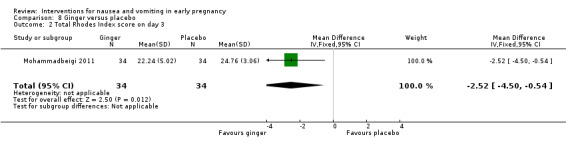
In a study with data for 68 women comparing ginger versus placebo (and metoclopramide, discussed below) (Mohammadbeigi 2011), ginger was favoured over placebo for mean nausea score (MD ‐1.38, 95% CI ‐2.73 to ‐0.03, Analysis 8.1) and mean vomiting score (MD ‐1.14, 95% CI ‐1.91 to ‐0.37, Analysis 8.11), and overall Rhodes index score (MD ‐2.52, 95% CI ‐4.50 to 0.54, Analysis 8.2); all reported on day three. Modares 2012 also compared ginger and placebo (and chamomile, discussed below), and results favoured ginger (MD ‐4.19, 95% CI ‐6.65 to ‐1.73, data for 70 women, Analysis 8.4) one week after treatment, using Rhodes Index overall score. In a study with a small sample size (n = 26) (Keating 2002), results favoured ginger over placebo for improving nausea by day nine (RR 0.29, 95% CI 0.10 to 0.82, Analysis 8.5). Results also favoured ginger for stopping vomiting at day six (RR 0.42, 95% CI 0.18 to 0.98, Analysis 8.12).
8.1. Analysis.
Comparison 8 Ginger versus placebo, Outcome 1 Mean nausea score (using Rhodes Index) on day 3.
8.11. Analysis.
Comparison 8 Ginger versus placebo, Outcome 11 Mean vomiting severity (using Rhodes Index) on day 3.
8.2. Analysis.
Comparison 8 Ginger versus placebo, Outcome 2 Total Rhodes Index score on day 3.
8.4. Analysis.
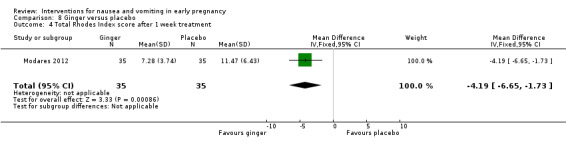
Comparison 8 Ginger versus placebo, Outcome 4 Total Rhodes Index score after 1 week treatment.
8.5. Analysis.
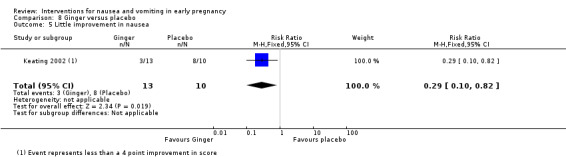
Comparison 8 Ginger versus placebo, Outcome 5 Little improvement in nausea.
8.12. Analysis.
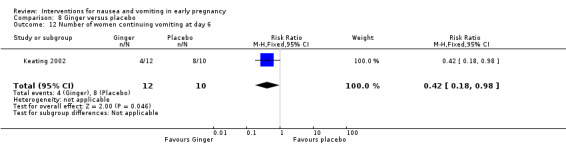
Comparison 8 Ginger versus placebo, Outcome 12 Number of women continuing vomiting at day 6.
In the study by Vutyavanich 2001 (n = 70), results suggested that improvement in nausea symptoms was greater in the ginger group over four days of treatment (MD 1.20, 95% CI 0.22 to 2.18, Analysis 8.6), but when intention‐to‐treat IITT) analysis was carried out (to include three missing patients in the placebo group counted as treatment failures), the evidence of a difference between groups was no longer statistically significant (MD 0.60 95%, CI ‐0.51 to 1.71, Analysis 8.7).
8.6. Analysis.
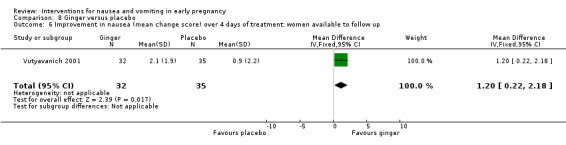
Comparison 8 Ginger versus placebo, Outcome 6 Improvement in nausea (mean change score) over 4 days of treatment: women available to follow up.
8.7. Analysis.
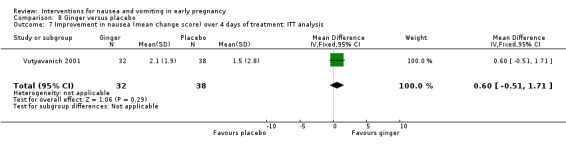
Comparison 8 Ginger versus placebo, Outcome 7 Improvement in nausea (mean change score) over 4 days of treatment: ITT analysis.
Results from Saberi 2014 in a study of 95 women comparing ginger versus no intervention (and P6 acupressure, reported above) found no statistically significant difference on total Rhodes Index score on day three of intervention (MD 0.79, 95% ‐1.89 to 3.47, Analysis 8.3).
8.3. Analysis.
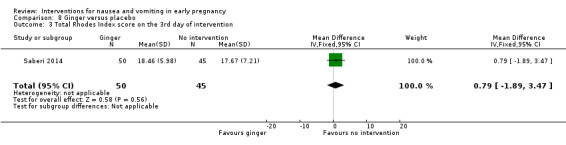
Comparison 8 Ginger versus placebo, Outcome 3 Total Rhodes Index score on the 3rd day of intervention.
Ozgoli 2009 also compared ginger with placebo and presented the results on nausea intensity using the total number of nausea‐intensity assessments per group (assessments were carried out twice daily over four days for each participant, resulting in a total of 280 assessments for treatment group and 256 assessments for control group). Apart from those results, which are not easily interpreted, and have not been included in our analysis, improvements in nausea intensity are reported in percentages per group (from which numbers have been calculated and analysed in this review). Data on overall improvements appear to have been gathered during interview (by an unblinded researcher) on day five, rather than by comparing scores over time, but this is unclear. These results show a statistically significant difference between groups, favouring the treatment group (RR 1.48, 95% CI 1.07 to 2.04, Analysis 8.8) on "nausea intensity improvement". The authors also report a reduction in the incidence of vomiting following treatment of 50% in the intervention group compared with 9% in the control group, although the original data on post‐treatment vomiting are not reported, and are not included in our analyses tables.
8.8. Analysis.
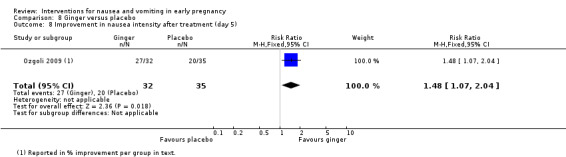
Comparison 8 Ginger versus placebo, Outcome 8 Improvement in nausea intensity after treatment (day 5).
Finally Basirat 2009 compared ginger biscuits with placebo biscuits in a study with 62 women. The authors report a statistically significant difference in baseline symptoms (P = 0.008) and thereafter mostly present results as change from those respective baselines for ginger and placebo groups, with a statistically significant difference in all cases, between the change from baseline to each day; these were not added to data tables due to the effects of the baseline difference; the actual level of symptoms for both groups are similar across each day after baseline. Where they report actual results averaged days one to four, the differences are not statistically different (MD 0.03, CI ‐0.88 to 0.94, Analysis 8.9). The authors also report a general assessment from the participants (much worse to much better) and those results did not find a statistically significant different for ginger over placebo for symptom improvement (RR 1.25, CI 0.96 to 1.63, Analysis 8.10).
8.9. Analysis.
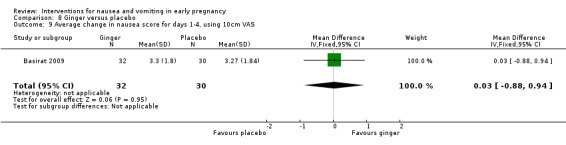
Comparison 8 Ginger versus placebo, Outcome 9 Average change in nausea score for days 1‐4, using 10cm VAS.
8.10. Analysis.
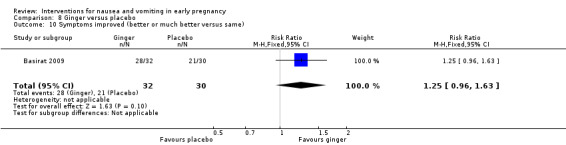
Comparison 8 Ginger versus placebo, Outcome 10 Symptoms improved (better or much better versus same).
Adverse maternal and fetal/neonatal outcomes
Vutyavanich 2001 reported on the rates of spontaneous abortion, with no significant difference between groups (RR 0.36, 95% CI 0.04 to 3.33, Analysis 8.13). Similarly, for delivery by caesarean section, there was no difference between groups (RR 1.64, 95% CI 0.51 to 5.29, Analysis 8.14). The authors reported that there were no congenital abnormalities in either group. As with the other studies reporting such fetal outcomes, this study did not have sufficient power to show differences between groups; we will return to this in the discussion.
8.13. Analysis.
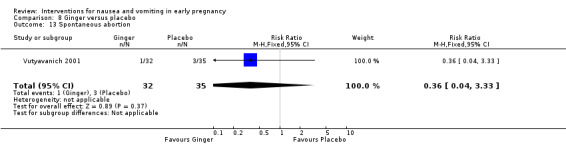
Comparison 8 Ginger versus placebo, Outcome 13 Spontaneous abortion.
8.14. Analysis.
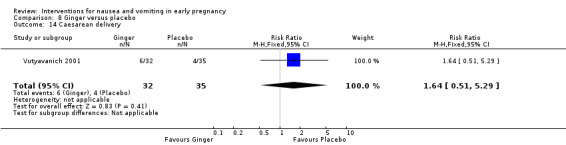
Comparison 8 Ginger versus placebo, Outcome 14 Caesarean delivery.
Willetts 2003 compared fetal adverse outcomes (such as stillbirth, neonatal death, preterm delivery, congenital abnormalities) with expected numbers based on data at one hospital in Sydney. The results were not clearly presented by randomisation group, but were shown for the overall number who completed the main study, with descriptive text about the number in the ginger group. The authors concluded that those exposed to ginger did not appear to be at greater risk of fetal abnormalities.
Also, in a study of ginger versus placebo, Keating 2002 reported weight change measured at the four‐week follow‐up visit, but data were not presented in a usable form; the authors commented that most women in both groups maintained or gained weight.
Modares 2012 (ginger versus chamomile versus placebo) reported one episode of 'severe nausea' and one allergic reaction in the chamomile group and one case of vomiting and another case of severe reaction and hospitalisation (though it is not clear why nausea and vomiting, the symptoms being treated, are reported as side effects).
The other studies of ginger versus placebo do not report maternal or fetal/neonatal outcomes.
Secondary outcomes
Quality of life
No studies of ginger versus placebo report quality of life outcomes.
Economic costs
No studies of ginger versus placebo report economic cost outcomes.
Ginger versus P6 acupressure (one study with 98 women)
One study (Saberi 2014) compared ginger to P6 acupressure.
Primary outcomes
Symptomatic relief
Results from Saberi 2014 comparing ginger to P6 acupressure (and no intervention, reported above) do not favour ginger (MD 2.27, 95% CI ‐0.01 top 4.55, Analysis 9.1) using the total Rhodes Index score on day three.
9.1. Analysis.
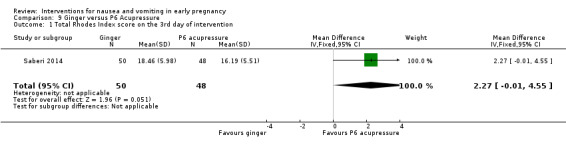
Comparison 9 Ginger versus P6 Acupressure, Outcome 1 Total Rhodes Index score on the 3rd day of intervention.
Adverse maternal and fetal/neonatal outcomes
Adverse outcomes are not reported.
Secondary outcomes
Quality of life
Quality of life outcomes are not reported.
Economic costs
Economic cost outcomes are not reported.
Ginger versus chamomile (one study with 105 women)
Primary outcomes
Symptomatic relief
In one study of ginger versus chamomile (Modares 2012), there was no statistically significant difference between chamomile and ginger (MD 1.55, 95% CI 95%, ‐0.34 to 3.44, data for 70 women, Analysis 10.1), measured using the Rhodes Index after one week of treatment.
10.1. Analysis.
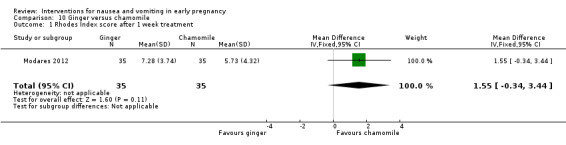
Comparison 10 Ginger versus chamomile, Outcome 1 Rhodes Index score after 1 week treatment.
Adverse maternal and fetal/neonatal outcomes
Secondary outcomes
Quality of life
This study of ginger versus chamomile did not report quality of life outcomes.
Economic costs
This study of ginger versus chamomile did not report economic cost outcomes.
Ginger versus vitamin B6 (four studies with 624 women)
Four trials compared ginger and vitamin B6 (Chittumma 2007; Ensiyeh 2009; Smith 2004; Sripramote 2003).
Primary outcomes
Symptomatic relief
In the two trials comparing ginger to vitamin B6 that had comparable outcomes reported (Chittumma 2007; Sripramote 2003), no statistically significant difference was found between groups (standardised mean difference (SMD) ‐0.00, 95% CI ‐0.25 to 0.25, I² = 0%, data for 251 women, Analysis 11.1) for symptom scores on day three. Chittumma 2007 used the Rhodes Index to measure symptom relief, while in the Sripramote 2003 trial a 10 cm VAS was used to measure level of nausea; results from both studies were not statistically significant. Post‐treatment number of vomiting episodes on day three was similar in the two intervention groups in the Sripramote 2003 trial (MD 0.00, 95% CI ‐0.60 to 0.60, 128 women, Analysis 11.2). Ensiyeh 2009 and Smith 2004 present results on improvement in symptoms and pooled results show no statistically significant difference between groups for the number of women reporting no relief (average RR 0.84, 95% CI 0.47 to 1.52, 360 women (random‐effects), although there was moderate heterogeneity for this outcome and results should be interpreted with caution (heterogeneity: Tau² = 0.11, I² = 52%. P = 0.15; Analysis 11.3).
11.1. Analysis.
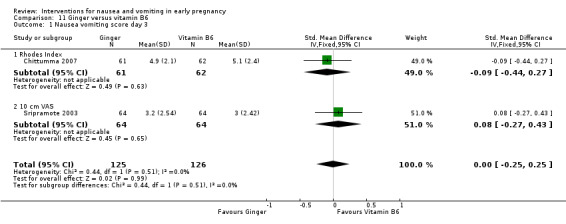
Comparison 11 Ginger versus vitamin B6, Outcome 1 Nausea vomiting score day 3.
11.2. Analysis.
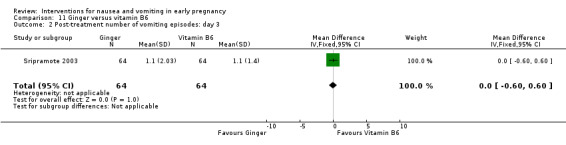
Comparison 11 Ginger versus vitamin B6, Outcome 2 Post‐treatment number of vomiting episodes: day 3.
11.3. Analysis.
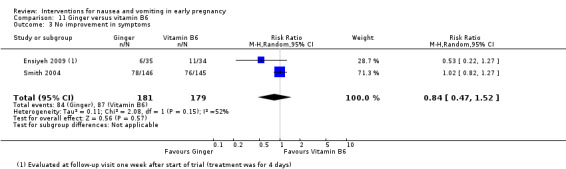
Comparison 11 Ginger versus vitamin B6, Outcome 3 No improvement in symptoms.
Adverse maternal and fetal/neonatal outcomes
Smith 2004 reported on outcomes including spontaneous abortion, stillbirth, heartburn, congenital abnormality, antepartum haemorrhage/abruption or placenta praevia, pregnancy‐induced hypertension, pre‐eclampsia and preterm birth. There were no neonatal deaths in either group and no significant differences between the groups (Analysis 11.4 to Analysis 11.10). Similarly in Ensiyeh 2009, no significant differences were found in the maternal and fetal outcomes reported (spontaneous abortions, caesarean delivery, congenital anomaly of the baby (Analysis 11.4, Analysis 11.6, Analysis 11.15)). The authors report that "all were discharged in good condition", though elsewhere they said that data collection and follow‐up took 12 weeks; women were recruited to the trial at 17 weeks' gestation or less, implying a longer follow‐up time.
11.4. Analysis.
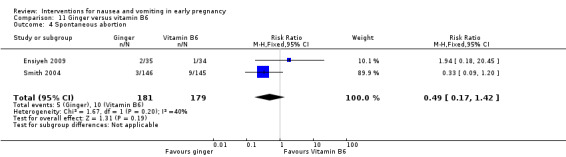
Comparison 11 Ginger versus vitamin B6, Outcome 4 Spontaneous abortion.
11.10. Analysis.
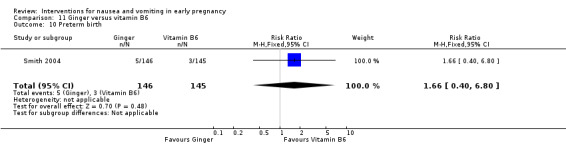
Comparison 11 Ginger versus vitamin B6, Outcome 10 Preterm birth.
11.6. Analysis.
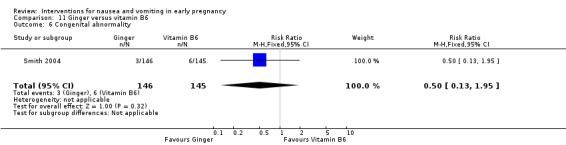
Comparison 11 Ginger versus vitamin B6, Outcome 6 Congenital abnormality.
11.15. Analysis.
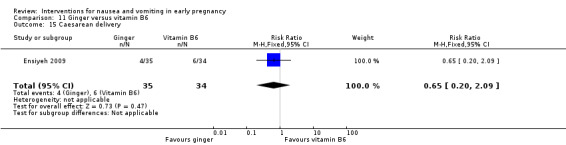
Comparison 11 Ginger versus vitamin B6, Outcome 15 Caesarean delivery.
Chittumma 2007 reported on arrhythmia and headache, with no evidence of a difference in effect between groups (Analysis 11.11; Analysis 11.12). Two studies (Chittumma 2007; Sripramote 2003) report results for heartburn, with no significant effect (RR 2.35, 95% CI 0.93 to 5.93, heterogeneity: I² = 3%, P = 0.31, Analysis 11.13). Chittumma 2007 reported on drowsiness, with neither ginger nor vitamin B6 favoured (RR 0.65, 95% CI 0.27 to 1.56, Analysis 11.14). Sripramote 2003 reported on sedation, with no strong evidence for either intervention (RR 0.81, 95% CI 0.47 to 1.39, Analysis 11.14).
11.11. Analysis.
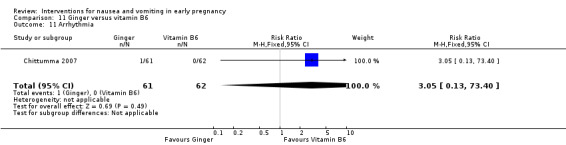
Comparison 11 Ginger versus vitamin B6, Outcome 11 Arrhythmia.
11.12. Analysis.
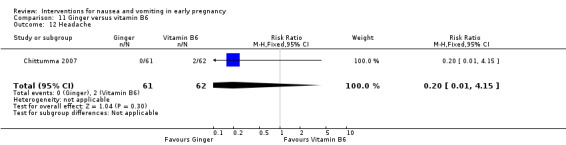
Comparison 11 Ginger versus vitamin B6, Outcome 12 Headache.
11.13. Analysis.
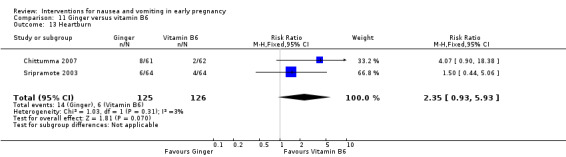
Comparison 11 Ginger versus vitamin B6, Outcome 13 Heartburn.
11.14. Analysis.
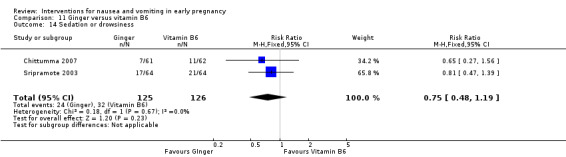
Comparison 11 Ginger versus vitamin B6, Outcome 14 Sedation or drowsiness.
Secondary outcomes
Quality of life
No studies of ginger versus vitamin B6 reported quality of life outcomes.
Economic costs
The studies of ginger versus vitamin B6 did not report economic cost outcomes.
Ginger versus metoclopramide (one study with 68 women)
Primary outcomes
Symptomatic relief
One study compared ginger with metoclopramide and placebo (Mohammadbeigi 2011); there was no significant difference between groups for mean nausea score (MD 1.56, 95% CI ‐0.22 to 3.34, Analysis 12.1), vomiting score (MD 0.33, 95% CI ‐0.69 to 1.35, Analysis 12.2), and overall Rhodes Index score (MD 1.89, 95% CI ‐0.78 to 4.56, Analysis 12.3).
12.1. Analysis.
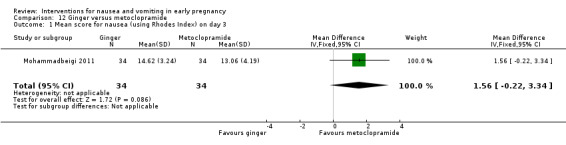
Comparison 12 Ginger versus metoclopramide, Outcome 1 Mean score for nausea (using Rhodes Index) on day 3.
12.2. Analysis.
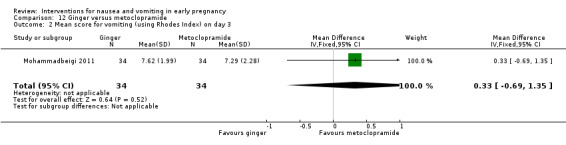
Comparison 12 Ginger versus metoclopramide, Outcome 2 Mean score for vomiting (using Rhodes Index) on day 3.
12.3. Analysis.
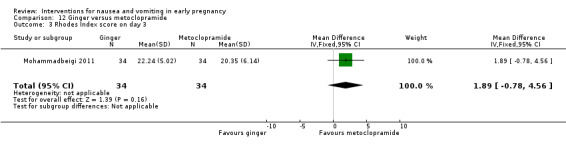
Comparison 12 Ginger versus metoclopramide, Outcome 3 Rhodes Index score on day 3.
Adverse maternal and fetal/neonatal outcomes
Mohammadbeigi 2011 did not report adverse maternal or fetal/neonatal outcomes.
Secondary outcomes
Quality of life
This study of ginger versus metoclopramide did not report quality of life outcomes.
Economic costs
This study of ginger versus metoclopramide did not report economic cost outcomes.
Ginger versus dimenhydrinate (one study with 170 women)
Primary outcomes
Symptomatic relief
One study (Pongrojpaw 2007a) compared ginger and dimenhydrinate, but the results for symptomatic relief were not easily interpreted and therefore, data have not been added to data tables in RevMan 2014.
Adverse maternal and fetal/neonatal outcomes
Pongrojpaw 2007a reported on the side effects of drowsiness and heartburn. More people in the dimenhydrinate group experienced drowsiness, while more in the ginger group experienced heartburn, but evidence of difference between groups was not statistically significant (drowsiness: RR 0.08, 95% CI 0.03 to 0.18, Analysis 13.1; heartburn: RR 1.44, 95% CI 0.65 to 3.20, Analysis 13.2).
13.1. Analysis.
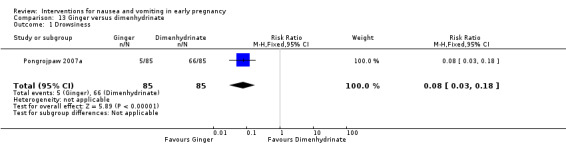
Comparison 13 Ginger versus dimenhydrinate, Outcome 1 Drowsiness.
13.2. Analysis.
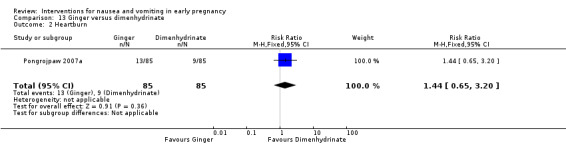
Comparison 13 Ginger versus dimenhydrinate, Outcome 2 Heartburn.
Secondary outcomes
Quality of life
The one study of ginger versus dimenhydrinate did not report quality of life outcomes.
Economic costs
The one study of ginger versus dimenhydrinate did not report economic cost outcomes.
Ginger versus Doxinate (doxylamine succinate plus pyridoxine hydrochloride) (one study with 63 women)
Primary outcomes
Symptomatic relief
Biswas 2011 reported only medians for symptomatic data so data have not been added to tables; the authors reported no statistical differences between groups for nausea and vomiting (with symptoms improving for both groups at the end of week one, end of week two and at a follow‐up visit). The authors (not contactable) concluded that therefore ginger is a safe and effective alternative therapy.
Adverse maternal and fetal/neonatal outcomes
Biswas 2011 reported that one (of 34) in the ginger group and two (of 29) participants in the Doxinate groups reported adverse events; body ache and loose stools for ginger and hyperacidity for the Doxinate participant. No serious adverse events were reported and all participants reported normal pregnancy outcome.
Secondary outcomes
Quality of life
Biswas 2011 reported well‐being at the end of week one of the study of ginger versus doxylamine, with dichotomous responses (yes/no) but the question asked was not included in the report, so the meaning of the responses was unclear, therefore, data have not been added to this review's tables. The authors (not contactable) reported that no inter‐group differences were found.
Economic costs
Biswas 2011 did not report economic cost outcomes.
Lemon oil versus placebo (one study with 100 women)
Primary outcomes
Symptomatic relief
One study (Yavari 2014) found that while there was not a statistically significant difference on levels of symptoms on day three (using the PUQE‐24 instrument) (MD ‐0.46, 95% CI ‐1.27 to 0.35, Analysis 14.1), the group using lemon oil did show a difference in reduction of symptoms from baseline to day three (MD ‐1.50, 95% CI ‐2.41 to ‐0.59, Analysis 14.2). There was no significant difference in the number of women satisfied with treatment in this study (RR 1.47, 95% CI 0.91 to 2.37, Analysis 14.3).
14.1. Analysis.
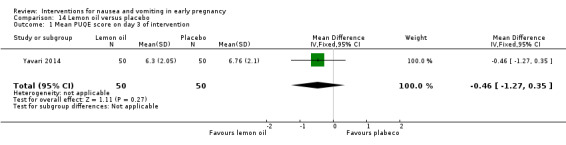
Comparison 14 Lemon oil versus placebo, Outcome 1 Mean PUQE score on day 3 of intervention.
14.2. Analysis.
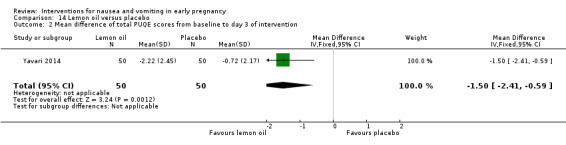
Comparison 14 Lemon oil versus placebo, Outcome 2 Mean difference of total PUQE scores from baseline to day 3 of intervention.
14.3. Analysis.
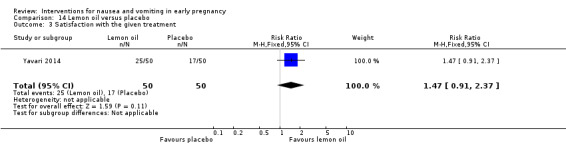
Comparison 14 Lemon oil versus placebo, Outcome 3 Satisfaction with the given treatment.
Adverse maternal and fetal/neonatal outcomes
Yavari 2014 reports no adverse effects due to treatment for ether group.
Secondary outcomes
Quality of life
No quality of life outcomes were reported.
Economic costs
No economic cost outcomes were reported.
Mint oil versus placebo (one study with 60 women)
Primary outcomes
Symptomatic relief
Pasha 2012 compared mint oil with placebo and there were no statistically significant differences between groups for nausea level (MD ‐0.88, 95% CI ‐1.93 to 0.17, Analysis 15.1) or vomiting level (MD ‐0.32, 95% CI ‐1.45 to 0.81, Analysis 15.2), on day four.
15.1. Analysis.
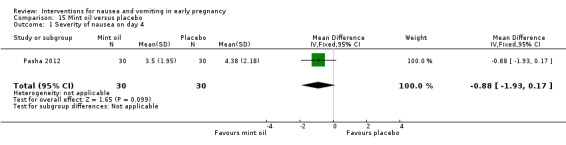
Comparison 15 Mint oil versus placebo, Outcome 1 Severity of nausea on day 4.
15.2. Analysis.
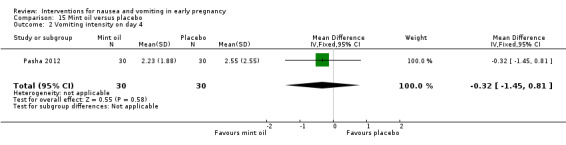
Comparison 15 Mint oil versus placebo, Outcome 2 Vomiting intensity on day 4.
Adverse maternal and fetal/neonatal outcomes
Pasha 2012 did not report adverse maternal or fetal/neonatal outcomes.
Secondary outcomes
Quality of life
This one study of mint oil versus placebo did not report quality of life outcomes.
Economic costs
This study of mint oil versus placebo did not report economic cost outcomes.
Chamomile versus placebo (one study with 70 women)
Primary outcomes
Symptomatic relief
In one study comparing chamomile versus placebo (Modares 2012), chamomile was favoured (MD ‐5.74, 95% CI ‐8.31 to ‐3.17, Analysis 16.1) for level of symptoms (using Rhodes Index) measured one week after treatment started.
16.1. Analysis.
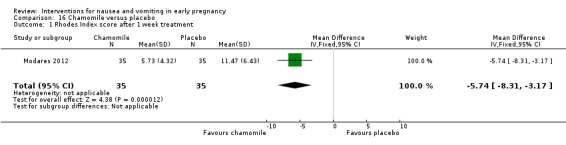
Comparison 16 Chamomile versus placebo, Outcome 1 Rhodes Index score after 1 week treatment.
Adverse maternal and fetal/neonatal outcomes
Modares 2012 did not report adverse maternal or fetal/neonatal outcomes.
Secondary outcomes
Quality of life
No quality of life outcomes were reported.
Economic costs
No economic outcomes were reported.
Vitamin B6 versus placebo (two studies with 416 women)
Primary outcomes
Symptomatic relief
In two studies comparing vitamin B6 with placebo (Sahakian 1991; Vutyavanich 1995), results favoured vitamin B6 for reduction in nausea after three days (MD 0.92, 95% CI 0.40 to 1.44, Analysis 17.1). Comparing the number of patients vomiting post‐treatment, there was no strong evidence that vitamin B6 reduced vomiting (average RR 0.76, 95% CI 0.35 to 1.66, Analysis 17.2). As there was high heterogeneity for this outcome we used a random‐effects model and results should be interpreted with caution (heterogeneity: I² = 77%, Tau² = 0.25, P = 0.04).
17.1. Analysis.
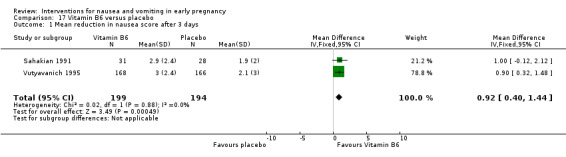
Comparison 17 Vitamin B6 versus placebo, Outcome 1 Mean reduction in nausea score after 3 days.
17.2. Analysis.
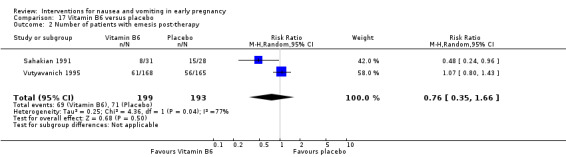
Comparison 17 Vitamin B6 versus placebo, Outcome 2 Number of patients with emesis post‐therapy.
Adverse maternal and fetal/neonatal outcomes
Neither study studies reported adverse maternal and fetal/neonatal outcomes.
Secondary outcomes
Quality of life
Neither study reported quality of life outcomes.
Economic costs
Neither study reported economic costs outcomes.
Vitamin B6 versus dimenhydrinate (one study with 135 women)
Primary outcomes
Symptomatic relief
In one study Babaei 2014 compared vitamin B6 with dimenhydrinate and results favour dimenhydrinate after three days of treatment measured using Rhiodes Index (MD 1.20, 95% CI 0.47 to 1.93, Analysis 19.1).
19.1. Analysis.

Comparison 19 Vitamin B6 versus dimenhydrinate, Outcome 1 Nausea and vomiting score after 3 days of treatment using Rhodes Index.
Adverse maternal and fetal/neonatal outcomes
Babaei 2014 reported a significant difference in drowsiness favouring vitamin B6 over dimenhydrinate (RR 0.14, 95% CI 0.06 to 0.34, Analysis 19.2).
19.2. Analysis.
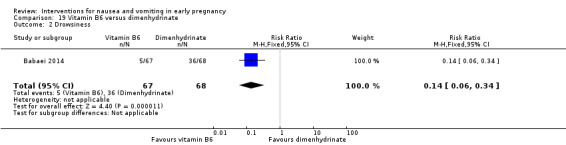
Comparison 19 Vitamin B6 versus dimenhydrinate, Outcome 2 Drowsiness.
Secondary outcomes
Quality of life
Quality of life outcomes were not reported.
Economic costs
Economic cost outcomes were not reported.
High‐dose vitamin B6 versus low‐dose vitamin B6 (one study with 60 women)
Primary outcomes
Symptomatic relief
Wibowo 2012 reported a significant difference favouring high‐dose over low‐dose vitamin B6 (MD ‐1.06, 95% CI ‐2.05 to ‐0.07, Analysis 18.1) for reduction in symptoms using PUQE, measured from baseline to two weeks.
18.1. Analysis.
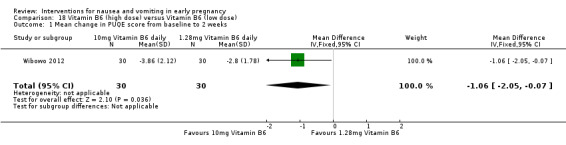
Comparison 18 Vitamin B6 (high dose) versus Vitamin B6 (low dose), Outcome 1 Mean change in PUQE score from baseline to 2 weeks.
Adverse maternal and fetal/neonatal outcomes
Adverse maternal or fetal/neonatal outcomes were not reported.
Secondary outcomes
Quality of life
Quality of life outcomes were not reported.
Economic costs
Economic cost outcomes were not reported.
Anti‐emetic medication versus placebo (10 studies with 1249 women)
There were 10 studies of anti‐emetic medications. A range of anti‐emetics (hydroxyzine, Debendox, Bendectin, Diclectin, thiethylperazine and fluphenazine‐pyridoxine) were compared with placebos; in one study, three anti‐emetic medications were compared, and in two studies ondansetron was compared with another medication.
Primary outcomes
Symptomatic relief
One study (Erez 1971) compared hydroxyzine with placebo, with the results favouring hydroxyzine for relief of nausea (RR 0.23, 95% CI 0.15 to 0.36, 150 women, Analysis 20.1).
20.1. Analysis.
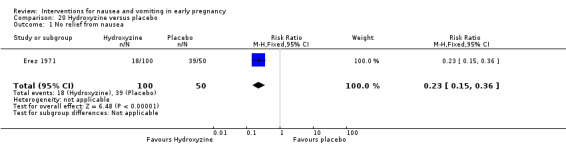
Comparison 20 Hydroxyzine versus placebo, Outcome 1 No relief from nausea.
Two studies (Geiger 1959; McGuiness 1971) compared preparations of doxylamine succinate 10 mg, pyridoxine 10 mg and dicyclomine 10 mg (as Bendectin (US) and Debendox (UK) respectively) with placebo, and results for nausea relief favoured the intervention group. However, there was high heterogeneity when results from these two studies were combined and the time point at which outcome data were collected was not clear in the McGuiness 1971 study, and so in the analyses we have provided subtotals only. In the McGuiness 1971 study, while fewer women in the Debendox group had no relief in symptoms, the difference between groups was not statistically significant (RR 0.65, 95% CI 0.36 to 1.17, 81 women, Analysis 21.1). In the Geiger 1959 study, only three of 52 women receiving Debendox reported no improvement in symptoms compared with 20/57 for controls.
21.1. Analysis.
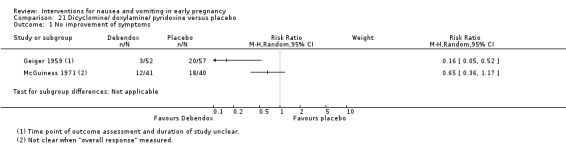
Comparison 21 Dicyclomine/ doxylamine/ pyridoxine versus placebo, Outcome 1 No improvement of symptoms.
More recently Koren 2010 compared Diclectin (doxylamine succinate 10 mg and pyridoxine hydrochloride 10 mg) and placebo. Results favoured Diclectin for improvement in symptoms (MD ‐0.90, 95% CI ‐1.55 to ‐0.25, 256 women, Analysis 22.1) from baseline to day 15 and for global‐assessment of well‐being (MD 1.00, 95% CI 0.38 to 1.62, Analysis 22.5), again from baseline to day 15. The authors measured the 'average change in symptoms' (measured as 'mean area under the curve for change in PUQE from baseline' as measured day‐by‐day) and reported a statistically significant difference favouring Dilectin (P < 0.0001) (data not shown in data and analysis tables). Requests for compassionate use of the drug after day 14 favoured Diclectin (RR 1.49, 95% CI 1.10 to 2.02, Analysis 22.2), a proxy measure for perception of effectiveness.
22.1. Analysis.
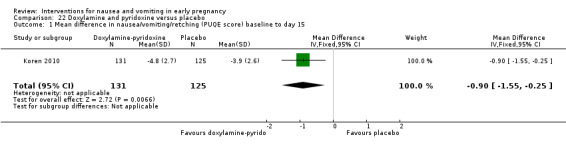
Comparison 22 Doxylamine and pyridoxine versus placebo, Outcome 1 Mean difference in nausea/vomiting/retching (PUQE score) baseline to day 15.
22.5. Analysis.
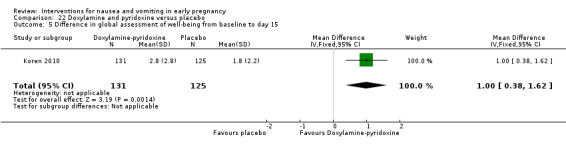
Comparison 22 Doxylamine and pyridoxine versus placebo, Outcome 5 Difference in global assessment of well‐being from baseline to day 15.
22.2. Analysis.
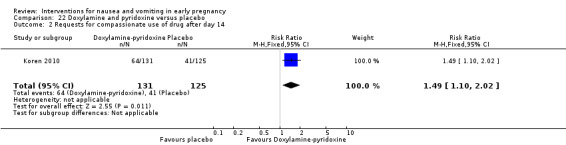
Comparison 22 Doxylamine and pyridoxine versus placebo, Outcome 2 Requests for compassionate use of drug after day 14.
Thiethylperazine was compared with placebo in one study (Newlinds 1964) and women in the placebo group were less likely to experience symptom relief (RR 0.49, 95% CI 0.31 to 0.78, 164 women, Analysis 23.1). Finally, fluphenazine‐pyridoxine seemed to improve symptoms compared with placebo in one trial, but results did not reach statistical significance (RR 0.52, 95% CI 0.27 to 1.01, 78 women, Analysis 24.1) (Price 1964); this is an antipsychotic drug (from the piperazine class of phenothiazines).
23.1. Analysis.
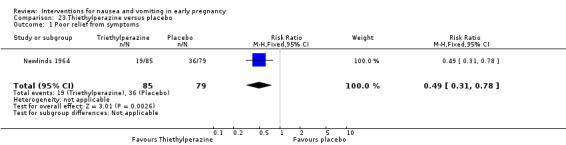
Comparison 23 Thiethylperazine versus placebo, Outcome 1 Poor relief from symptoms.
24.1. Analysis.
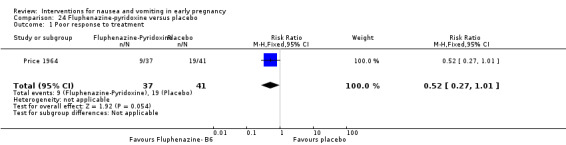
Comparison 24 Fluphenazine‐pyridoxine versus placebo, Outcome 1 Poor response to treatment.
Metoclopramide was compared with placebo in one study (Mohammadbeigi 2011) and results favoured metoclopramide for nausea level (MD ‐2.94, 95% CI ‐4.55 to ‐1.33, 68 women, Analysis 25.1) and vomiting (MD ‐1.47, 95% CI, ‐2.33 to ‐0.61, Analysis 25.2), on day three.
25.1. Analysis.
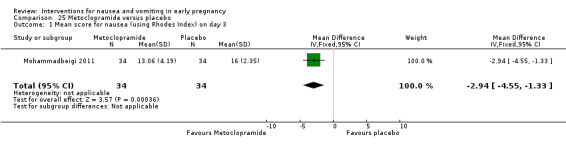
Comparison 25 Metoclopramide versus placebo, Outcome 1 Mean score for nausea (using Rhodes Index) on day 3.
25.2. Analysis.
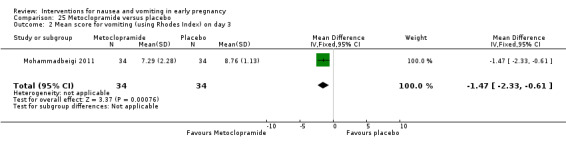
Comparison 25 Metoclopramide versus placebo, Outcome 2 Mean score for vomiting (using Rhodes Index) on day 3.
Bsat 2003a compared three drug regimens: pyridoxine‐metoclopramide, prochlorperazine and promethazine. Results were reported in graphs and we have not entered estimated figures into data tables. Approximately 65%, 38% and 40% of women in each group, respectively, responded that they felt better on the third day of treatment. The authors concluded that their results favoured pyridoxine‐metoclopramide over the other two regimens.
Ondansetron was compared with metoclopramide in one study with data for 70 women (Ghahiri 2011), and no statistical difference was found for nausea (MD ‐0.12, 95% CI ‐0.44 to 0.20, Analysis 26.1) and vomiting (MD ‐0.20, 95% CI ‐0.57 to 0.17, Analysis 26.2) on day three, with symptoms improving for both groups.
26.1. Analysis.
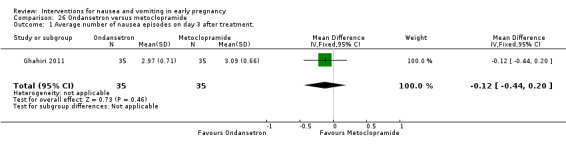
Comparison 26 Ondansetron versus metoclopramide, Outcome 1 Average number of nausea episodes on day 3 after treatment..
26.2. Analysis.
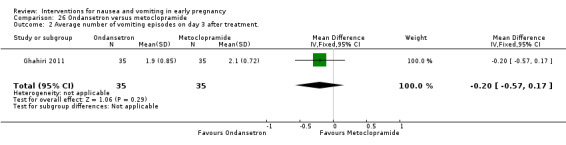
Comparison 26 Ondansetron versus metoclopramide, Outcome 2 Average number of vomiting episodes on day 3 after treatment..
Ondansetron was compared with pyridoxine‐doxylamine (Bendectin) in one study of 30 women (Oliveira 2014) but results are presented with medians only and were not entered in data tables. The authors report statistically significant results favouring ondansetron for nausea and vomiting relief and conclude that their investigation showed ondansetron to be superior to the combination of pyridoxine and doxylamine in the treatment of nausea in pregnancy. Dichotomous data on 'clinical improvement'/not using a 25 mm improvement on 100 mm VAS (as improvement) are seen to favour ondansetron (RR 2.24, 955 CI 1.24 to 4.04, Analysis 27.1). However, Cunningham 2015 and Koren 2015 challenge the sample size in this study, dose and type (not slow release) of doxylamine‐pyridoxine, and measurement instrument and urge caution in the conclusions drawn by Oliveira 2014.
27.1. Analysis.
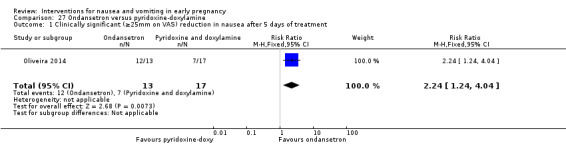
Comparison 27 Ondansetron versus pyridoxine‐doxylamine, Outcome 1 Clinically significant (≥25mm on VAS) reduction in nausea after 5 days of treatment.
Adverse maternal and fetal/neonatal outcomes
In the trials of anti‐emetic drugs, fetal outcome was recorded only by Erez 1971. In that study, of the 79 cases available for follow‐up in the hydroxyzine group, there were four spontaneous abortions (three in the first trimester and one in the second trimester), and one perinatal death. In the 36 cases available for follow‐up from the placebo group, there were two first trimester spontaneous abortions (spontaneous abortions: RR 0.91, 95% CI 0.17 to 4.75, Analysis 20.2; perinatal mortality: RR 1.39, 95% CI 0.06 to 33.26, Analysis 20.3). In the text, the authors report that slight drowsiness was reported by 7% (n = 7) of the treatment group, but no other adverse effects were reported, and there were no hospitalisations in either group.
20.2. Analysis.
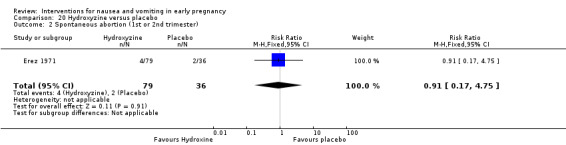
Comparison 20 Hydroxyzine versus placebo, Outcome 2 Spontaneous abortion (1st or 2nd trimester).
20.3. Analysis.
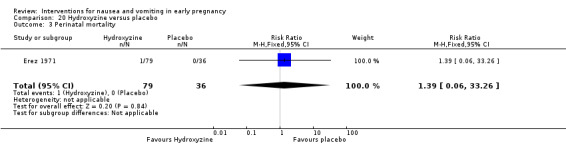
Comparison 20 Hydroxyzine versus placebo, Outcome 3 Perinatal mortality.
Bsat 2003a reported a non‐significant difference in hospitalisation across the three groups receiving pyridoxine‐metoclopramide, prochlorperazine and promethazine. They commented that subsequent pregnancy courses were similar and only one neonatal anomaly was seen (a cardiac defect in the prochlorperazine group).
McGuiness 1971 stated that side effects were reported by 12 patients in the Debendox group (including drowsiness for three patients, feeling weak for two, tiredness for two) compared to six adverse effects reported in the placebo group (including tiredness, sleepiness, depression and constipation). Newlinds 1964 reported that side effects occurred in 12 of the 93 patients who received thiethylperazine and 10 of the 87 in the placebo group. These adverse effects included drowsiness (four treatment, three placebo), aggravation of nausea (two treatment, three placebo), 'cerebral stimulation', described as mild in the text, and included restlessness (two in treatment group, none in placebo). Price 1964 reported that there were no side effects in the fluphenazine‐pyridoxine group and one patient in the placebo group reported drowsiness. Geiger 1959 reported that one patient in the Bendectin group reported listlessness; no other adverse effects were reported.
Koren 2010 reports no significant differences between groups receiving Diclectin versus placebo for maternal side effects including headache (RR 0.81, 95% CI 0.45 to 1.48, Analysis 22.3) and somnolence (RR 1.21, 95% CI 0.64 to 2.27, Analysis 22.4); other side effects were reported by a similar and small number of participants per group and have not been added to the data tables.
22.3. Analysis.
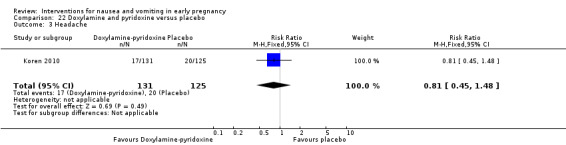
Comparison 22 Doxylamine and pyridoxine versus placebo, Outcome 3 Headache.
22.4. Analysis.
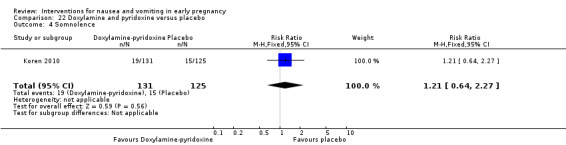
Comparison 22 Doxylamine and pyridoxine versus placebo, Outcome 4 Somnolence.
There are no significant differences in the study by Oliveira 2014 of ondansetron with pyridoxine‐doxylamine for sedation (RR 0.75, 95% CI 0.28 to 2.02, Analysis 27.2) or constipation (RR 2.18, 95% CI 0.63 to 7.5, Analysis 27.3); as discussed above, sample size and treatment protocol have been questioned (Cunningham 2015; Koren 2015).
27.2. Analysis.
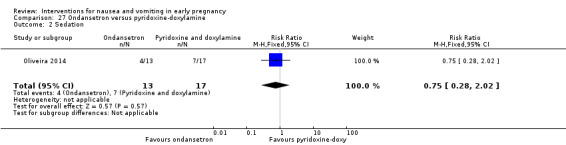
Comparison 27 Ondansetron versus pyridoxine‐doxylamine, Outcome 2 Sedation.
27.3. Analysis.
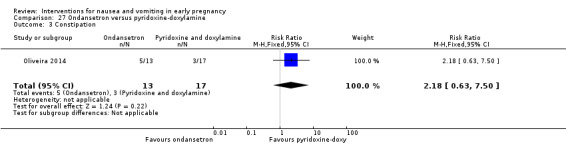
Comparison 27 Ondansetron versus pyridoxine‐doxylamine, Outcome 3 Constipation.
Secondary outcomes
Quality of life
Koren 2010 compared Diclectin (doxylamine succinate 10 mg and pyridoxine hydrochloride 10 mg) and placebo and results favoured Diclectin for global‐assessment of well‐being measured within PUQE (MD 1.00, 95% CI 0.38 to 1.62, Analysis 22.5), again from baseline to day 15.
Economic costs
Koren 2010 in a study comparing Diclectin with placebo reported loss of employment in days; there was no statistically significant difference between groups (MD ‐1.45, 95% CI ‐3.36 to 0.46, Analysis 22.6). It should be noted that mean days employment loss were 0.92 days (SD 3.86) for Diclectin and 2.37 (SD10.23) for placebo (P = 0.06).
22.6. Analysis.
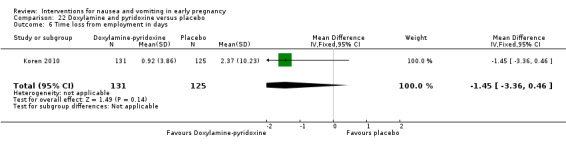
Comparison 22 Doxylamine and pyridoxine versus placebo, Outcome 6 Time loss from employment in days.
Discussion
Summary of main results
Nausea and vomiting in early pregnancy are common. Symptoms are generally self‐limiting, are not usually life threatening and, provided women do not have very severe vomiting, do not often lead to serious complications. Nevertheless, early pregnancy nausea and vomiting may be extremely distressing to women, and may disrupt their physical and social functioning, and affect their quality of life.
In this review we found little strong or consistent evidence that non‐pharmacological therapies are effective in reducing symptoms. There was some evidence regarding the effectiveness of P6 acupressure. There was also some evidence of the effectiveness of auricular acupressure, though further larger studies are required to confirm this. Acupuncture (P6 or traditional) showed no significant benefit to women with nausea and vomiting in early pregnancy. The use of preparations containing ginger may be helpful to women, with some evidence of benefit especially from recent studies, but the evidence overall was not consistent.
Nor did we find consistent or strong evidence from trials to support the use of any one pharmacological agent including vitamin B6, antihistamines, and other anti‐emetic drugs to relieve mild or moderate nausea and vomiting (a related Cochrane review is examining their use in women with more severe symptoms (Boelig 2013)). There were only single studies of many anti‐emetics included. There were no studies of dietary or other lifestyle interventions included, though one excluded quasi‐experimental study (Liu 2014) describes an intervention involving a diet and lifestyle resource booklet and individualised follow‐up telephone support, which warrants further study. It is acknowledged that including only randomised controlled trials (RCTs) (which are approached by researchers with caution in the first trimester) is restrictive (Koren 2011), but that is only type of study included in this review.
Overall completeness and applicability of evidence
We attempted to be as inclusive as possible in the search strategy and have included studies reported in languages other than English where translations could be obtained. While the literature included in the review was predominantly reported in European and North American journals, some recent studies from Iran were translated for this review.
Interpreting the findings of the studies included in the review was not simple. Some of the studies were more than 50 years old and during the time period covered by this research, the attitudes of women and clinical staff towards symptoms and towards symptom relief may have changed. Most of the studies examining non‐pharmacological approaches have been published more recently, yet there is very little conclusive evidence on the efficacy of these complementary or alternative therapies.
The main focus of the review was on the effectiveness of interventions to relieve symptoms. However, our prespecified outcomes also included the impact of interventions on the well‐being of mothers and babies. Although there may be a perception that complementary and alternative approaches are not 'invasive', their safety has not been adequately evaluated. Few studies reported pregnancy outcomes, adverse effects from treatments, or adverse events. It may not be safe to assume that because negative outcomes were not reported that they did not occur. In those studies (mainly those focusing on pharmacological interventions) that did report data on side effects and adverse events, none had the statistical power to provide convincing evidence regarding relatively rare adverse outcomes. Non‐randomised research studies (such as the multi‐site population‐based case‐control study of Anderka 2012) or other data sources can provide observational data on adverse effects, from larger samples. UKTIS 2012 specifically reports teratogenic effects of nausea and vomiting interventions in early pregnancy.
Apart from one recent study (Koren 2010), the studies reviewed contained very little information on the psychological, social or economic impact of nausea on pregnant women, despite its burden on women's lives. The scales used tended to focus on the experience of symptoms, but very little data were presented on other aspects of quality of life such as the impact of nausea on family and social functioning, or on relationships (as acknowledged by Wood 2013). Many women experience symptoms whilst attempting to care for young children or whilst attending work; none of the studies reported on outcomes relating to the impact of interventions on family life, the ability to perform work, on paid sickness absence from work, or on the broader economic impact of symptoms.
Some of the interventions examined in the review, such as ginger or acupressure wrist bands, may be transferable to clinical contexts other than those in which they were tested as they may be relatively low cost (although studies did not provide information on this) and acceptable to women and staff. Other interventions may require special equipment not generally available in antenatal care settings (e.g. acustimulation or acupuncture) and staff may need particular skills and training; even if these interventions had been proven effective, they may not be easily transferable between care settings.
Quality of the evidence
We were unable to pool findings from studies for most review outcomes due to heterogeneity in study participants (e.g. stage of pregnancy and severity of symptoms), interventions (and co‐interventions), comparison groups, and outcomes measured or reported (in particular reporting outcomes at widely varying time points). For this reason, most of the results were derived from single studies with findings that have not been replicated elsewhere. Where results from more than one study were pooled, inconsistencies in findings between studies was reflected in high levels of statistical heterogeneity for some outcomes; we have indicated in the results section those outcomes affected by high heterogeneity and advise caution in interpreting those results.
The methodological quality of the included studies was mixed. Many of the included studies were described as being double‐blind, though blinding can be difficult due to the interventions involved. Sham acupressure, acupuncture or acustimulation may not be convincing to women. Some of the trials which investigated the effectiveness of blinding provided some evidence that women may have had some idea of group allocation (Norheim 2001; Smith 2002; Smith 2004). The lack of blinding or unconvincing blinding may be particularly relevant where the main outcome is women's subjective, self‐reported symptoms. We had intended to carry out sensitivity analysis whereby we would exclude from the analyses those studies at high risk of bias to see what impact this would have on findings; however, we did not do this because we were unable to pool data for most interventions and outcomes, and results were derived from single trials.
Lack of clear information on how studies were conducted (especially relating to random sequence generation and allocation concealment) and in selective reporting of results means that some findings are difficult to interpret. Few of the studies provided clear information on whether or not women were using other over‐the‐counter remedies or prescribed medications to control symptoms. This information would have been very helpful in understanding results. One study reported the use of "rescue" medication (Jamigorn 2007). In other studies the treatment effect may have been underestimated if women in control groups were more likely than those in intervention groups to use other treatments.
The effectiveness of vitamin B6 was difficult to interpret. In some studies, vitamin B6 was the active intervention, in others it was the control condition, and in at least two studies it was taken by women in addition to one of the interventions (Bsat 2003a; Rad 2012). In Bsat 2003a it was not clear whether the results obtained for the anti‐emetic plus B6 group were attributable to the anti‐emetic alone, vitamin B6 alone or both acting together, and in Rad 2012 it was reported that women in both Youmen acupressure and placebo groups were taking vitamin B6.
The way in which outcomes were measured and reported in studies varied considerably. Some studies used the validated instruments. Other studies used ordinal data such as three‐ or five‐point scales. In these cases, in order to include data in the analysis tables, we converted the data into binary form by choosing cut‐off points. We attempted to be consistent in choice of cut‐off, opting for no relief versus improvement in symptoms, but we acknowledge that the choice may have impacted the results. There was also variation in the way continuous data were collected, with some studies using visual analogue scales or validated scales. Thirteen studies in the review used the Rhodes Index. This was originally created to measure the nausea and vomiting symptoms of chemotherapy (Rhodes 1984), and has been validated for use in studying these symptoms in pregnancy (Zhou 2001). However, the use of Rhodes Index of Nausea, Vomiting and Retching, for example, was not consistent in studies; some trials used shortened forms or did not collect or report data on all subscales. Further, as we mentioned earlier, in some trials data were collected repeatedly and a great deal of (not always consistent) data were presented. In this review we have tried to present findings for a time point approximately three days after the start of treatment, but this was not always possible. The lack of consistency in the way outcome data were measured and reported should be kept in mind when interpreting results.
The use of pregnancy‐specific nausea and vomiting measurement instruments in recent studies facilitates better outcome measurement. The Pregnancy Unique Quantification of Emesis (and nausea) (PUQE) has been has been developed by clinician‐researchers at the Canadian Motherisk Program. The clinician‐researchers had been using the Rhodes Index and stated that they found it to be detailed but cumbersome and time‐consuming (Koren 2002b). They also noted the strong correlations between the severity of a physical symptom and the stress caused by that symptom. Also, nausea was measured twice (duration and number of bouts (frequency) of nausea). They also felt that, based on their experience, frequency of nausea was more difficult for women to define. The PUQE has been validated against four independent criteria (Koren 2005) and with an established Quality of LIfe instrument (Lacasse 2008), and it has been used in studies that have now been included in this review (Koren 2010; Wibowo 2012; Yavari 2014). Other pregnancy‐specific instruments have been developed (Magee 2002b; Swallow 2002), but these have not been used in published randomised controlled trials identified within this review.
Potential biases in the review process
We acknowledge that there was the potential for bias at all stages in the reviewing process. We attempted to minimise bias in a number of ways; for example, two review authors independently carried out data extraction and assessed risk of bias. However, we acknowledge that such assessments involve subjective judgments, and another review team may not have agreed with all of our decisions. A further possible source of bias (discussed above) was the choice of time points for symptom assessment and the cut‐off points chosen to convert ordinal into binary data for entry into RevMan 2014. Again, we attempted to minimise bias by discussing such issues and attempting to be consistent across studies and outcomes.
Agreements and disagreements with other studies or reviews
Current clinical practice guidelines suggest that acupressure and ginger may be useful in the relief of symptoms of nausea and vomiting (NICE 2008) and NICE 2013 recommend several anti‐emetic drugs (promethazine, cyclizine, prochlorperazine, metoclopramide and ondansetron), based on expert opinion. We found insufficient evidence about these drugs in this review. The American American College of Obstetricians and Gynecologists (ACOG) in its 2004 guideline (affirmed in 2009) concluded that vitamin B6 or doxylamine with vitamin B6 is safe and effective and should be considered first line pharmacotherapy (ACOG 2004). They also stated that, based on weaker evidence, ginger has shown beneficial effects and can be considered as a nonpharmacologic option. The Society of Obstetricians and Gynaecologists of Canada also recommends doxylamine‐pyridoxine as the 'standard of care' for pharmaceutical therapy, since it has 'the greatest evidence to support its efficacy and safety' (Arsenault 2002). Persaud 2014 recently questioned whether evidence is stronger for pyridoxine alone (over doxylamine‐pyridoxine), though Slaughter 2014 explains the FDA approval linked with safety evidence.There is limited evidence of its effectiveness found in this review, due to the small number of studies of this drug that were included.
There are many other non‐Cochrane reviews and overviews of various interventions for nausea and vomiting in pregnancy in the literature (Aikins Murphy 1998; Borrelli 2005; Bryer 2005; Dante 2013; Davis 2004; Ding 2013; King 2009; Kousen 1993; Magee 2002a; Magee 2006; McParlin 2008; Niebyl 2002; Quinlan 2003; Viljoen 2014; Wilkinson 2000). These reviews present variable levels of evidence to back up their conclusions. Bryer 2005 reviews the same three studies of ginger included in this review (Keating 2002; Smith 2004; Vutyavanich 2001), and comments on the variety of doses and preparations used and the lack of safety reporting. Nonetheless, drawing on an observational study of teratogeny, Bryer 2005 concludes that 'ginger is a safe and effective treatment option for nausea and comparable with vitamin B6 in effectiveness'. Our review found limited and inconsistent evidence of such effectiveness. Davis 2004 proposes "an evidence based review" and describes briefly the findings of some trials of both pharmaceutical and non‐pharmaceutical treatments, but does not comment on the quality of studies and concludes that treatment has been 'poorly refined'. Viljoen 2014 reviews the studies of ginger included in this review and also assesses risk of bias; the authors conclude that ginger is a harmless and possibly effective intervention but similar to this review comment on the limited number of studies, varied outcome measurement and varied quality. Magee 2002a offers an 'evidence‐based approach of safety and effectiveness' of pharmacological therapies, and reproduces a forest plot of various treatments from a previous review (Mazzotta 2000). The authors conclude that evidence from controlled trials has shown that Bendectin/Diclectin, antihistamine blockers and phenothiazines as a group are safe and effective for treatment. The current review would not support that conclusion, based on the quality and consistency of evidence. The recent re‐analysis (Chin 2014) of safety data supporting the use of doxylamine for nausea and vomiting in pregnancy suggests that the safety evidence is not as strong as was claimed by Seto 1997. Magee 2006 also comments on the mixed quality of the trials reviewed and the lack of consistent outcome measurement, as was also found in the current review.
Some reviews include cross‐over studies within their inclusion criteria, which is problematic as symptoms generally improve over time during pregnancy. For example, Ernst 2000 includes one trial that studied ginger for nausea and vomiting across different groups (postoperative sickness, seasickness, etc.). The included trial was a cross‐over study with 30 patients; nonetheless, these study results are pooled with two other studies and found to collectively favour ginger over placebo.
Authors' conclusions
Implications for practice.
Women will continue to seek treatments for the often distressing symptoms of nausea and vomiting in pregnancy. They may take over‐the‐counter and complementary therapies, based on anecdotal or peer advice. There are many sources of advice for women on the Internet, including peer fora. Wilkinson 2000 found a lack of consensus about safety of herbal treatments (including ginger) for nausea and vomiting in pregnancy in 300 non‐medical sources identified in a literature review. This highlights the necessity of health professionals providing clear guidance to women, based on systematically reviewed evidence. As a useful example of this, Tiran 2012 offers specific advice on the use of ginger for professionals and women in pregnancy. On the basis of this review, high‐quality consistent evidence is lacking to support the accuracy or appropriateness of that advice. Current guidelines and other reviews often offer incomplete evidence, without comment on the quality of evidence. Health professionals' decisions about treatments should take account of the lack of clear and consistent evidence found in this review and acknowledge that it is not possible at present to identify, with confidence, safe and effective interventions for nausea and vomiting in early pregnancy.
Implications for research.
The difficulties in interpreting the results of the studies included in this review highlight the need for specific and clearly justified outcomes in research on interventions for nausea and vomiting in pregnancy. The range of instruments used to measure these symptoms (including those not developed for this patient group) also suggest the need for a consistent and appropriate approach to measurement, which may be addressed by the PUQE scale, which has been used in recent studies. There is also a need to systematically measure quality of life and adverse maternal and fetal and neonatal outcomes, to ensure that studies are as useful as possible for women seeking safe and effective treatments and health professionals advising them. We did not identify any studies of dietary or behavioural interventions. Dietary and behavioural strategies (eating low‐fat, small, frequent meals) were often recommended to all participants (in both treatment and placebo groups) within the studies in this review. Only one study (Ozgoli 2009) measured adherence to dietary advice. The effectiveness of dietary and other behavioural strategies also needs to be evaluated in good quality trials, for example testing the professional telephone support intervention described in Liu 2014.
What's new
| Date | Event | Description |
|---|---|---|
| 19 January 2015 | New citation required but conclusions have not changed | Four new studies included. |
| 19 January 2015 | New search has been performed | Search updated and 21 new reports identified. |
History
Protocol first published: Issue 1, 2009 Review first published: Issue 9, 2010
| Date | Event | Description |
|---|---|---|
| 21 November 2013 | New citation required but conclusions have not changed | Ten new studies included; conclusions largely unchanged. |
| 27 April 2013 | New search has been performed | Search updated. Methods updated. |
Acknowledgements
Thanks to Susan Wieland for searches of the Cochrane Complementary Medicine Field's Trials Register.
Thanks also to Angela Cooke, Chow Yuan Way, Farhad Shokraneh, Fatemeh Pazouki and Sharhzad Irani for help with translating non‐English language papers.
Thanks to the Cochrane Pregnancy and Childbirth editorial team for their support with the 2015 update.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Appendices
Appendix 1. CAM Field Register search strategy
(pregnan* OR antenatal OR prenatal) AND (nause* OR sickness OR vomit* OR emesis OR hyperemisis OR antiemetic)
Data and analyses
Comparison 1. P6 Acupressure versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Severity of nausea after treatment (of 4 days) using a 10 cm VAS | 1 | 100 | Mean Difference (IV, Fixed, 95% CI) | ‐1.70 [‐2.41, ‐0.99] |
| 2 No improvement in intensity of symptoms (while using wristbands) reported | 1 | 97 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.44, 1.39] |
| 3 Mean nausea score after day 3 using VAS | 1 | 40 | Mean Difference (IV, Fixed, 95% CI) | 0.10 [‐1.49, 1.69] |
| 4 Mean nausea score days 1‐3 (average) | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | 0.39 [‐0.80, 1.58] |
| 5 Mean total scores (Rhodes Index) days 1‐3 (average) | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | 1.17 [‐1.52, 3.86] |
| 6 Total Rhodes Index score on the 3rd day of intervention | 1 | 93 | Mean Difference (IV, Fixed, 95% CI) | ‐1.48 [‐4.10, 1.14] |
| 7 Severity of vomiting after treatment (of 4 days) as number of vomiting episodes | 1 | 100 | Mean Difference (IV, Fixed, 95% CI) | ‐0.9 [‐1.06, ‐0.74] |
| 8 Mean emesis scores days 1‐3 (average) | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | 0.26 [‐1.06, 1.58] |
Comparison 2. P6 Acupressure versus vitamin B6.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Nausea scores on day 3 | 1 | 66 | Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐2.24, 2.64] |
| 2 Poor symptom relief/amount of rescue medication (number of tablets) | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | ‐2.20 [‐3.98, ‐0.42] |
Comparison 3. Auricular acupressure versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Nausea/vomiting score (combined Rhodes Index score) on day 6 (3 days after treatment started) | 1 | 91 | Mean Difference (IV, Fixed, 95% CI) | ‐3.60 [‐6.62, ‐0.58] |
| 2 Number of anti‐emetic drugs used on day 6 (3 days after treatment started) | 1 | 91 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.37, 0.17] |
Comparison 4. Acustimulation therapy at P6 point versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Weight gain (in lbs) over 3 week period | 1 | 187 | Mean Difference (IV, Fixed, 95% CI) | 1.7 [0.23, 3.17] |
| 2 Dehydration: occurrences reported | 1 | 187 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.24 [0.07, 0.83] |
| 3 Ketonuria at the end of the trial | 1 | 187 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.15, 1.55] |
Comparison 5. Traditional acupuncture versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean nausea score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | ‐0.70 [‐1.36, ‐0.04] |
| 2 Mean dry retching score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐0.57, 0.17] |
| 3 Mean vomiting score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.58, 0.38] |
5.1. Analysis.
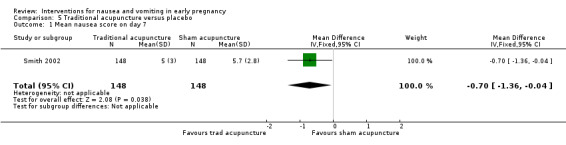
Comparison 5 Traditional acupuncture versus placebo, Outcome 1 Mean nausea score on day 7.
Comparison 6. P6 Acupuncture versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean nausea score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | ‐0.30 [1.00, 0.40] |
| 2 Mean dry retching score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | 0.10 [‐0.30, 0.50] |
| 3 Mean vomiting score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | ‐0.30 [‐0.78, 0.18] |
Comparison 7. Traditional acupuncture versus P6 acupuncture.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean nausea score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | ‐0.40 [‐1.12, 0.32] |
| 2 Mean dry retching score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | ‐0.30 [‐0.65, 0.05] |
| 3 Mean vomiting score on day 7 | 1 | 296 | Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐0.26, 0.66] |
Comparison 8. Ginger versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean nausea score (using Rhodes Index) on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | ‐1.38 [‐2.73, ‐0.03] |
| 2 Total Rhodes Index score on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | ‐2.52 [‐4.50, ‐0.54] |
| 3 Total Rhodes Index score on the 3rd day of intervention | 1 | 95 | Mean Difference (IV, Fixed, 95% CI) | 0.79 [‐1.89, 3.47] |
| 4 Total Rhodes Index score after 1 week treatment | 1 | 70 | Mean Difference (IV, Fixed, 95% CI) | ‐4.19 [‐6.65, ‐1.73] |
| 5 Little improvement in nausea | 1 | 23 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.10, 0.82] |
| 6 Improvement in nausea (mean change score) over 4 days of treatment: women available to follow up | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | 1.20 [0.22, 2.18] |
| 7 Improvement in nausea (mean change score) over 4 days of treatment: ITT analysis | 1 | 70 | Mean Difference (IV, Fixed, 95% CI) | 0.60 [‐0.51, 1.71] |
| 8 Improvement in nausea intensity after treatment (day 5) | 1 | 67 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.48 [1.07, 2.04] |
| 9 Average change in nausea score for days 1‐4, using 10cm VAS | 1 | 62 | Mean Difference (IV, Fixed, 95% CI) | 0.03 [‐0.88, 0.94] |
| 10 Symptoms improved (better or much better versus same) | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.96, 1.63] |
| 11 Mean vomiting severity (using Rhodes Index) on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | ‐1.14 [‐1.91, ‐0.37] |
| 12 Number of women continuing vomiting at day 6 | 1 | 22 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.42 [0.18, 0.98] |
| 13 Spontaneous abortion | 1 | 67 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.04, 3.33] |
| 14 Caesarean delivery | 1 | 67 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.64 [0.51, 5.29] |
Comparison 9. Ginger versus P6 Acupressure.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Total Rhodes Index score on the 3rd day of intervention | 1 | 98 | Mean Difference (IV, Fixed, 95% CI) | 2.27 [‐0.01, 4.55] |
Comparison 10. Ginger versus chamomile.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Rhodes Index score after 1 week treatment | 1 | 70 | Mean Difference (IV, Fixed, 95% CI) | 1.55 [‐0.34, 3.44] |
Comparison 11. Ginger versus vitamin B6.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Nausea vomiting score day 3 | 2 | 251 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.00 [‐0.25, 0.25] |
| 1.1 Rhodes Index | 1 | 123 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.09 [‐0.44, 0.27] |
| 1.2 10 cm VAS | 1 | 128 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.08 [‐0.27, 0.43] |
| 2 Post‐treatment number of vomiting episodes: day 3 | 1 | 128 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.60, 0.60] |
| 3 No improvement in symptoms | 2 | 360 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.47, 1.52] |
| 4 Spontaneous abortion | 2 | 360 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.17, 1.42] |
| 5 Stillbirth | 1 | 291 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.01, 2.72] |
| 6 Congenital abnormality | 1 | 291 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.13, 1.95] |
| 7 Antepartum haemorrhage/abruption, placenta praevia | 1 | 291 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.29, 3.36] |
| 8 Pregnancy‐induced hypertension | 1 | 291 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.34, 4.53] |
| 9 Pre‐eclampisa | 1 | 291 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.49 [0.43, 5.17] |
| 10 Preterm birth | 1 | 291 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.66 [0.40, 6.80] |
| 11 Arrhythmia | 1 | 123 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.05 [0.13, 73.40] |
| 12 Headache | 1 | 123 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.20 [0.01, 4.15] |
| 13 Heartburn | 2 | 251 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.35 [0.93, 5.93] |
| 14 Sedation or drowsiness | 2 | 251 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.48, 1.19] |
| 15 Caesarean delivery | 1 | 69 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.20, 2.09] |
11.5. Analysis.
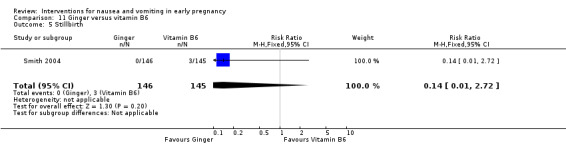
Comparison 11 Ginger versus vitamin B6, Outcome 5 Stillbirth.
11.7. Analysis.
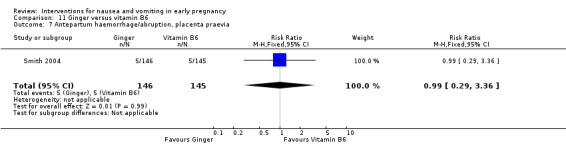
Comparison 11 Ginger versus vitamin B6, Outcome 7 Antepartum haemorrhage/abruption, placenta praevia.
11.8. Analysis.
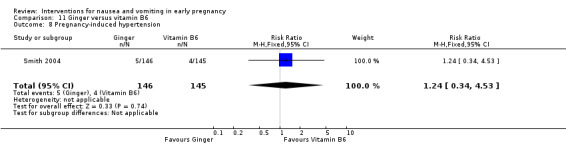
Comparison 11 Ginger versus vitamin B6, Outcome 8 Pregnancy‐induced hypertension.
11.9. Analysis.
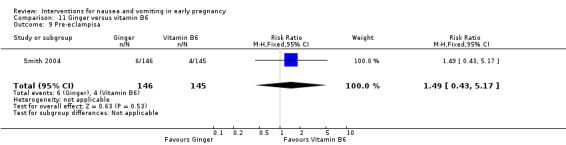
Comparison 11 Ginger versus vitamin B6, Outcome 9 Pre‐eclampisa.
Comparison 12. Ginger versus metoclopramide.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean score for nausea (using Rhodes Index) on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | 1.56 [‐0.22, 3.34] |
| 2 Mean score for vomiting (using Rhodes Index) on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | 0.33 [‐0.69, 1.35] |
| 3 Rhodes Index score on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | 1.89 [‐0.78, 4.56] |
Comparison 13. Ginger versus dimenhydrinate.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Drowsiness | 1 | 170 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.08 [0.03, 0.18] |
| 2 Heartburn | 1 | 170 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.44 [0.65, 3.20] |
Comparison 14. Lemon oil versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean PUQE score on day 3 of intervention | 1 | 100 | Mean Difference (IV, Fixed, 95% CI) | ‐0.46 [‐1.27, 0.35] |
| 2 Mean difference of total PUQE scores from baseline to day 3 of intervention | 1 | 100 | Mean Difference (IV, Fixed, 95% CI) | ‐1.50 [‐2.41, ‐0.59] |
| 3 Satisfaction with the given treatment | 1 | 100 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.47 [0.91, 2.37] |
Comparison 15. Mint oil versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Severity of nausea on day 4 | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | ‐0.88 [‐1.93, 0.17] |
| 2 Vomiting intensity on day 4 | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | ‐0.32 [‐1.45, 0.81] |
Comparison 16. Chamomile versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Rhodes Index score after 1 week treatment | 1 | 70 | Mean Difference (IV, Fixed, 95% CI) | ‐5.74 [‐8.31, ‐3.17] |
Comparison 17. Vitamin B6 versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean reduction in nausea score after 3 days | 2 | 393 | Mean Difference (IV, Fixed, 95% CI) | 0.92 [0.40, 1.44] |
| 2 Number of patients with emesis post‐therapy | 2 | 392 | Risk Ratio (M‐H, Random, 95% CI) | 0.76 [0.35, 1.66] |
Comparison 18. Vitamin B6 (high dose) versus Vitamin B6 (low dose).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean change in PUQE score from baseline to 2 weeks | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | ‐1.06 [‐2.05, ‐0.07] |
Comparison 19. Vitamin B6 versus dimenhydrinate.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Nausea and vomiting score after 3 days of treatment using Rhodes Index | 1 | 135 | Mean Difference (IV, Fixed, 95% CI) | 1.20 [0.47, 1.93] |
| 2 Drowsiness | 1 | 135 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.06, 0.34] |
Comparison 20. Hydroxyzine versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 No relief from nausea | 1 | 150 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.23 [0.15, 0.36] |
| 2 Spontaneous abortion (1st or 2nd trimester) | 1 | 115 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.17, 4.75] |
| 3 Perinatal mortality | 1 | 115 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.39 [0.06, 33.26] |
Comparison 21. Dicyclomine/ doxylamine/ pyridoxine versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 No improvement of symptoms | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only |
Comparison 22. Doxylamine and pyridoxine versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean difference in nausea/vomiting/retching (PUQE score) baseline to day 15 | 1 | 256 | Mean Difference (IV, Fixed, 95% CI) | ‐0.9 [‐1.55, ‐0.25] |
| 2 Requests for compassionate use of drug after day 14 | 1 | 256 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.49 [1.10, 2.02] |
| 3 Headache | 1 | 256 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.45, 1.48] |
| 4 Somnolence | 1 | 256 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.21 [0.64, 2.27] |
| 5 Difference in global assessment of well‐being from baseline to day 15 | 1 | 256 | Mean Difference (IV, Fixed, 95% CI) | 1.00 [0.38, 1.62] |
| 6 Time loss from employment in days | 1 | 256 | Mean Difference (IV, Fixed, 95% CI) | ‐1.45 [‐3.36, 0.46] |
Comparison 23. Thiethylperazine versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Poor relief from symptoms | 1 | 164 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.49 [0.31, 0.78] |
Comparison 24. Fluphenazine‐pyridoxine versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Poor response to treatment | 1 | 78 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.52 [0.27, 1.01] |
Comparison 25. Metoclopramide versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean score for nausea (using Rhodes Index) on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | ‐2.94 [‐4.55, ‐1.33] |
| 2 Mean score for vomiting (using Rhodes Index) on day 3 | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | ‐1.47 [‐2.33, ‐0.61] |
Comparison 26. Ondansetron versus metoclopramide.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Average number of nausea episodes on day 3 after treatment. | 1 | 70 | Mean Difference (IV, Fixed, 95% CI) | ‐0.12 [‐0.44, 0.20] |
| 2 Average number of vomiting episodes on day 3 after treatment. | 1 | 70 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐0.57, 0.17] |
Comparison 27. Ondansetron versus pyridoxine‐doxylamine.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Clinically significant (≥25mm on VAS) reduction in nausea after 5 days of treatment | 1 | 30 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.24 [1.24, 4.04] |
| 2 Sedation | 1 | 30 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.28, 2.02] |
| 3 Constipation | 1 | 30 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.18 [0.63, 7.50] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Babaei 2014.
| Methods | Double blind RCT. | |
| Participants | 140 women up to 16 weeks' gestation. | |
| Interventions | Vitamin B6 versus dimenhydrinate. 50 mg vitamin B6 every morning for 1 week or 50 mg dimenhydrinate every morning for 1 week. | |
| Outcomes | Primary outcome: change in nausea and vomiting scores by Rhodes Index; side effects. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated 'randomized'. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Stated both blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | Noted attrition, 3 in vitamin B6 and 2 in dimenhydrinate lost to follow‐up. |
| Selective reporting (reporting bias) | Low risk | Report on all outcomes. |
| Other bias | Low risk | None suspected. |
Basirat 2009.
| Methods | Double blind RCT. | |
| Participants | 65 women 7‐17 weeks' gestation, 30 to placebo group, 35 to ginger. | |
| Interventions | Ginger biscuits versus placebo biscuits. Intervention group: biscuits containing 0.5g ginger as fine powder; placebo: similarly prepared. Both groups ate 5 biscuits daily for 4 days. | |
| Outcomes | Primary ‐ change in nausea and vomiting scores by VAS graded by participants over the last 24 hours 0‐10 cm (0 = no nausea and 10 = severe nausea as bad as it could be). Follow‐up visit 7 days later scored again and average score recorded. Number of vomiting episodes per 24 hour period. Five‐item Likert scale of general ideas of patients about symptom improvement. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table. |
| Allocation concealment (selection bias) | Low risk | Similar looking packaging and biscuits. The treatment codes were kept in sequence in sealed black envelopes that could not be read through. As each participant entered the trial, she received the next envelope in the sequence which determined her assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Neither the physician nor the patients knew the composition of the biscuits administered. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | Noted attrition, 3 in ginger group did not take them due to hot spicy taste. |
| Selective reporting (reporting bias) | Low risk | Reports on all outcomes. |
| Other bias | Low risk | None suspected. |
Belluomini 1994.
| Methods | A randomised blinded study. | |
| Participants | 90 pregnant women, with gestation of 12 weeks or less by the completion of the study. Exclusion criteria were diagnosed hyperemesis gravidarum, diseases that cause nausea and emesis, and current use of anti‐emetic medication. | |
| Interventions | Treatment group received acupressure using an acupressure point (Nei Guan PC‐6); placebo point (on palmar surface of the hand, proximal to the head of the fifth metacarpal joint) used for the sham control group. Applied for 10 minutes 4 times per day. | |
| Outcomes | Nausea and vomiting were measured using the Rhodes Index of Nausea and Vomting Form‐2 (scale range of 0‐32, 3 subscales: nausea (duration, frequency and distress), vomiting (amount, frequency and distress) and retching (frequency and distress). Outcomes were measured each evening for 10 consecutive days; data from the first 3 days were used as pre‐treatment data; data from days 5‐7 were used to measure treatment effect. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Women were assigned by a randomised block design to P6 acupressure or sham acupressure group. How this was done is not described. Probably adequate, though size of blocks not stated. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Single‐blinding possible due to the nature of the intervention (P6 vs sham acupressure known to those administering them). |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | High risk | 30 of 90 participants did not complete the study (16 treatment and 14 control). Failure to return forms, very incomplete forms or loss to follow‐up explained attrition of 13 treatment and 12 control participants. The remaining attrition (3 treatment and 2 control) was explained as prescribing anti‐emetics, abdominal surgery and voluntary dropout. Though this high attrition rate might introduce bias, it is similar between groups. |
| Selective reporting (reporting bias) | High risk | Retching subscale results not reported. Subscale results for nausea and vomiting presented averaged for days 1‐3 and 5‐7; data from days 8, 9, 10 were not presented; it was reported in text that data from these days "demonstrated no significant differences between the treatment and placebo groups because nausea and vomiting had improved over time" (average gestation 8.5 weeks +/‐ 1.4 weeks). |
| Other bias | Low risk | Internal reliability of Rhodes Index reported for day 2 of pre‐treatment (r = 0.88); not explained why this day was chosen. Unlikely to introduce bias. |
Biswas 2011.
| Methods | Single‐masked RCT. | |
| Participants | 78 women between 6‐16 weeks' gestation with NVP, without having received any treatment for same; the study was completed by 63 women (withdrawn participants did not present for even the first follow‐up visit). | |
| Interventions | 150 mg standardised extract of dried ginger (LHR‐2445AE), in 1 tablet 3 times daily vs Doxinate (doxylamine 10 mg as succinate and pyridoxine 10 mg as hydrochloride). Compliance with medication was assessed by pill count and graded as excellent/ good/poor. 3 weeks of active treatment, follow‐up visits at the end of the first and second weeks. |
|
| Outcomes | Severity of nausea and vomiting recorded on a 100 mm VAS, on the day of each visit as well as averaged over the past week. Average number of spells of nausea or episodes of vomiting per day over the past week were also recorded. Subjective feeling of well‐being (binary yes/no) recorded at each visit. Diary card to record severity of their problem was held by participants. Routine laboratory tests (blood counts, liver function tests, serum creatinine and fasting glucose) were done at baseline and at the end of the study to assess safety. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomly allocated (using computer‐generated random number list) to 1 of the 2 groups. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants were blinded using coded packaging, investigators not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | Outcomes reported for all those who reported at first follow‐up (6 in group A and 5 in Group B were lost to follow‐up); 4 not eligible due to protocol violation, 2 in each group. |
| Selective reporting (reporting bias) | Low risk | All results reported. |
| Other bias | Low risk | None suspected. |
Bsat 2003a.
| Methods | Prospective randomised comparison of 3 drug regimens. | |
| Participants | 169 women with singleton pregnancies in first trimester presenting to their obstetrical provider with nausea and/or vomiting. | |
| Interventions | 3 "commonly prescribed pharmaceutical regimens in the outpatient management of nausea and vomiting in pregnancy", to "mirror local practices". Group A: 50 mg IM injection of pyridoxine, with metoclopramide 10 mg orally every 6 hours as needed. Group B: prochlorperazine as needed 25 mg rectal suppositories every 12 hours or 10 mg tablets orally every 6 hours as needed. Group C: promethazine 25 mg orally every 6 hours as needed. |
|
| Outcomes | Change in symptoms: scores 1‐5 on a scale which comprised: much worse, worse, same, better, much better; recorded by participants on third day of treatment. Responses then divided into 2 subgroups:‐those who answered 1‐3 (same‐worse) and those who answered 4‐5 (better). Women also recorded the number of emesis episodes the day before and on the third day of treatment; dry heaves (retching) were counted as nausea, but not vomiting episodes. Worsening of symptoms was evaluated and patient admission for hydration or inpatient management was considered on an individual basis. Hospitalisation for the specific management of nausea or vomiting was noted. Patients also recorded their "medication compliance". |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were divided into 3 groups based on a computer‐generated randomisation. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 12 patients lost to follow‐up (3, 5 and 4 from groups A, B and C respectively). 1 patient from Group A withdrew from the study with side effects (acute dystonic reactions, thought to be secondary to metoclopramide). |
| Selective reporting (reporting bias) | High risk | Results for "subjective response" presented only in graphical format; not usable. Emesis frequency only reported. States that "drug usage and compliance was comparable between all three groups", but no description of amount of each drug used (most were on an "as required" basis). |
| Other bias | Unclear risk | 2 drugs were given to Group A; this treatment was found to be most effective; it is not possible to identify whether 1 or both agents were effective. The authors note that combining 2 agents that may also both work independently may raise questions of fairness ‐ this was done to mirror local practices. Unclear who and where drugs were administered (e.g. IM injections on an "as required" basis). Study was done in out‐patient setting. |
Chittumma 2007.
| Methods | Randomised double‐blind controlled trial. | |
| Participants | 126 pregnant women at 16 weeks' gestation or less who had nausea and vomiting, required anti‐emetics, had no medical conditions, and were not hospitalised. | |
| Interventions | Treatment group: 2, 325 mg capsules of ginger or placebo group: 2, 12.5 mg identical capsules. Capsules taken 3 times daily before meals for 4 days. |
|
| Outcomes | Primary outcome: change of nausea vomiting scores (mean of post‐treatment minus baseline scores). Symptoms recorded at baseline and each day during treatment. The 3 physical symptoms of Rhodes's score were measured (episodes of nausea, duration of nausea and number of vomits); range lowest score of 3 to maximum of 15. Secondary outcomes measured: occurrence of side effects such as heartburn, arrhythmia, headache and sedation. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Women were randomly allocated. The randomisation of patients was done using a table of random numbers with blocks of 4 to receive ginger or vitamin B6. When using blocks of 4, it may be possible to predict sequence. |
| Allocation concealment (selection bias) | Low risk | The treatment code was concealed by placing the patient's assignments in sequence in sealed opaque envelopes that were drawn in ascending consecutive order. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind trial. Four patients (6.3%) in the ginger group correctly identified what they were taking, but none in the vitamin B6 group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 2 cases in the ginger group and 1 case in the vitamin B6 group were lost to follow‐up. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Other bias | Unclear risk | The authors chose a study period of 4 days because previous studies showed that the effect of ginger was evident within a few days of treatment and too long a period would result in a higher rate of participant noncompliance and loss to follow‐up. 1 person in the ginger group and 4 in the B6 group took other medications (common cold, headache); 3 of the ginger group and 4 of the B6 group took other ginger products during the trial. At the end of the trial, the use of other antiemetics was reported by 7 of 12 patients (5.7%); unclear what this means. |
Ensiyeh 2009.
| Methods | Double‐blind RCT. | |
| Participants | Pregnant women with nausea, with or without vomiting, who first attended the antenatal clinic at or before 17 weeks' gestation. Women were excluded if they had other diseases that might cause nausea and vomiting, had mental health problems, had taken tablets in the previous week that might have aggravated nausea or vomiting symptoms, refused to participate or were unable to return 1 week later for follow‐up. During the study, 80 women were eligible and 70 agreed to participate, 35 randomised to each group. |
|
| Interventions | Ginger 1 g/day or vitamin B6 40 mg/day for 4 days (for both groups: 2 capsules daily, after breakfast and dinner). | |
| Outcomes | Severity of nausea using a VAS, number of episodes of vomiting recorded, 3 times daily during treatment for 4 days (average daily scores and mean nausea score calculated over the 4 days of treatment). At 7‐day follow‐up, treatment response was assessed using a 5‐point Likert scale (much worse, worse, same, better, much better). Median change in severity of nausea and number of vomiting episodes compared by group. Secondary outcomes also measured were: side effects and adverse effects on pregnancy outcomes such as abortion, preterm birth, congenital anomaly, perinatal death and mode of birth. Compliance was assessed by pill count and by asking women if they took the drugs. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | 35 women were randomised to the ginger group and 35 to the vitamin B6 group, using a table of random numbers. |
| Allocation concealment (selection bias) | Unclear risk | No details given. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 1 woman randomised to vitamin B6 group did not return to the clinic, so she was excluded from the study. Results presented by ITT, after excluding the 1 woman. |
| Selective reporting (reporting bias) | High risk | Only changes in scores and number of vomiting episodes presented, as well as frequency of improvement in symptoms (by category much worse to much better) The authors stated that data collection and follow‐up took 12 weeks; also stated that pregnancy outcomes including preterm birth, perinatal death, congenital anomaly, mode of delivery were assessed, which could not have been concluded within 12 weeks. Median changes in scores presented only. Compliance/adherence to treatment is not recorded. |
| Other bias | Low risk | Power analysis was said to be used to determine the sample size, resulting in 31 per group to achieve a power of 0.80 with an alpha of 0.05; however effect size (presumably for primary outcome) needed for the calculation is not stated. Not likely to introduce bias. |
Erez 1971.
| Methods | Double‐blind study/evaluation. | |
| Participants | 150 pregnant women in the first 2 months of pregnancy, reporting recurrent nausea and had vomited at least 3 times per week over the previous 2 weeks. | |
| Interventions | Hydroxyzine hydrochloride 25 mg capsules twice daily orally (morning and 2 pm) or identical capsules of placebo for 3 weeks. | |
| Outcomes | Effectiveness of the medication graded subjectively by the patient as follows: complete relief, partial relief, no relief. Evaluation of effectiveness of drug and side effects was made 3 weeks after starting the medication. Side effects were evaluated (not stated how, by whom). "Fetal wastage" and fetal anomalies checked. |
|
| Notes | Initially no attempt was made to eliminate causes of recurrent vomiting other than pregnancy. Comments that spontaneous remission or psychological factors may have played a role and this was evident from the fact that 22% of the placebo group had some response. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | By random selection from the available preparations, 100 patients received Hydroxyzine and 50 patients received the placebo. There was a 2:1 ratio of treatment: control participants. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. Blind evaluation of drug efficacy and any side effects was made 3 weeks after the institution of the medication. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | No missing data for follow‐up at 3 weeks (primary outcome of symptom relief); obstetrical outcome reported for 115 (of 150, 23%); 21 of treatment group and 14 of control group could not be evaluated as they delivered elsewhere; not considered high risk relating to symptomatic relief as primary outcome. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Other bias | Low risk | None suspected. |
Fan 1995.
| Methods | Randomised comparison/observation. | |
| Participants | 302 patients with pregnant vomiting, with menstruation suspended for more than 2 months (maximum not stated). | |
| Interventions | Patients were treated according to differentiation of symptoms and signs and types of syndromes (1. deficiency of both the spleen and the stomach, 2. incoordination between the liver and the stomach). 2 treatment groups: Moxibustion group (specified points). Chinese drug group (specified herbs). |
|
| Outcomes | Criteria for evaluating the therapeutic effect: cured, improved, ineffective. Not described who measured these. "Cure" defined as disappearance of symptoms after treatment for 1 week, but outcome measurement time point(s) not specified. | |
| Notes | Gestation unclear; more than 8 weeks since last menstrual period. Concluding statement: "the therapeutic effect of moxibustion is superior to that of Chinese drug therapy. It is also simple and easy to be performed, and it an ideal therapy". Unclear about study design: first paragraph states: "In the past several years, the author has cooperated with some gynaecologists from this and other hospitals to treat pregnant vomiting with moxibustion therapy and achieved significant therapeutic effect. It is introduced as follows. General data. 302 and two [sic] patients with pregnancy vomiting were randomly divided into two groups, 151 cases in each group". |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Patients were randomly divided into 2 groups; no further details. |
| Allocation concealment (selection bias) | Unclear risk | No detail. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Not described who recorded symptoms, classified as cured/improved/effective based on symptomatic relief, presumed to be self‐reported (e.g. 'symptoms of nausea and vomiting were relieved'). |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All 151 per group reported on (total of 302). |
| Selective reporting (reporting bias) | Low risk | Reported as % cured/improved. States that all had improvement or cure. |
| Other bias | Low risk | None suspected. |
Geiger 1959.
| Methods | Within a series of studies; a double‐blind comparative experiment, a controlled double‐blind study. | |
| Participants | 100 ward (not explained) and private patients. | |
| Interventions | Bendectin (10 mg each of Bentyl (dicyclomine), Decapryn (doxylamine) and pyridoxine), 2 tablets nightly, an additional tablet in the morning as required. Placebo (not described). |
|
| Outcomes | Relief from nausea and vomiting: complete, partial or no relief. No description of how or when outcomes were measured. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No description about randomisation. |
| Allocation concealment (selection bias) | Unclear risk | No description about allocation concealment; tablets were in envelopes with an identification number. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 1 patient in treatment group received medication for 1 day, otherwise all patients' outcomes reported in results. |
| Selective reporting (reporting bias) | Low risk | Outcomes reported. |
| Other bias | Unclear risk | 2 patients were included in both the treatment and control groups as they received medication on 2 separate occasions during the study. |
Ghahiri 2011.
| Methods | Clinical trial. | |
| Participants | 70 women with NVP in first trimester. | |
| Interventions | Ondansetron 4 mg every 12 hours vs metoclopramide 10 mg every 12 hours, both orally for 3 weeks. For metoclopramide group, after 1 week if the episodes of NVP did not decrease to half, metoclopramide was stopped and they started on ondansetron. For ondansetron group, if ineffective, they were started on metoclopramide. It does not appear that there was any cross‐over between interventions, but this is not certain. | |
| Outcomes | Daily frequency of nausea and vomiting, medication side effects, number of tables taken were studied before starting the intervention, 3 days, 1 week, 2 weeks and 3 weeks after treatment in both groups. | |
| Notes | Article translated from Arabic. Stated in conclusion that Ondansetron is a safe medication that we can use to treat severe NVP. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 35 per group, no missing data reported. |
| Selective reporting (reporting bias) | Low risk | All outcomes measured are reported. |
| Other bias | Low risk | None apparent. |
Jamigorn 2007.
| Methods | A single‐blind randomised study. | |
| Participants | 66 pregnant women with mild to moderate nausea and vomiting between 6 and 12 weeks' gestation, in the outpatient setting. | |
| Interventions | The patients in the acupressure group were advised to apply Sea‐Bands on P6 point and identical looking tablets were used as placebo in the same regimen as vitamin B6. Those in vitamin B6 group were advised to apply Sea‐Bands on the dummy point and 50 mg tablets of vitamin B6 were prescribed every 12 hours for 5 days. | |
| Outcomes | Primary outcome: self‐recorded nausea and vomiting according to Rhodes Index of Nausea and Vomiting form 2 (8 items, 5‐point LIkert‐type instrument). Women evaluated their symptoms twice daily for 7 days. Secondary outcomes: weight gain and medication use‐ use of the rescue drug (oral dimenhydrinate 50 mg every 6 hours when required). |
|
| Notes | The authors state that the Rhodes Index was "translated into Thai and tested for validity and reliability by experts" but provide no other details on this. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was done into 2 groups (acupressure and vitamin B6 groups) by an independent remote researcher who had no prior knowledge of the patients by using a block of 4 technique. |
| Allocation concealment (selection bias) | Low risk | Sequential sealed envelopes picked by independent, remote researcher. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Single‐blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 6 patients did not complete the study (3 in each group). The attrition of the 6 people was explained as follows: "one patient from the withdrawal [sic] group was lost to follow‐up", 1 had irritation from the acupressure band, 2 patients lost their acupressure devices, 2 patients had incomplete forms. ITT analysis was performed, counting all withdrawals as treatment failures. |
| Selective reporting (reporting bias) | High risk | All outcomes reported but change in Rhodes score only presented graphically; results for weight change and rescue drug use presented fully. |
| Other bias | Unclear risk | The initial Rhodes Index score in the B6 group was higher than acupressure group; stated to be not significant, sample size 33 per group. The authors acknowledge that it is possible that the rescue drug provided a large reduction of the symptoms but that it was not possible to exclude it for ethical reasons. They state that the use of the rescue drug did not differ by group (although they also report 0.6+/‐1.6 tablets vs 2.8 +/‐4.7 tablets P > 0.05 in acupressure and vitamin B6 groups respectively). They also state that the improvement of nausea and vomiting in the present study may be spontaneous due to a placebo effect, the additional medications used, or either of the treatments. |
Keating 2002.
| Methods | Double‐blind, placebo‐controlled RCT. | |
| Participants | Pregnant women in first trimester attending obstetric visit. 26 women were enrolled with 14 patients in the intervention group and 12 in the placebo group. | |
| Interventions | Intervention group: tablespoon of syrup 250 mg ginger, honey and water Placebo: water, honey, lemon oil. 1 tablespoon mixed in 4‐8 ounces of cold water 4 times/day. |
|
| Outcomes | Each participant kept a daily diary for first 2 weeks to record the number of syrup drinks ingested and the degree of nausea and vomiting. Degree of nausea and vomiting "A numerical scale of 1 through 10 was used to quantify the level of nausea, number of vomiting episodes and the patient’s perspective of her daily functioning related to her symptoms". No information about the scale. Outcomes reported: point improvement on the nausea scale; number of vomiting episodes; maintenance/gain in weight. |
|
| Notes | A statistical analysis was not applied to the results because of the small numbers. The ginger syrup is prepared and sold by New Chapter Inc (Brattleboro, Vt). The company also prepared the placebo syrup and provided both syrups free of charge. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants were randomised to the placebo or the study group by computer‐generated numbers matching the numbers on identical‐appearing bottles of ginger or placebo syrup. |
| Allocation concealment (selection bias) | Unclear risk | Nothing stated about allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | Attrition from the placebo group ‐ 1 woman did not take the study drink as her nausea resolved, 2 women stopped the study on days 7 and 11 because of no improvement and they were prescribed anti‐emetics. In the ginger group, 1 woman stopped the study at day 5 as she could not tolerate the taste of the drink; another woman stopped the study on day 10 when her symptoms resolved. Results are reported for days 6, 9, 14, for groups with varying sizes, linked with this attrition. |
| Selective reporting (reporting bias) | High risk | Reported 4‐point, 2‐point improvement in nausea; reported vomiting on day 6 was not pre‐specified and seems arbitrary. Patient’s perspective on her daily functioning ‐ not reported. Weight gain/loss reported in results ‐ not specified as an outcome. |
| Other bias | Low risk | |
Khavandizadeh 2010.
| Methods | A randomised clinical trial. | |
| Participants | 100 primigravida women with 10‐16 weeks' singleton pregnancy gestation, minimum 2 days of nausea and vomiting, no anti‐emetic use during past week. | |
| Interventions | Acupressure using a 'sea band' placed in Neiguan point (4‐5 cm above the first transverse crease of the wrist) on hands vs sea band placed on points other than Neiguan point. Treatment lasted 4 days, started on day 2 of the study. | |
| Outcomes | Severity of nausea measured by VAS. Severity of vomiting was measured and rated using 'East Oncology criteria', where mild is 1‐2 episodes per day, 3‐5 episodes is considered moderate and more than 5 severe. | |
| Notes | Abstract in English, full text article translated from Farsi for data extraction. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Women were divided randomly into 2 groups. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Not described, though placebo implies single‐blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | No dropouts from study noted. |
| Selective reporting (reporting bias) | High risk | Data recorded daily but only reported as 'before and after treatment', assuming day 1 and day 6. |
| Other bias | Low risk | None apparent. |
Knight 2001.
| Methods | Participant‐ and observer‐masked RCT. | |
| Participants | 55 pregnant women, gestation between 6 and 10 weeks. | |
| Interventions | Acupuncture ‐ fully described. Sham with a cocktail stick. 15 minute treatments, twice in the first week and once weekly for 2 weeks, minimum number of treatments was 3. |
|
| Outcomes | Primary outcomes measured using a 100 mm VAS ‐ marked no nausea to nausea worst imaginable. Completed the scale daily to represent the worst experience of nausea in the previous 24 hours. Also recorded number of times they vomited in past 24 hours; plus adverse effects. Hospital Anxiety and Depression Scale as a secondary measure ‐ at baseline and immediately after the last treatment. Overall effectiveness ‐ within 2 weeks completion of treatment, using 5‐point LIkert‐type: much worse (1) to very much better or cured (5). |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants randomly assigned to 2 groups. Computer‐generated random numbers, stratified for severity of nausea, randomisation in blocks of 4. It may be possible to predict randomisation sequence in small blocks. |
| Allocation concealment (selection bias) | Low risk | By opening opaque sequentially numbered envelopes containing codes. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. In response to the question about masking, one woman in each group believed she might have had sham treatment, whereas all others believed they had received acupuncture or were not sure. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | High risk | 11 women from 55 (20%) were lost from the study. Acupuncture group: 5 people dropped out for no reason and 1 was admitted for hyperemesis. Sham acupuncture group: 1 withdrew consent before treatment; 2 dropped‐out for no reason, 1 had a missed abortion and 1 was admitted for hyperemesis. ITT analysis performed. |
| Selective reporting (reporting bias) | High risk | Number of vomiting episodes not reported; state that women failed to record systematically data on vomiting. Median scores reported only (data not normally distributed; failed Mauchly's test of sphericity). Median rating of 4 (range 3‐5) for global effectiveness for both groups, reported by the authors as "indicating an overall level of satisfaction with the treatment", implying satisfaction with sham treatment also. |
| Other bias | Low risk | Authors state limitation of availability of acupuncturist, variable times between treatments for some women. Sham procedure might have placebo effects (A‐delta fibres stimulated). |
Koren 2010.
| Methods | Randomised, double‐blind, multi‐centre placebo‐controlled trial. | |
| Participants | 298 assessed for eligibility, 18 excluded, 280 women assigned to groups, though 19 withdrew before receiving any dose of study medication (7 from treatment group and 12 from placebo group), leaving 261 women in the trial, 133 received treatment, 128 received placebo. 7‐14 weeks' gestation, with NVP with a PUQE score of >= 6 and had not responded to conservative management including dietary/lifestyle advice. | |
| Interventions | Doxylamine succinate 10 mg and pyridoxine hydrochloride 10 mg delayed release preparation (as Diclectin) vs similar‐appearing placebo. 2 tablets administered at bedtime on day 1, is symptoms persisted, 2 tablets on day 2 at bedtime and 1 tablet on morning of day 3; assessed in the clinic on day 4, if symptoms persisted directed to take a 4th tablet in the mid afternoon on day 4; daily dose was minimum of 2 tablets up to 4 tablets per day. 15‐day study, tablets administered on 14 days. Compassionate use of the product they had received was offered to participants after 15 days, recorded for 30 days, after that only serious adverse effects were recorded. | |
| Outcomes | Nausea, retching and vomiting measured using PUQE scoring system; measured once daily in the morning before medication, global assessment of well‐being scale on PUQE on days 1, 8, 14. Secondary outcomes recorded were: time loss from employment, compliance with medication and adverse effects, numbers continuing with (blinded) continued compassionate use of their medication; numbers who used concurrent use of alternate therapy for NVP such as nutritional modifications, teas, aromatherapy, massage and yoga. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Interactive voice response system provided study sites the ability to randomly assign a participant. |
| Allocation concealment (selection bias) | Low risk | Voice response system facilitated allocation of participants. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind study. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All participants accounted for; 7 lost to follow‐up in treatment group, 19 in placebo group. |
| Selective reporting (reporting bias) | High risk | Data recorded daily but only changes from baseline to end point (at 15 days) are reported; 'day‐by‐day area under the curve for change in PUQE from baseline' are reported. |
| Other bias | Low risk | None apparent. |
McGuiness 1971.
| Methods | Double‐blind comparison. Tablets supplied in bottles serially numbered from 1 to 100 and each contained 28 tablets, either the active product or lactose. | |
| Participants | Pregnant women who complained of nausea and vomiting in the first trimester; no women admitted to the trial after 20 weeks; 1 woman entered the trial twice with 2 pregnancies. General practice setting. Results reported for 41 women in intervention group, 40 women in control group. It was not stated how many women entered the trial. | |
| Interventions | Intervention group: Debenox (a mixture of dicyclomine, doxylamine and pyridoxine) 2 tablets at bedtime each night (dose not stated) for 14 consecutive nights. Control group: inert dummy tablets of identical appearance. |
|
| Outcomes | Change in grade of nausea or vomiting at the second visit compared to the first (time between visits not specified). Symptoms were graded according to severity between Grade 0 and 4 (no explanation or validation information given, no sources cited). Grade 0: no nausea or vomiting (only applicable on the second visit); Grade 1: slight nausea only which is acknowledged only on questioning; Grade 2: more severe nausea complained of by the patient spontaneously; Grade 3: vomiting once or twice a day; Grade 4: more severe vomiting 3 or more times a day. Side effects were also reported ‐ though these were not mentioned as being measured. |
|
| Notes | Within the introduction the authors state that Debenox had been in use for many years in their practice and that "the absence of untoward side actions with 'Debenox', in particular teratogenesis, has been amply demonstrated by the passage of 12 years". “Thanks are due to Dr J. P. Birkett, Merrell Division, Richardson‐Merrell Limited for supplies of inert and active tablets, statistical aid and secretarial help". |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Nothing stated about randomisation. |
| Allocation concealment (selection bias) | Low risk | Implied "A sealed code was available to us in case of emergency but this was not broken throughout the course of the trial, since no untoward reactions occurred". |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Data were collected by an independent observer; based on women's symptoms. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | High risk | No information of number of women who entered the trial so it is not possible to establish if there was any attrition. |
| Selective reporting (reporting bias) | Low risk | Reports on pre‐specified outcome. |
| Other bias | Low risk | None apparent. |
Modares 2012.
| Methods | Triple‐blind randomised placebo‐controlled trial. | |
| Participants | 105 pregnant women with mild‐moderate NVP based on Rhodes Index, between 6‐16 weeks' gestation. Those who dropped out from the study were replaced by a new member (timing and extent of replacements not described). | |
| Interventions | Ginger capsules vs chamomile capsules vs placebo capsules, twice per day for 1 week. Ginger capsule was extracted from ginger root which was powdered, 500 mg each and chamomile capsule had 500 mg of dried flower of German chamomile. Placebo was 500 mg capsule of starch. | |
| Outcomes | Nausea and vomiting using the Rhodes Index, completed daily before bedtime for 2 weeks, 1 week pre‐trial. | |
| Notes | Abstract in English, full text translated from Farsi for data extraction. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Allocated by lottery using coloured cards. |
| Allocation concealment (selection bias) | Unclear risk | Unclear regarding 'coloured cards'. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Triple‐blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Unclear risk | 35 in each group for analysis. Women who left the study were to be replaced by others, but not stated if this occurred. |
| Selective reporting (reporting bias) | High risk | Only baseline and end point scores reported, though recorded daily. |
| Other bias | Low risk | None apparent. |
Mohammadbeigi 2011.
| Methods | Randomised double‐blind controlled trial. | |
| Participants | 120 pregnant women with NVP were evaluated, 18 were excluded and 102 were allocated to 3 groups, 34 per group. Power calculation indicated 28 per group, 'downflow' of 20% led to 34 per group. | |
| Interventions | Ginger 200 mg (ginger essence) vs metoclopramide 10 mg vs placebo (flour), all capsules, 3 times per day. | |
| Outcomes | Severity of nausea and vomiting measured by the Rhodes Index translated into Persian, with face validity and internal reliability tested, completed twice per day, 9 am and 5 pm for 5 days. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | A person who assisted the study conducted the randomisation, she gave medicines to the patients for 5 days. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Unclear re person administering medications, participants appear to be blinded by use of identical capsules. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All 34 women in each group completed the study. |
| Selective reporting (reporting bias) | Low risk | Full results reported. |
| Other bias | Low risk | None apparent. |
Newlinds 1964.
| Methods | Clinical trial. | |
| Participants | 225 pregnant women in the first and 2nd trimesters of pregnancy. | |
| Interventions | Thiethylperazine 30 mg daily. Placebo. |
|
| Outcomes | Therapeutic response: good, fair, poor. No information on time point of evaluation(s). | |
| Notes | The patients were not told they were taking part in a trial. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Staff reported to be blind to group allocation ‐ not described how. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | 'Patients did not know they were taking part in a trial.' |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | High risk | High attrition: 45 (20% of 225, 19 from treatment group, 26 from placebo group) were not included in the analysis because of failure to return for assessment, transfer to another hospital or failure to take the tablets (breakdown by reason not given). Results about therapeutic response reported for 180 patients (but 8 from treatment group and 8 from placebo group were not classified "because of equivocal evidence, intercurrent illness or abortion"), results for fetal outcome reported for 147 patients. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Other bias | Low risk | None apparent. |
Norheim 2001.
| Methods | RCT. | |
| Participants | 97 pregnant women, 6‐12 weeks' gestation, with nausea for at least 1 week before trial entry. 139 women responded to the study invitation, 97 women took part (symptoms disappeared, too ill, too late in pregnancy). |
|
| Interventions | Acupressure group: wristbands (with button/knob on the inside) day and night on Neiguan point of both arms. Placebo group: wristband (with felt patch in stead of button) identical on the outside to acupressure band. 4 day run‐in, 4 day intervention, 4 day follow‐up. |
|
| Outcomes | Symptoms of nausea and vomiting recorded daily ‐ 3 recordings. What problems they had: no problems, nausea, vomiting. How many hours they had suffered. Every evening an overall evaluation of their symptoms on a VAS (0‐5 no problems to worst thinkable level of nausea and vomiting). |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation in blocks of 20. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double‐blind. No patient recognised the type of wristband they were given by the instructor though the control group guessed better what type of band they had used. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All 97 participants reported on in results: 13 women who did not complete all of the daily forms were assigned values equivalent to the last reported value on the outcome variables. |
| Selective reporting (reporting bias) | High risk | Unclear about numbers per group in results tables (%s presented). |
| Other bias | Low risk | The authors highlight potential selection, information and performance of intervention bias ‐ but these appear to be no greater than for other similar studies. |
O'Brien 1996.
| Methods | RCT. | |
| Participants | 161 women with symptoms of nausea with or without vomiting and retching during pregnancy. Gestational age for most (78.6%) women was < 12 weeks, maximum gestation 24 weeks (not stated for how many). | |
| Interventions | P6 (Neiguan) acupressure group ‐ band applied for 5 days, removed morning of day 6. Placebo acupressure group (acupressure band inappropriately placed). Control group ‐ no treatment. 7‐day study. |
|
| Outcomes | Symptoms of nausea and vomiting, using Rhodes Inventory of Nausea and Vomiting (Form 2), measuring prevalence and amount of distress caused by symptoms over 12‐hour period, recorded twice daily from entry to the study to 6 days later. | |
| Notes | Gestation up to 23.6 weeks; no raw usable data provided. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Use of a process of block randomisation (size of blocks not specified), computer‐generated. |
| Allocation concealment (selection bias) | Low risk | The blocks of group assignments were computer‐generated and placed in numbered sealed envelopes before the study began. Participants were given numbers that corresponded with their envelope numbers and this was determined by the order in which they entered the study. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Treatment and placebo groups unaware of group allocation; blinding not possible for no treatment group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 12 participants withdrew at various times during the study (5 lost of interest in evaluating their symptoms during the study, 3 for disappointment at being assigned to control group, 2 were hospitalised for severe symptoms and 4 refused to discontinue the intervention at the appropriate time). |
| Selective reporting (reporting bias) | High risk | Results reported graphically only, as mean squares. |
| Other bias | Low risk | None apparent. |
Oliveira 2014.
| Methods | Double‐blind RCT. | |
| Participants | 36 women with gestation of less than 16 weeks entered study. | |
| Interventions | Ondansetron vs pyridoxine‐doxylamine; Ondansetron 4 mg plus one placebo to take every 8 hours for 5 days versus 25 mg pyridoxine and 12.5 mg doxylamine taken every 8 hours for 5 days. | |
| Outcomes | VAS for nausea and vomiting both 0‐100 mm (no nausea/vomiting to worst imaginable), value of 25 mm indicated significant reduction; pill count done at end of study; side effects. Measured at baseline and 5‐7 days after treatment. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated program randomly allocated participants. |
| Allocation concealment (selection bias) | Low risk | 1 pharmacist prepared all medications and sealed bottles in Identical numbered brown bags. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The dispensing pharmacist, treating provider, patient and enrolling investigator were blinded to the medication regimen. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | Appear to report. 5 lost to follow‐up and initial data lost on 1 more; Missing data were estimated by multiple imputation over variables by group. |
| Selective reporting (reporting bias) | Low risk | Report on all outcomes. |
| Other bias | Low risk | None suspected. |
Ozgoli 2009.
| Methods | Single‐blind RCT. | |
| Participants | 70 pregnant women under 20 weeks' gestational age, without any surgical or medical history, without a history of smoking or drug use, and with mild or moderate nausea with or without vomiting were recruited to the study. | |
| Interventions | Treatment group: 1 g ginger daily (as 4, 250 mg ginger capsules, 1 capsule morning, noon, afternoon and night) for 4 days. Control group: placebo capsules, similar in appearance to ginger capsules, containing only lactose, for 4 days. |
|
| Outcomes | Nausea severity and intensity on 0‐10 VAS twice daily; number of vomiting episodes daily; general changes to nausea and vomiting recorded during interview with researcher after 4 days of treatment. Adherence to dietary advice was also recorded and assessed by interview after day 4. The incidence of unspecified "complications" was also recorded. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly assigned, no details given. |
| Allocation concealment (selection bias) | Unclear risk | Stated that the experimental group was matched with the control group regarding demographic and obstetrical characteristics. The results section states that matching groups on these characteristics did not reveal any significant differences between the 2, so maybe matching relates to comparisons after allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Single‐blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Unblinded researcher interviewed the participants at the end of the study; women recorded outcome data for days 1‐4 of the study. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 67 women completed the study; 3 from the experimental group failed to complete the after‐treatment questionnaire. |
| Selective reporting (reporting bias) | High risk | Results reported unclearly; daily scores/results not presented, presented by number of assessments, not participants. Overall percentage improvement by group then reported in the text and tables (based on 2 daily measurements for 4 days per person per group). |
| Other bias | Low risk | None apparent. |
Pasha 2012.
| Methods | Double‐blind RCT. | |
| Participants | 150 women invited to participate, 83 excluded (all explained), 67 started the trial, 60 completed it. women were selected from the 'prenatal wards of seven selected health clinics' | |
| Interventions | Pure mInt essential oil (4 drops) in a bowl of water placed in the floor near the bed for 4 nights vs 4 drops of normal saline. Some mint oil was poured to the inner part of the drug's lid so that mothers receiving the normal saline cannot be aware of being allocated to this group. | |
| Outcomes | Severity of nausea using a 10 cm VAS and severity of vomiting by counting episodes 7 days before, 4 days of study and 7 days after the study. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Divided into 2 groups with block randomisation. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All participants accounted for; 3 lost to follow‐up from treatment group, 4 from control group. |
| Selective reporting (reporting bias) | High risk | Daily mean scores for nausea reported in graph without standard deviations (SDs), SDs only provided for average scores over 4 days; difference average scores for nausea intensity given in text of results and in a Figure. For vomiting intensity, only results averaged 4 days scores reported, with SDs. |
| Other bias | Low risk | None apparent. |
Pongrojpaw 2007a.
| Methods | RCT. | |
| Participants | 170 pregnant women less than 16 weeks' gestation, with symptoms of nausea and vomiting. | |
| Interventions | Group A: received 1 ginger capsule (0.5 g ginger powder) twice daily. Group B: identical capsule of 50 mg dimenhydrinate twice daily. |
|
| Outcomes | Primary outcome: improvement in nausea and vomiting symptoms. Degree of nausea measured using a 10 cm VAS to grade the severity of nausea over past 24 hours on first visit; on the following 7 days of treatment recordings were made twice daily in the morning and evening. Number of episodes of vomiting recorded daily. Secondary outcomes: occurrence of side effects such as drowsiness, heartburn, palpitation and mouth dryness. |
|
| Notes | Results difficult to interpret. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomly allocated ‐ no detail. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Identical capsules, double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 11% attrition: 8 women from ginger group and 11 women from dimenhydrinate group were lost to follow‐up (no further details given). |
| Selective reporting (reporting bias) | High risk | Unclear reporting of results; many tests. Explained tests due to high variation in pre‐intervention scores. |
| Other bias | Low risk | None apparent. |
Price 1964.
| Methods | A double‐blind placebo‐controlled study. | |
| Participants | 78 patients complaining of nausea or vomiting in pregnancy, gestation was over 20 weeks for some participants: 13‐24 weeks' gestation: 8 in treatment group, 4 in placebo. 25‐36 weeks: 6 in placebo group. Not specified: 1 in placebo group. |
|
| Interventions | Treatment group: fluphenazine 1 mg (repeat action tablet) plus 50 mg pyridoxine. Placebo: identically appearing placebo tablets. |
|
| Outcomes | Intensity of nausea and vomiting graded by women at outset and at the conclusion of 1 week of therapy. 6‐point scale (0‐6) ranged from no nausea or vomiting (0) to vomiting more than 3 times/day (6). Initial symptoms: 1‐2 classified as mild, 3‐4 as moderate and 5‐6 as severe. Effectiveness was measured by deducting the post‐treatment score from the initial score ‐ therapeutic response for each category of initial symptoms is expressed as excellent, good or poor by proper assignment of numerical values (based on their initial score). | |
| Notes | Later gestation of some participants in placebo group. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Details of how the randomisation sequence was generated was not clear. "Investigator bias is eliminated by the provision of a numbered series of bottles in which drug and identically appearing placebo tablets are randomly distributed". |
| Allocation concealment (selection bias) | Unclear risk | Not described ‐ patients were given 1 of successively numbered bottles in the series. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | 'Intensity of nausea and vomiting was graded according to' a numerical scale; not stated who graded, though implies self‐reported for symptoms. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All participants included in reported results. |
| Selective reporting (reporting bias) | Low risk | Outcomes reported according to classification. |
| Other bias | Unclear risk | Baseline imbalance. |
Puangsricharern 2008.
| Methods | RCT. | |
| Participants | 98 pregnant women with symptoms of nausea and vomiting, of not more than 14 weeks' gestation were recruited; exclusion criteria: women with molar pregnancy, multifetal pregnancy, blighted ovum, hyperemesis gravidarum, or current use of anti‐emetic medication. | |
| Interventions | Treatment group: auricular acupuncture, using round magnetic balls as ear pellets. These were placed with adhesive tape at the auricles of both ears (on auricular point at inner surface of auricle at the concha ridge zone, according to the meridians of Traditional Chinese Medicine). Women in this group were instructed to start pressing the magnets for 30 seconds 4 times a day (before meals and at bedtime), starting on the third day until the 6th day. First 2 days used as control days. Control group: no treatment, except oral anti‐emetic drugs (as below). Both groups were allowed to take 1 tablet of 50 mg dimenhydrinate every 6 hours as required if they could not tolerate their symptoms; remaining tablets were counted at end of 1 week of the study. |
|
| Outcomes | Frequency, duration and distress of nausea and vomiting and retching symptoms was measured using the Rhodes Index (range 0‐32, 8 5‐point self‐report items); completed every morning for 6 days. Scores from days 4‐6 used to measure treatment effect. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were randomised using a random table of numbers. |
| Allocation concealment (selection bias) | Unclear risk | No details stated. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 91 patients completed the study. 7 patients lost to follow‐up, 4 in the treatment group, 3 in the control group. No explanation given. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. Stated in results section that no 1 in treatment group experienced any adverse effect from acupressure and satisfaction with treatment is also reported as (% of treatment group satisfied). Adverse effects and satisfaction not stated as outcomes to be measured. |
| Other bias | Unclear risk | Differences between groups on education, income and occupation within baseline characteristics reported (women in control group were more educated, higher income and a higher percentage were housewives, in the occupational category). |
Rad 2012.
| Methods | Single‐blind clinical trial. | |
| Participants | 80 pregnant women with NVP. | |
| Interventions | KID 21 Point (Youmen) Acupressure vs sham acupressure, 20 minutes per day for 4 days. The KID21 point on the abdomen is illustrated and explained. All women were given 'routine tips' and 'all pregnant women have taken vitamin B6 (40 mg BD)'. Women were shown how to apply pressure on KID21 themselves whenever they felt nausea and vomiting. | |
| Outcomes | Intensity of nausea using 10 cm VAS, frequency of vomiting was also counted every day. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Block randomisation method in a block of 6. However, the authors later state that 'then gestational age, intensity of nausea and frequency of vomiting were matched in these women'. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Single‐blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 5 did not complete the trial (3 in treatment group, 2 in placebo group). |
| Selective reporting (reporting bias) | Low risk | Only reports medians (and IQRs) for main outcomes. |
| Other bias | Low risk | None apparent. |
Rosen 2003.
| Methods | RCT. | |
| Participants | 230 pregnant women with symptoms of mild to severe nausea and vomiting between 6 and 12 weeks' gestation. | |
| Interventions | Nerve stimulation therapy at the P6 acupuncture point, via a wristband. Placebo: identical but non‐stimulating device. |
|
| Outcomes | Primary outcomes ‐ assessment of nausea and vomiting, self‐recorded symptoms according to the Rhodes Index of Nausea, Vomiting and Retching; data collected on 12 days of the 21 day study, days 1‐7, 9, 11, 13, 17 and 21. Secondary outcomes ‐ weight gain or loss, change in urinary ketones and specific gravity and medication use. |
|
| Notes | Some results (changes in scores over time) in graphical form only. Includes participants with mild to severe symptoms; does not present result separately for each group. Miller 2001 presents results for participants with severe symptoms only (73 of the 193 total). De Veciana 2001 [abstract] reports mild/moderate vs severe‐ not reported in Rosen 2003 [main/only full paper]. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated list. |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered opaque, sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Single‐blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 187 women completed the trial; ‐ 43 patients did not complete the study (18.6%), 22 in treatment group and 21 in the control group. Patients who withdrew were more likely to be multiparous and to have ketonuria. 3 patients from each group withdrew due to adverse events, only 1 attributable to the device. Patients were excluded if they completed fewer than 9 form sets (from total of 23). 4 patients in the treatment group and 1 patient in the control group were "non‐compliant". |
| Selective reporting (reporting bias) | Unclear risk | Results not reported by subgroup (based on severity) in the full paper available for this study. |
| Other bias | Unclear risk | Women were free to take other medication which may have had a bearing on outcomes; without information on what other medication women were using, it is difficult to interpret these data. |
Saberi 2014.
| Methods | RCT. | |
| Participants | 159 women with mild to moderate NVP up to 16 weeks' gestation. | |
| Interventions | Acupressure versus ginger versus control; 7 day study, no participants received any intervention for first 3 days, from intervention began on day 4 for acupressure and ginger groups. Acupressure on the Neiguan point was self‐administered using sea‐band and trained to use it continuously for four days (except when bathing). Women in the ginger group received 12 250 mg ginger capsules and were asked to take 3 per day for 4 days. | |
| Outcomes | Symptoms measured by Rhodes Index of nausea and vomiting. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Table of random numbers. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible with different interventions. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 16 participants were lost to follow‐up: 3 from ginger group, 5 from acupressure group and 8 from control group and all are accounted for. |
| Selective reporting (reporting bias) | Low risk | Results all reported. |
| Other bias | Low risk | None apparent. |
Sahakian 1991.
| Methods | Randomised, double‐blind placebo‐controlled study. | |
| Participants | 74 pregnant women consented to participate; 59 women completed the protocol. | |
| Interventions | Treatment group: vitamin B6 ‐ 25 mg tablets every 8 hours for 72 hours. Placebo: identical appearing tablets to be taken using the same regimen. |
|
| Outcomes | Severity of nausea: marked on 10 cm unmarked VAS: 0 as no nausea and 10 as worst possible nausea; recorded by women 4 times daily (am, noon, pm, bedtime) for the 3 days of treatment. Number of episodes of emesis per 24 hours recorded daily for 3 days. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised by a table of numbers. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | High risk | 20.2% dropout rate high, not clear which group attrition was in. |
| Selective reporting (reporting bias) | High risk | After data collection but before data analysis, the authors say that they arbitrarily divided the patients into 2 subgroups according to the severity of their nausea ‐ patients with a nausea score of greater than 7 were in the severe nausea group and those with scores less than or equal to 7 were categorised in the mild to moderate subgroup and these 2 groups were then compared. As the results showed that there was a significant improvement in the severe nausea subgroup who received the intervention, bias in the arbitrary post hoc cut‐off for severity subgroup bias cannot be ruled out. Unclear reporting ‐ average of averages, mean change from baseline (standard error of the difference in the means) etc. |
| Other bias | Low risk | None apparent. |
Smith 2002.
| Methods | RCT. | |
| Participants | 593 women less than 14 weeks' gestation with symptoms of nausea or vomiting. | |
| Interventions | Traditional acupuncture group (traditional diagnosis and then acupuncture to selected points). P6 acupuncture group (Pericardium point on wrist only). Sham acupuncture group (to points near true points). No acupuncture (control) group (general advice and phoned and asked about their well‐being). The authors state that to reduce disappointment when women were allocated to the control group, a standardised information sheet was made available about advice on diet, lifestyle and the use of vitamin B6 during the 4‐week study period. Not stated if all women got this advice (including about vitamin B6). Treatment was administered weekly for 4 weeks from all 3 acupuncture groups. Very detailed descriptions given. |
|
| Outcomes | Primary outcomes: nausea, vomiting, dry retching at days 7, 14, 21 and 26 (measured by the Rhodes Index of Nausea and Vomiting Form 2) and health status on days 1, 14 and 28 (measured by MOS 36 Short Form Health Survey (SF36)). Pregnancy outcomes: perinatal outcome, congenital abnormalities, pregnancy complications and infant outcomes. |
|
| Notes | Related 2 articles report pregnancy outcomes and placebo response and effect of time and related abstract reports women's experiences of nausea (data collected prior to randomisation from 253 women). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation sequence in variable balanced blocks. |
| Allocation concealment (selection bias) | Low risk | Centralised, external telephone randomisation service. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Single‐blinded; participants blinded. Three hundred and eighty (85%) women guessed which study group they were allocated to, but eight women were unable to guess. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | High risk | 24% attrition by week 4; number of forms (nausea and vomiting and SF36) not completed and number of pregnancy losses per group stated described in detail. |
| Selective reporting (reporting bias) | High risk | Many results reported (mean differences not reported). |
| Other bias | Unclear risk | Vitamin B6 advice given to control group not clear whether to others also. |
Smith 2004.
| Methods | Randomised controlled equivalence trial. | |
| Participants | 291 women with nausea or vomiting, less than 16 weeks' pregnant. | |
| Interventions | Ginger 1.05 g daily (1 capsule of ginger 350 mg 3 times a day). Vitamin B6 daily (1 capsule vitamin B6 25 mg 3 times a day). Treatment was for 3 weeks to test whether ginger and vitamin B6 were equivalent in treating symptoms. |
|
| Outcomes | Equivalence and examined any change in nausea and vomiting scores, measured at days 7, 14 and 21, measured using the Rhodes Index of Nausea and Vomiting Form 2. They recorded baseline for 3 days before randomisation. Health status measured using the MOS 36 Short Form Health Survey, recorded at baseline and day 21. Secondary outcomes: occurrence of any side effects and adverse pregnancy outcomes. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Women were randomly assigned by logging on to the service at a Trials Unit; the computer‐generated randomisation schedule used balanced variable blocks and was prepared by a researcher not involved in the trial. |
| Allocation concealment (selection bias) | Low risk | Centralised system as above, capsules contained in opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Single‐blinded. Data on blinding were available from 138 women (47%); of these, 55 women (40%) reported they were unsure to which group they were allocated. Among the 83 women who gave an opinion, 76% of women who thought they were taking ginger were in the ginger group, compared to 65% of women who thought they were taking vitamin B6 and were allocated to the vitamin B6 group (p.001). |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | Loss to follow‐up in ginger group (n = 146) was 26 and vitamin B6 group (n = 145) was 30; total attrition of 56 (from 291, 19.2%) by day 21. |
| Selective reporting (reporting bias) | Low risk | Does not appear to be any. |
| Other bias | Low risk | None apparent. |
Sripramote 2003.
| Methods | Double‐blind RCT. | |
| Participants | 138 women with NVP at or before 16 weeks' gestation. | |
| Interventions | Ginger 500 mg orally (1 capsule) 3 times daily for 3 days. Vitamin B6 10 mg daily (1 capsule), identical to ginger capsule 3 times daily for 3 days (used as a positive control for ethical reasons). |
|
| Outcomes | Primary outcomes: improvement in nausea symptoms, measured using 10 cm VAS (0 as no nausea to 10 as nausea as bad as it could be). Number of vomiting episodes also recorded. Other secondary outcomes: occurrence of side effects such as drowsiness, palpitations, heartburn and mouth dryness. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A pharmacist not responsible for patient care used a table of random numbers to prepare the treatment assignment by randomisation with a block of 4 to receive ginger or vitamin B6. |
| Allocation concealment (selection bias) | Low risk | The treatment code was concealed by placing the patient's assignment in sequence in sealed opaque envelopes that were drawn in ascending consecutive order. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 4 cases in the ginger and 6 cases in the vitamin B6 group did not return for follow up; 64 evaluable in each group. |
| Selective reporting (reporting bias) | Low risk | No selective reporting apparent. |
| Other bias | Low risk | None apparent. |
Vutyavanich 1995.
| Methods | Randomised double‐blind placebo‐controlled trial. | |
| Participants | 342 pregnant women at </= 17 weeks' gestation. | |
| Interventions | Oral pyridoxine (vitamin B6) received 20 10 mg tablets to be taken every 8 hours (6‐8 am, 2‐4 pm, 10 pm‐12 md) for 5 days. Placebo: identical‐looking tablets to be taken in the same regime. |
|
| Outcomes | Primary outcome: change in the secondary outcome severity of nausea; measured in a VAS in centimetres (10 cm 0 as no nausea to 10 as nausea as bad as it could be). Average daily nausea scores calculated and then mean nausea score over 5 days. Secondary outcome: change in the number of vomiting episodes. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were then randomised into 2 groups by a table of random numbers. |
| Allocation concealment (selection bias) | Low risk | A list that revealed drug codes was kept by the research assistant and was not accessible to the physicians. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All included in analysis except 6 who did not return for follow‐up (2 in placebo group, 4 in treatment group). |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Other bias | Low risk | No other sources of bias apparent. |
Vutyavanich 2001.
| Methods | Randomised double‐masked placebo‐controlled trial. | |
| Participants | 70 women with NVP before 17 weeks' gestation (88 eligible for inclusion, 70 agreed to participate). | |
| Interventions | Ginger 1 g daily orally (250 mg capsules 4 times per day, 3 after meals and 1 before bed); capsules prepared from ginger roots (preparation described). Placebo ‐ identical capsules. Treatment was for 1 week. |
|
| Outcomes | Primary outcome: improvement in nausea symptoms. Severity of nausea recorded a 10 cm VAS 0 as no nausea, 10 as nausea as bad as could be; twice daily (noon and evening) for 4 days. Average daily scores and mean score over 4 days calculated. Number of vomiting episodes daily recorded. At follow‐up 1 week after treatment overall severity was measured using a 5‐point Likert scale (much worse, worse, same, better, much better). Occurrence of side effects and adverse effects on pregnancy outcomes also recorded: such as abortion, preterm birth, congenital anomaly, perinatal death and mode of delivery. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A research nurse who was not responsible for patient care used a table of random numbers to prepare the treatment assignment. |
| Allocation concealment (selection bias) | Low risk | The treatment codes were kept in sequence in a sealed black envelope that could not be read through. As each participant entered the trial, she received the next envelope in the sequence which determined her assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | Low number of women lost to follow‐up (3, all in placebo group, included in the analysis, assuming symptom relief equal to the best improvement in the placebo group). |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Other bias | Low risk | No other sources of bias identified. |
Werntoft 2001.
| Methods | Randomised placebo‐controlled pilot study. | |
| Participants | Pregnant women with normal pregnancy and NVP. Results presented for 60 women ‐ 80 envelopes had been distributed by the time 20 women in each group, totally 60 women or 75% had returned the envelopes (12 of the 20 explained, 8 missing, unknown group). No clear gestational criteria set, 1 woman after 6 weeks', 1 after 16 weeks' gestation and most (n = 34) entered the study after 9‐11 weeks' gestation; there was a statistically significant difference in mean gestational age by group (control group highest). |
|
| Interventions | Acupressure at the P6 (Neiguan) point, using wristbands with a button; worn daily for 2 weeks, only removing it when showering. Acupressure at a placebo point, wristband with a button, applied at upper side of wrist; worn daily for 2 weeks. Control group ‐ no acupressure. |
|
| Outcomes | 100 mm VAS with anchors at each end to indicate the extremes of the sensation under study (no nausea to extreme nausea). Recorded before treatment, on day 1, after 3 days, after 6 days and after 14 days. Incidence of vomiting also reported ‐ not described as an outcome of interest. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Only description: women drew an envelope from a box, envelopes had the same appearance but different contents. |
| Allocation concealment (selection bias) | Unclear risk | Only description: women drew an envelope from a box, envelopes had the same appearance but different contents. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Women did not open the envelope until they got home; blinding possible only if in 1 of 2 acupressure (P6 or placebo) groups; this then presumes no prior knowledge of acupressure (not stated). Blinding not possible for control (no treatment) group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | High risk | Study stopped when 20 completed questionnaires per group were received ‐ states about 80 envelopes were given out ‐ not clear how many per group were given out. From the 20 not completed, 12 are explained: 6 questionnaires from the P6 and placebo groups were excluded due to incompleteness, 4 women found the wristband too tight to use and 2 women had miscarriages. 8 women did not respond and it was not possible to identify which group they belonged to (implies did not know how many in each group were given out). |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Other bias | High risk | It was stated that approximately 80 women were randomised, but the study was ended when 20 women in each of three groups had returned their data collection forms. |
Wibowo 2012.
| Methods | Experimental study. | |
| Participants | 60 pregnant women experiencing NVP prior to 12th week gestation. A further 60 women were not given any treatment (30 who had experienced NVP and 30 who had not). | |
| Interventions | Vitamin B6 10 mg vs vitamin B6 1.28 mg vitamin B6 (pyridoxine hydrochloride) (named high or low dose supplementation), daily for 2 weeks. It was mixed with milk powder, women were asked to take 1 glass containing 2 spoonfuls (or 40 g) of powdered milk twice per day, 1 in the morning and the other at night. | |
| Outcomes | Severity of nausea and vomiting measured by PUQE scoring system (measured at baseline and end of study. unclear if measured between those points). Secondary outcomes: plasma concentration of vitamin B6, vitamin B6 concentration to plasma protein concentration, plasma concentration of serotonin, dopamine, unconjugated estriol and ghrelin. Measured after 2 weeks of treatment. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A computer‐generated random number sequence was drawn up by an independent third party who used the SPSS package. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Investigator blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All participants accounted for; no dropouts. |
| Selective reporting (reporting bias) | High risk | Only baseline and end results reported, unclear if PUQE completed between start and end points. |
| Other bias | Low risk | None apparent. |
Willetts 2003.
| Methods | Double‐blind randomised placebo‐controlled trial. | |
| Participants | 120 pregnant women less than 20 weeks' gestation who had experienced morning sickness for at least 1 week with no relief through dietary changes. | |
| Interventions | 125 mg ginger extract (EV.EXT35, equivalent to 1.5 g dried ginger). Placebo, containing soya bean oil in identical wax‐sealed capsules. 4 times/day (8 am, 12 noon, 4 pm, 8 pm) 4 days. |
|
| Outcomes | Primary outcomes: nausea experience. Secondary outcomes: other 8 scores. Nausea, vomiting, retching as measured by the Rhodes Index of Nausea, Vomiting and Retching (RINVR) (8‐item 5‐point Likert‐type tool, measuring frequent, duration and distress caused by symptoms). Recorded 1 hour after capsule was taken, for baseline day and 4 days of treatment. Side effects and adverse events also reported. |
|
| Notes | Eurovita funded the study, generated the allocation sequence and manufactured the ginger extract. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The random allocation sequence was generated by Eurovita Pty Ltd Denmark using random blocks of 6 and was placed in sealed envelopes and posted to the researchers. |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants, those administering the treatment and those assessing the outcomes were all blinded to the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | 21 women (17.5%) excluded from final analysis due to insufficient data: 12 for adverse events (details given) and 9 for 'non‐compliance'. |
| Selective reporting (reporting bias) | High risk | Mostly report the primary outcome (nausea experience), little reported on vomiting and retching. Results displayed in graphs only, no raw (usable) data. |
| Other bias | Unclear risk | Stated in Discussion that treatment continued for ginger group for 8 days and placebo took ginger for 4 days and all were given 2 weeks' supply following the end of the trial. Only the data for 4 days were analysed, hence the findings of the follow‐up assessment (for the 81 women who completed the main study) should be viewed with caution. No direct attempt can be made to infer cause or association between the findings and the use of ginger over the 8‐day period of the principal study. |
Yavari 2014.
| Methods | Randomised clinical trial. | |
| Participants | 100 pregnant women of gestation 6‐16 weeks, having mild to moderate nausea and vomiting (PUQE score between 3 and 12). | |
| Interventions | Lemon inhaler aromatherapy (when nausea experienced 2 drops placed on cotton and held 3 cm under nose) vs placebo (normal saline). Participants were advised to take 3 slow breaths and if necessary repeat it after 5 minutes. Study duration of 4 days of intervention. The lemon oil was prepared from lemon peel and in solvent distillation method with 10 cc added to almond oil as a carrier oil. The placebo oil the colour of carrots was used with almond oil carrier oil. | |
| Outcomes | Severity of nausea and vomiting using PUQE‐24 daily during 4 days of intervention and at the end of the intervention; side effects; satisfaction. | |
| Notes | Both groups were asked to follow the nutritional advice and lifestyle recommendations. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computerised random number table. |
| Allocation concealment (selection bias) | Low risk | Dark and similar packaged containers sequentially numbered from 1 to 100 executed by a person not involved in the trial. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Similar bottles. Possibility of lack of lemon aroma detected by placebo group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants self‐reported outcomes. |
| Incomplete outcome data (attrition bias) Change in grade of nausea or vomiting at second visit compared to first | Low risk | All participants accounted for. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported. |
| Other bias | Low risk | None. |
IM: intramuscular IQR: interquartile range ITT: intention‐to‐treat NVP: nausea and vomiting of pregnancy PUQE: Pregnancy‐Unique Quantification of Emesis and Nausea RCT: randomised controlled trial SD: standard deviation VAS: visual analogue scale vs: versus
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Anjum 2002 | Double‐blind cross‐over placebo‐controlled study (though only abstract available, unable to source full text, requested from editor). |
| Baum 1963 | Quasi‐randomised, alternate allocation of patients to groups. |
| Bayreuther 1994 | Cross‐over design. |
| Can Gurkan 2008 | Planned as a randomised study, but not carried out as planned (patients on each day placed in same group). |
| Cartwright 1951 | Cross‐over design. |
| Conklin 1958 | Not randomised, patients "arbitrarily allocated" to groups. |
| De Aloysio 1992 | Cross‐over design. |
| Diggory 1962 | Quasi‐randomised "each patient in sequence was allocated"; control group reallocated if not improving. |
| Dundee 1988 | Not an RCT; women allocated to groups by day of the week; non‐responders replaced in treatment group. |
| Evans 1993 | Cross‐over design. |
| Ferruti 1982 | This is a study of hypocorticalism in pregnancy. |
| Fitzgerald 1955 | Not an RCT; alternate allocation of patients. |
| Heazell 2006 | Severe symptoms, in‐patient; hyperemesis gravidarum implied (severe symptoms plus ketonuria). |
| Hyde 1989 | Cross‐over design. |
| Kadan 2009 | Hyperemesis gravidarum as specified condition of participants (RCT, with cross‐over if first drug allocated not effective: thiamine 100 mg IV or promethazine 25 mg IV; started February 2009, trial registry record only, no results at November 2013). |
| King 1955 | Type of cross‐over design. |
| Koren 2004 | Pre‐emptive treatment; not treating symptoms; for severe nausea and vomiting or hyperemesis gravidarum. |
| Koren 2006 | Pre‐emptive treatment; not treating symptoms; for severe nausea and vomiting or hyperemesis gravidarum. Ongoing at 2015. |
| Lask 1953 | Not an RCT. |
| Liu 2014 | Quasi‐experimental; allocation based on registration number and prenatal visit date; comparison of professional support versus routine nursing care. |
| Luz 1987 | No data available; this is a communication of a planned trial ‐ a search identified no further publications from this study. |
| McCarthy 2014 | Trial record (Higgins 2009). Hyperemesis gravidarum: inclusion criteria: ongoing viable intrauterine pregnancy/ pregnancies < 22 weeks' gestation; persistent vomiting (> x 3 episodes/24 hours) not attributable to other causes; severe nausea not attributable to other causes. Dehydration diagnosed by the presence of ketonuria. Electrolyte imbalance not attributable to other causes. |
| Mehrolhasani 2012 | Hyperemesis gravidarum (clinical diagnosis, dehydration); comparison of intramuscular demitron versus promethazine. |
| Pasha 2010 | Trial record only, but appears to be HG based on inclusion criteria: 'symptoms of vomiting for more than 3 times per day, or weight loss more than 3 kilograms or positive urine ketones'. No response from author in August 2013. |
| Reyhani 2013 | States RCT but single arm trial of boiled ground Achiillea milleform, no control group. No results available in abstract. |
| Shahbazzadegan 2006 | Single‐arm study of acupressure using wristband, no control group. Trial record available only at July 2013, no response from author. |
| Steele 2001 | Quasi‐experimental design post‐test only and post‐test repeated measure. |
| Wheatley 1977 | Cross‐over design. |
| Winters 1961 | Quasi randomised trial ‐ "test material and placebo were strictly alternated". |
HG: hyperemesis gravidarum IV: intravenous RCT: randomised controlled trial
Characteristics of studies awaiting assessment [ordered by study ID]
Abedian 2014.
| Methods | RCT. |
| Participants | 60 pregnant women experiencing mild nausea and vomiting in the first half of pregnancy. |
| Interventions | Telephone social support twice a week for a period of 4 weeks versus routine care. Each phone conversation lasted around 15‐20 minutes and dietary and lifestyle changes during pregnancy, as well as ways to reduce fatigue and improve psycho‐emotional status, were discussed. |
| Outcomes | Nausea and vomiting using PUQE score; stress and perceived social support, using the Multidimensional Scale of Perceived Social Support, and VAS for stress. |
| Notes | Abstracts only in English, unable to translate full article from Farsi (forwarded by authors) for this update. Authors report a statistically significant difference in severity of nausea and vomiting in the experimental group before and after intervention (P < 0.001) but not in the control group (P = 0.272). They also report that social support score at the beginning of the study was significantly different from that at the end of the study in both groups (P = 0.036). |
Adamczak 2007.
| Methods | Prospective randomised trial. |
| Participants | 110 pregnant women with gestation of 8 to 14 weeks. |
| Interventions | Solumedrol dose pack (tapered) versus phenergan. |
| Outcomes | Weight, number of episodes of emesis per day, pregnancy outcome. |
| Notes | The authors report that the solumedrol group had significantly fewer emesis episodes that the phenergan group on days 3, 7, 14. Abstract only; no full text reference/article retrieved; unable to contact authors. Insufficient detail to include this study. Given the outcomes measured above, it is possible that this was a study of hyperemesis gravidarum, and it would be excluded if so. |
Babaee 2010.
| Methods | Not stated. "Two hundred pregnant at > [sic] 17 weeks gestational age were selected. For one (case group) 20 mg pyridoxine was used (5 days tds) and for another group placebo was used with the same process." |
| Participants | 200 women > [sic] 17 weeks' gestational age were selected. |
| Interventions | Pyridoxine 20 mg three times daily for 5 days vs placebo. |
| Outcomes | Nausea (not stated how measured), vomiting episodes. |
| Notes | The authors report that Pyridoxine 20 mg three times daily for 4 days [sic] relieved morning sickness. Abstract only; no full text reference/article retrieved; unable to contact authors. Unclear if this was a randomised study based on insufficient information. |
Hsu 2003.
| Methods | Prospective double‐blinded RCT. |
| Participants | 77 pregnant women attending the ED. |
| Interventions | P6 acupressure versus sham acupressure, via a wristband. |
| Outcomes | Nausea severity (using the McGill Nausea Questionnaire), measured at baseline, 30 and 60 minutes. Subsequent anti‐emetic administration, length of ED stay. |
| Notes | The authors report that no differences between groups were reported at any time point. Abstract only ‐ no full text reference/article retrieved; unable to contact authors. Insufficient detail to include this study. |
Mamo 1995.
| Methods | Prospective randomised trial. |
| Participants | 38 pregnant women in first trimester presenting with severe pregnancy vomiting (not stated if hyperemesis gravidarum); title of abstract states "early pregnancy nausea and vomiting". |
| Interventions | Acupressure via sea‐band device on both wrists versus control (counselled and dietary advice). |
| Outcomes | Anti‐emetic drug use, hospitalisation. |
| Notes | The authors only report higher levels of anti‐emetic medication usage for the control group (37%) than the acupressure group (11%) and that there was no significant difference in hospitalisation. However they do not state the denominators for the groups. Abstract only ‐ no full text reference/article retrieved; unable to contact authors. Insufficient detail to include this study. |
Narenji 2014.
| Methods | RCT. |
| Participants | 100 pregnant women. |
| Interventions | Ginger syrup versus vitamin B6. Trial record states: 'ginger powder and fresh root of ginger and vitamin B6'; article title states 'Ginger fresh root versus vitamin B'. |
| Outcomes | Rate of nausea and number of episodes of vomiting, measurement instrument not stated. |
| Notes | Incomplete results in abstract available in English (e.g. number of participants per group); unable to translate from Farsi for this update.Author emailed March 2015. |
Paridokht 2010.
| Methods | Not stated. |
| Participants | 200 pregnant women >[sic] 17 weeks' gestational age. |
| Interventions | Pyridoxine 20 mg three times daily for 5 days. |
| Outcomes | Nausea and vomiting. |
| Notes | No further information available; Poster at conference; identical abstract (including typographical errors) to Babaee 2010. |
Smith 1991.
| Methods | Not stated. |
| Participants | Not stated. |
| Interventions | Acupressure. |
| Outcomes | Nausea and vomiting (not details available). |
| Notes | Masters Abstracts International (from CAM field Register). |
ED: emergency department PUQE: Pregnancy‐Unique Quantification of Emesis and Nausea RCT: randomised controlled trial tds: three times daily VAS: visual analogue scale vs: versus
Characteristics of ongoing studies [ordered by study ID]
Dehkordi 2013.
| Trial name or title | Comparison of 'Cydonia Oblonga' fruit product with B6 on nausea and vomiting in pregnancy. |
| Methods | RCT, not blinded. |
| Participants | 60 pregnant women 6‐14 weeks' gestation. |
| Interventions | Syrup of Cydonia oblonga (quince) fruit 1 table spoon 3 times daily before meals for 1 week vs vitamin B6 20 mg tablet 3 times daily before meals for 1 week. |
| Outcomes | Nausea, vomiting, retching, measured by PUQE and VAS. |
| Starting date | Recruitment start date: 19/02/2013; study ongoing; expected end date for recruitment August 2013. No response to email requesting results in March 2015. |
| Contact information | Dr Efat Jafari Dehordi, Faculty of Traditional Medicine, Tehran University of Medical Sciences, Iran e‐jafarid@razi.tums.ac.ir |
| Notes | IRCT registration number: IRCT2012081110559N1 |
Faramarzi 2013.
| Trial name or title | The comparison of effectiveness of supportive psychotherapy and pharmacotherapy with ondansetron. |
| Methods | RCT. |
| Participants | 90 pregnant women in the first trimester with mild to moderate nausea/ vomiting. |
| Interventions | Ondansetron 4 mg 3 times daily for 4 weeks vs psychotherapy (psychology once weekly) for 4 weeks vs control group. |
| Outcomes | Nausea and vomiting, using 'Rodesh' nausea/vomiting scale; hyperemesis gravidarum (secondary outcome measure). |
| Starting date | Trial registered April 2013; recruitment stated as starting: 01/02/2013 expected recruitment end date 23/12/2014. No response to email requesting results in March 2015. |
| Contact information | Mahbobeh Faramarzi, Babol University of Medical Sciences, Mazanderan, Iran mahbob330@yahoo.com |
| Notes | IRCT registration number: IRCT201304035931N2. |
Farhadifar 2011.
| Trial name or title | Comparing the effects of ginger and metoclopramide in the treatment of pregnancy nausea. |
| Methods | Randomised double‐blind controlled trial. |
| Participants | 68 pregnant women (gestation not specified). |
| Interventions | Ginger 200 mg 3 times daily for 5 days vs Metoclopramid 10 mg three times daily for 5 days vs placebo. |
| Outcomes | Nausea and vomiting measured using Rhodes Index daily for 5 days. |
| Starting date | 23 August 2010. Trial registered June 2011; No response to email requesting results in March 2015. |
| Contact information | Fariba Farhadifar, Kurdistan UNiversity of Medical Sciences, Islamic Republic of Iran. Email: fariba.farhadifar@muk.ac.ir |
| Notes | IRCT registration number: IRCT201306082324N12. |
Keshavarz 2014.
| Trial name or title | Comparison [of] the effect of Lavender and mint oil on nausea, vomiting and anxiety in pregnant women. |
| Methods | RCT. |
| Participants | Pregnant women 6 to 16 weeks' gestation with mild to moderate nausea and vomiting; single pregnancy with a live and healthy fetus according to ultrasound. |
| Interventions | Participants in 2 intervention groups drop lavender or peppermint oil (made by Barij Company) on a piece of cotton pad and will attach to their dress collar within 20 cm distance from nose and they will breathe normally for 20 minutes. This process continues 2 times a day for 1 week. The control group does the same process with placebo. |
| Outcomes | Nausea, vomiting and anxiety. 8‐question Rhodes Index and State Anxiety questionnaire. |
| Starting date | Recruitment start date: June 2014. Confirmed recruitment ongoing in February 2015. |
| Contact information | Azam Amzajerdi. Azamamzajerdi@yahoo.com |
| Notes | IRCT registration number: IRCT201306082324N12. |
Koren 2014.
| Trial name or title | A multicenter trial of the efficacy and safety of Diclegis for nausea and vomiting of pregnancy in pregnant adolescents. |
| Methods | Double‐blind multi‐centre RCT. |
| Participants | Eligible participants are those between 12 and 17 years of age, pregnant with a gestational age of 7 to 15 weeks + 0 days, suffering from NVP, with a PUQE score ≥ 6, and who have not responded to conservative management consisting of dietary/lifestyle advice according to the 2004 American College of Obstetrics and Gynecology (ACOG) Practice Bulletin. |
| Interventions | Participants will be randomised to receive Diclegis or placebo. On day 1, all participants will take 2 tablets of study drug at bedtime. On days 2 to 14, participants will take 2 tablets of study drug at bedtime. The minimum dosage will be 2 tablets daily at bedtime, increasing, when indicated, to the maximal dosage of 4 tablets per day on days 3 to 14. |
| Outcomes | NVP severity from baseline to day 15, using the change in PUQE and Global Assessment of Well‐being scores. |
| Starting date | February 2014. Email to authors confirmed recruitment ongoing in February 2015. |
| Contact information | Hoang Nguyen. hoang.nguyen@premier‐research.com |
| Notes | NCT02045901. |
Ozgoli 2011.
| Trial name or title | Study of cardamom powder effect on the severity of nausea and vomiting in pregnant women referred to health centres in Chalus city 1389‐90. |
| Methods | Randomised double‐blind study. |
| Participants | 120 women with 'mild hyperemesis gravidarum', gestation 6‐22 weeks (the researcher has confirmed that only women less than 20 weeks ultimately took part). |
| Interventions | Cardamom powder capsules 500 mg 3 times per day orally for 4 days vs placebo capsules containing 500 mg lactose 3 times per day orally for 4 days. |
| Outcomes | Severity of nausea and vomiting, using modified PUQE score. |
| Starting date | 22 June 2011. |
| Contact information | Gity Ozgoli, email: gozgoli@yahoo.com |
| Notes | Gestation of participants 6‐22 weeks stated in Iranian Registry of Clinical Trials record (IRCT201107016928N1). Follow‐up email sent to contact person, the trial is complete but results are not available; the researcher stated that in the study women had gestation only of up to 20 weeks. No further update in March 2015. |
Ozgoli 2014.
| Trial name or title | Determination [of] the effect of inhaled peppermint aroma on the severity of nausea and vomiting of pregnancy in women. |
| Methods | RCT. |
| Participants | 56 pregnant women (28 patients in the intervention group and 28 patients in the control group) aged 18 to 35 years, basic level of nausea and vomiting according to (PUQE) questionnaire before intervention in range mild to moderate (points 12‐3), 6 to 20 weeks of gestational age. |
| Interventions | Women in intervention group at the time of nausea will pour 5 drops of peppermint essential oil on a cotton ball and put it 0.5 centimetre below their nose then will inhale 3 deep breaths through the nose. Aromatherapy in the control group will perform similarly with sweet almond oil. |
| Outcomes | Sevberity of nausea and vomiting; satisfaction with treatment; side effects. |
| Starting date | Recruitment start date: January 2015. Recruitment ongoing at March 2015. |
| Contact information | Gity Ozgoli. g.ozgoli@gmail.com |
| Notes | IRCT registration number: IRCT201412043860N9. |
Safajou 2014.
| Trial name or title | The effect of combined inhaler aromatherapy on nausea and vomiting of pregnancy: a randomised controlled trial. |
| Methods | RCT. |
| Participants | Pregnant women who are 16 to 40 years old, 6 to 16 weeks' gestation; with mild to moderate nausea with or without vomiting (based on 3‐12 PUQE‐24 scores). |
| Interventions | Aromatherapy with combined lemon and peppermint essential oil, participants when feeling nauseated, place 3 drops of solution on the cotton, and keep it in distance of 3 cm of their nose, and then breathe 3 times deeply through the nose; placebo group does the same. |
| Outcomes | Severity of nausea and vomiting of pregnancy using PUQE‐24; side effects. |
| Starting date | Recruitment start date: September 2014. Recruiting until July 2015. |
| Contact information | Farzaneh Safajou. fsafajou@bums.ac.ir |
| Notes | IRCT registration number: IRCT2014062914324N2. |
NVP: nausea and vomiting of pregnancy PUQE: Pregnancy‐Unique Quantification of Emesis and Nausea RCT: randomised controlled trial VAS: visual analogue scale vs: versus
Differences between protocol and review
Methods updated to current Cochrane Pregnancy and Childbirth Group standards.
We did not include a 'Summary of findings' table as we had planned, as there were insufficient comparisons that included multiple studies.
We removed the outcomes, caesarean section and satisfaction with treatment. They appear in earlier updates, but were not specified as outcomes within the methods. It was decided that both outcomes, which had been included as proxies for effectiveness of treatment for symptoms, were unnecessary (2015 update).
Contributions of authors
Anne Matthews: guarantor of the review; co‐ordination of the review; review of articles for inclusion/exclusion; extraction of data; wrote the first draft of the review; finalised the review.
David Haas: review of articles for inclusion/exclusion; extraction of data; review of draft review.
Dónal O'Mathúna: review of articles where inclusion/exclusion or quality criteria were not agreed on by AM and DH; review of draft review; provision of methodological advice.
Therese Dowswell: provision of methodological advice and guidance; review of draft review.
Sources of support
Internal sources
The University of Liverpool, UK.
External sources
-
Health Research Board, Ireland.
Cochrane Fellowship held by Anne Matthews 2007‐9
-
National Institute for Health Research, UK.
TD was supported for the 2010 review by a NIHR NHS Cochrane Collaboration Programme Grant Scheme award for NHS‐prioritised centrally‐managed, pregnancy and childbirth systematic reviews: CPGS02
Declarations of interest
No declarations of interest.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Babaei 2014 {published data only}
- Babaei AH, Foghaha MH. A randomized comparison of vitamin B6 and dimenhydrinate in the treatment of nausea and vomiting in early pregnancy. Iranian Journal of Nursing and Midwifery Research 2014;19(2):199‐202. [PMC free article] [PubMed] [Google Scholar]
Basirat 2009 {published data only}
- Basirat Z, Moghadamnia AA, Kashifard M, Sarifi‐Razavi A. The effect of ginger biscuit on nausea and vomiting in early pregnancy. Acta Medica Iranica 2009;47(1):51‐6. [Google Scholar]
Belluomini 1994 {published data only}
- Belluomini J, Litt RC, Lee KA, Katz M. Acupressure for nausea and vomiting of pregnancy: a randomized, blinded study. Obstetrics & Gynecology 1994;84:245‐8. [PubMed] [Google Scholar]
Biswas 2011 {published data only}
- Biswas SC, Bal R, Kamilya GS, Mukherjee J, Hazra A, Narender S, et al. A single‐masked, randomized, controlled trial of ginger extract in the treatment of nausea and vomiting of pregnancy [abstract]. 49th All India Congress of Obstetrics and Gynaecology; 2006 Jan 6‐9; Cochin, Kerala State, India. 2006:53.
- Biswas SC, Dey R, Kamliya GS, Bal R, Hazra A, Tripathi SK. A single‐masked, randomized, controlled trial of ginger extract in the treatment of nausea and vomiting of pregnancy. Journal International Medical Sciences Academy 2011;24(4):167‐9. [Google Scholar]
Bsat 2003a {published data only}
- Bsat F, Bayer‐Zwirello L, Seubert D, Hoffman D. Randomized study of three common outpatient treatments for nausea and vomiting of pregnancy [abstract]. American Journal of Obstetrics and Gynecology 2001;185(6 Suppl):S181. [Google Scholar]
- Bsat FA, Hoffman DE, Seubert DE. Comparison of three outpatient regimens in the management of nausea and vomiting in pregnancy. Journal of Perinatology 2003;23(7):531‐5. [DOI] [PubMed] [Google Scholar]
Chittumma 2007 {published data only}
- Chittumma P, Kaewkiattikun K, Wiriyasiriwach B. Comparison of the effectiveness of ginger and vitamin B6 for treatment of nausea and vomiting in early pregnancy: a randomized double‐blind controlled trial. Journal of the Medical Association of Thailand 2007;90(1):15‐20. [PubMed] [Google Scholar]
Ensiyeh 2009 {published data only}
- Ensiyeh J, Sakineh MAC. Comparing ginger and vitamin B6 for the treatment of nausea and vomiting in pregnancy: a randomised controlled trial. Midwifery 2009;25(6):649‐53. [DOI] [PubMed] [Google Scholar]
Erez 1971 {published data only}
- Erez S, Schifrin BS, Dirim O. Double‐blind evaluation of hydroxyzine as an antiemetic in pregnancy. Journal of Reproductive Medicine 1971;7:57‐9. [PubMed] [Google Scholar]
Fan 1995 {published data only}
- Fan Y. Observation on the therapeutic effect of moxibustion for treatment of pregnant vomiting. World Journal of Acupuncture and Moxibustion 1995;5(4):31‐3. [Google Scholar]
- Fan YJ, Zhu ML, Fu CF. Clinical observation on the effect of moxibustion for vomiting of pregnancy. Zhongguo zhen jiu // Chinese Acupuncture & Moxibustion 1995; Vol. 15, issue 1:11.
Geiger 1959 {published data only}
- Geiger CJ, Fahrenbach DM, Healey FJ. Bendectin in the treatment of nausea and vomiting in pregnancy. Obstetrics & Gynecology 1959;14:688‐90. [PubMed] [Google Scholar]
Ghahiri 2011 {published data only}
- Ghahiri AA, Abdi F, Mastoo R, Ghasemi M. The effect of ondansetron and metoclopramide in nausea and vomiting of pregnancy. Journal of Isfahan Medical School 2011; Vol. 29, issue 131.
Jamigorn 2007 {published data only}
- Jamigorn M, Phupong V. Acupressure and vitamin B6 to relieve nausea and vomiting in pregnancy: a randomized study. Archives of Gynecology and Obstetrics 2007;276(3):245‐9. [DOI] [PubMed] [Google Scholar]
Keating 2002 {published data only}
- Keating A, Chez RA. Ginger syrup as an antiemetic in early pregnancy. Alternative Therapies in Health & Medicine 2002;8(5):89‐91. [PubMed] [Google Scholar]
Khavandizadeh 2010 {published data only}
- Khavandizadeh AS, Mahfouzi B. Evaluation of the effects of acupressure by sea band on nausea and vomiting in pregnancy. Iranian Journal of Obstetrics, Gynecology and Infertility 2010;13(2):39‐44. [Google Scholar]
Knight 2001 {published data only}
- Knight B, Mudge C, Openshaw S, White A, Hart A. Effect of acupuncture on nausea of pregnancy: a randomized, controlled trial. Obstetrics & Gynecology 2001;97:184‐8. [DOI] [PubMed] [Google Scholar]
Koren 2010 {published data only}
- Costantine MM, Matok I, Chiossi G, Clark S, Miodovnik M, Umans JG, et al. Determinants of adherence to delayed‐release doxylamine and pyridoxine in patients with nausea and vomiting of pregnancy. Therapeutic Drug Monitoring 2012;34(5):569‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koren G, Clark S, Hankins GD, Caritis SN, Miodovnik M, Umans JG, et al. Effectiveness of delayed‐release doxylamine and pyridoxine for nausea and vomiting of pregnancy: a randomized placebo controlled trial. American Journal of Obstetrics and Gynecology 2010;203(6):571.e1‐571.e7. [DOI] [PubMed] [Google Scholar]
- Matok I, Clark S, Caritis S, Miodovnik M, Umans G, Hankins G, et al. Studying the antiemetic effect of vitamin B6 for morning sickness: Pyridoxine and pyridoxal are prodrugs. Journal of Clinical Pharmacology 2014;54(12):1429‐33. [DOI] [PubMed] [Google Scholar]
- Matok I, Umans J, Feghali MN, Clark S, Caritis S, Miodovnik M, et al. Characteristics of women with nausea and vomiting of pregnancy who chose to continue compassionate use of placebo after a randomised trial. Journal of Obstetrics & Gynaecology 2013;33(6):557‐60. [DOI] [PubMed] [Google Scholar]
- Nguyen H. The efficacy of diclectin for nausea and vomiting of pregnancy. ClinicalTrials.gov (http://clinicaltrials.gov/) [accessed 20 February 2008] 2008.
McGuiness 1971 {published data only}
- McGuiness BW, Taylor Binns D. 'Debendox' in pregnancy sickness. Journal of the Royal College of General Practitioners 1971;21:500‐3. [PMC free article] [PubMed] [Google Scholar]
Modares 2012 {published data only}
- Besharat S. Effect of ginger and chamomile on nausea and vomiting in pregnancy. IRCT Iranian Registry of Clinical Trials (www.irct.ir) [accessed 6 December 2010] 2010.
- Modares M, Besharat S, Rahimi Kian F, Besharat S, Mahmoudi M, Salehi Sourmaghi H. Effect of ginger and chamomile capsules on nausea and vomiting in pregnancy. Journal of Gorgan University of Medical Sciences 2012;14(1):46‐51. [Google Scholar]
Mohammadbeigi 2011 {published data only}
- Mohammadbeigi R, Shahgeibi S, Soufizadeh N, Rezaiie M, Farhadifar F. Comparing the effects of ginger and metoclopramide on the treatment of pregnancy nausea. Pakistan Journal of Biological Sciences 2011;14(16):817‐20. [DOI] [PubMed] [Google Scholar]
Newlinds 1964 {published data only}
- Newlinds JS. Nausea and vomiting in pregnancy: a trial of thiethylperazine. Medical Journal of Australia 1964;51:234‐6. [PubMed] [Google Scholar]
Norheim 2001 {published data only}
- Norheim AJ, Pedersen EJ, Fonnebo V, Berge L. Acupressure against morning sickness [Akupressur mot svangerskapskvalme]. Tidsskrift for Den Norske Laegeforening 2001;121(23):2712‐5. [PubMed] [Google Scholar]
- Norheim AJ, Pedersen EJ, Fonnebo V, Berge L. Acupressure treatment of morning sickness in pregnancy A randomised, double‐blind, placebo‐controlled study. Scandinavian Journal of Primary Health Care 2001;19(1):43‐7. [DOI] [PubMed] [Google Scholar]
O'Brien 1996 {published data only}
- O'Brien B, Relyea MJ, Taerum T. Efficacy of P6 acupressure in the treatment of nausea and vomiting during pregnancy. American Journal of Obstetrics and Gynecology 1996;174:708‐15. [DOI] [PubMed] [Google Scholar]
Oliveira 2014 {published data only}
- Capp S, Oliveira L, Carstairs S, You W. Ondansetron versus doxylamine/pyridoxine for treatment of nausea and vomiting in pregnancy: a prospective randomized double‐blind trial. American Journal of Obstetrics and Gynecology 2014;210(1 Suppl):S39. [Google Scholar]
- Oliveira L. Ondansetron vs doxylamine and pyridoxine in treating nausea of pregnancy. ClinicalTrials.gov (http://clinicaltrials.gov) [accessed 29 March 2013] 2013.
- Oliveira LG, Capp SM, You WB, Riffenburgh RH, Carstairs SD. Ondansetron compared with doxylamine and pyridoxine for treatment of nausea in pregnancy: a randomized controlled trial. Obstetrics and Gynecology 2014;124(4):735‐42. [DOI] [PubMed] [Google Scholar]
Ozgoli 2009 {published data only}
- Ozgoli G, Goli M, Simbar M. Effects of ginger capsules on pregnancy, nausea, and vomiting. Journal of Alternative and Complementary Medicine 2009;15(3):243‐6. [DOI] [PubMed] [Google Scholar]
Pasha 2012 {published data only}
- Behmanesh F. Evaluating the effect of super mint oil on nausea & vomiting of pregnancy, Babol, 2009. IRCT Iranian Registry of Clinical Trials (www.irct.ir) [accessed 6 December 2010] 2010.
- Pasha H, Behmanesh F, Mohsenzadeh F, Hajahmadi M, Moghadamnia AA. Study of the effect of mint oil on nausea and vomiting during pregnancy. Iranian Red Crescent Medical Journal 2012;14(11):744‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pongrojpaw 2007a {published data only}
- Pongrojpaw D. A randomized comparison of ginger and dimenhydrinate in the treatment of nausea vomiting in pregnancy. American Journal of Obstetrics and Gynecology 2006;195(6 Suppl 1):S92. [Google Scholar]
- Pongrojpaw D, Somprasit C, Chanthasenanont A. A randomized comparison of ginger and dimenhydrinate in the treatment of nausea and vomiting in pregnancy. Journal of the Medical Association of Thailand 2007;90(9):1703‐9. [PubMed] [Google Scholar]
Price 1964 {published data only}
- Price JJ, Barry MC. A double blind study of fluphenazine with pyridoxine. Pennsylvania Medical Journal 1964;67:37‐40. [PubMed] [Google Scholar]
Puangsricharern 2008 {published data only}
- Puangsricharern A, Mahasukhon S. Effectiveness of auricular acupressure in the treatment of nausea and vomiting in early pregnancy. Journal of the Medical Association of Thailand 2008;91(11):1633‐8. [PubMed] [Google Scholar]
Rad 2012 {published data only}
- Lamyian M. Evaluation of the influence of KID 21(youmen) point acupressure on nausea and vomiting of pregnancy. IRCT: Iranian Register of Clinical Trials (www.irct.ir) [accessed 30 April 2013] 2013.
- Rad MN. Evaluation of the influence of KID 21 (youmen) point acupressure on nausea and vomiting of pregnancy. IRCT Iranian Registry of Clinical Trials (www.irct.ir) [accessed 6 December 2010] 2010.
- Rad MN, Lamyian M, Heshmat R, Jaafarabadi MA, Yazdani S. A randomized clinical trial of the efficacy of KID21 point (Youmen) acupressure on nausea and vomiting of pregnancy. Iranian Red Crescent Medical Journal 2012;14(11):697‐701. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rosen 2003 {published data only}
- Veciana M, Stewart L, Miller H, Slotnick R, Rebarber A, Rosen T. Multicenter randomized controlled trial of nerve stimulation therapy for the relief of nausea and vomiting in pregnancy [abstract]. American Journal of Obstetrics and Gynecology 2001;185(6 Suppl):S182. [DOI] [PubMed] [Google Scholar]
- Miller H, Veciana M, Stewart L, Rebarber A, Rosen T, Slotnick R. A multicenter randomized controlled trial of nerve stimulation therapy: subanalysis of severe nausea and vomiting symptoms [abstract]. American Journal of Obstetrics and Gynecology 2001;185(6 Suppl):S188. [Google Scholar]
- Rosen T, Veciana M, Miller HS, Stewart L, Rebarber A, Slotnick RN. A randomized controlled trial of nerve stimulation for relief of nausea and vomiting in pregnancy. Obstetrics & Gynecology 2003;102(1):129‐35. [DOI] [PubMed] [Google Scholar]
Saberi 2014 {published data only}
- Saberi F. Comparison of acupressure and ginger in the treatment of nausea and vomiting of pregnancy. IRCT: Iranian Register of Clinical Trials (www.irct.ir) [accessed 20 September 2011] 2011.
- Saberi F, Sadat Z, Abedzadeh‐Kalahroudi M, Taebi M. Acupressure and ginger to relieve nausea and vomiting in pregnancy: a randomized study. Iranian Red Crescent Medical Journal 2013;15(9):854‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saberi F, Sadat Z, Abedzadeh‐Kalahroudi M, Taebi M. Effect of ginger on relieving nausea and vomiting in pregnancy: a randomized, placebo‐controlled trial. Nursing and Midwifery Studies 2014;3(1):e11841. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sahakian 1991 {published data only}
- Sahakian V, Rouse D, Sipes S, Rose N, Niebyl J. Vitamin B6 is effective therapy for nausea and vomiting of pregnancy: a randomized, double‐blind placebo‐controlled study. Obstetrics & Gynecology 1991;78:33‐6. [PubMed] [Google Scholar]
- Sahakian V, Rouse DJ, Rose NB, Niebyl JR. Vitamin B6 for nausea and vomiting of pregnancy. American Journal of Obstetrics and Gynecology 1991;164:322. [PubMed] [Google Scholar]
Smith 2002 {published data only}
- Smith C, Crowther C. The placebo response and effect of time in a trial of acupuncture to treat nausea and vomiting in early pregnancy. Complementary Therapies in Medicine 2002;10(4):210‐6. [DOI] [PubMed] [Google Scholar]
- Smith C, Crowther C, Beilby J. Acupuncture to treat nausea and vomiting in early pregnancy: a randomized controlled trial. Birth 2002;29(1):1‐9. [DOI] [PubMed] [Google Scholar]
- Smith C, Crowther C, Beilby J. Pregnancy outcome following women's participation in a randomised controlled trial of acupuncture to treat nausea and vomiting in early pregnancy. Complementary Therapies in Medicine 2002;10:78‐83. [DOI] [PubMed] [Google Scholar]
- Smith C, Crowther C, Beilby J. Women's experiences of nausea and vomiting in early pregnancy. 2nd Annual Congress of the Perinatal Society of Australia & New Zealand; 1998 March 30‐April 4; Alice Springs, Australia. 1998:142.
Smith 2004 {published data only}
- Smith C, Crowther C, Willson K, Hotham N, McMillian V. A randomized controlled trial of ginger to treat nausea and vomiting in pregnancy. Obstetrics & Gynecology 2004;103(4):639‐45. [DOI] [PubMed] [Google Scholar]
- Smith CA, Hotham N, MacMillan V, Crowther CA. Comparison of ginger and vitamin B6 for treating nausea and vomiting in early pregnancy: a randomised controlled trial. Perinatal Society of Australia and New Zealand 7th Annual Congress; 2003 March 9‐12; Tasmania, Australia. 2003:P47.
Sripramote 2003 {published data only}
- Sripramote M, Lekhyananda N. A randomized comparison of ginger and vitamin b6 in the treatment of nausea and vomiting in pregnancy. Journal of the Medical Association of Thailand 2003;86:846‐53. [PubMed] [Google Scholar]
Vutyavanich 1995 {published data only}
- Vutyavanich T, Wongtra‐ngan S, Ruangsri R. Pyridoxine for nausea and vomiting of pregnancy: a randomized, double‐blind, placebo‐controlled trial. American Journal of Obstetrics and Gynecology 1995;173(3 Pt 1):881‐4. [DOI] [PubMed] [Google Scholar]
Vutyavanich 2001 {published data only}
- Kraisarin T, Vutyavanich T. The effectiveness of ginger for the treatment of nausea and vomiting of pregnancy. Thai Journal of Obstetrics and Gynaecology 2000;12(4):340. [Google Scholar]
- Vutyavanich T, Kraisarin T, Ruangsri RA. Ginger for nausea and vomiting in pregnancy: randomized double masked, placebo controlled trial. Obstetrics & Gynecology 2001;97:577‐88. [DOI] [PubMed] [Google Scholar]
Werntoft 2001 {published data only}
- Werntoft E, Dykes AK. Effect of acupressure on nausea and vomiting during pregnancy. Journal of Reproductive Medicine 2001;46(9):835‐9. [PubMed] [Google Scholar]
Wibowo 2012 {published data only}
- Wibowo N. B6 treatment for nausea and vomiting in pregnancy. ClinicalTrials.gov (http://clinicaltrials.gov/) [accessed 4 January 2009] 2009.
- Wibowo N, Purwosunu Y, Sekizawa A, Farina A, Tambunan V, Bardosono S. Vitamin B(6) supplementation in pregnant women with nausea and vomiting. International Journal of Gynaecology and Obstetrics: the Official Organ of the International Federation of Gynaecology and Obstetrics 2012;116(3):206‐10. [DOI] [PubMed] [Google Scholar]
Willetts 2003 {published data only}
- Willetts KE, Ekangaki A, Eden JA. Effect of a ginger extract on pregnancy‐induced nausea: a randomised controlled trial. Australian and New Zealand Journal of Obstetrics and Gynaecology 2003;43:139‐44. [DOI] [PubMed] [Google Scholar]
Yavari 2014 {published data only}
- Safajou F. The effect of lemon inhaler aromatherapy on nausea and vomiting of pregnancy: a randomised controlled trial. IRCT: Iranian Register of Clinical Trials (www.irct.ir) [accessed 30 April 2010] 2010.
- Yavari Kia PY, Safajou F, Shahnazi M, Nazemiyeh H. The effect of lemon inhalation aromatherapy on nausea and vomiting of pregnancy: a double‐blinded, randomized, controlled clinical trial. Iranian Red Crescent Medical Journal 2014;16(3):e14360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yavari Kia PY, Safajou F, Shahnazi M, Nazemiyeh H. The effect of lemon inhalation aromatherapy on nausea and vomiting of pregnancy: double‐blind randomised controlled clinical trial. Author's unpublished copy of article for submission to a journal 2013. [DOI] [PMC free article] [PubMed]
References to studies excluded from this review
Anjum 2002 {published data only}
- Anjum N, Rizvi MIS, Ayub Z, Baig MA, Hameed A. Control of early morning sickness of pregnancy by acupressure technique. Annals of Abbasi Shaheed Hospital & Karachi Medical & Dental College 2002;7(2):369‐73. [Google Scholar]
Baum 1963 {published data only}
- Baum G, Boxer EI, Davidson JH, Lawrence N, Lewis JBR, Morgan DJR, et al. Meclozine and pyridoxine in pregnancy sickness. Practitioner 1963;190:251‐3. [Google Scholar]
Bayreuther 1994 {published data only}
- Bayreuther J, Lewith GT, Pickering R. A double‐blind cross‐over study to evaluate the effectiveness of acupressure at pericardium 6 (P6) in the treatment of early morning sickness (EMS). Complementary Therapies in Medicine 1994;2:70‐6. [Google Scholar]
Can Gurkan 2008 {published data only}
- Can Gurkan O, Arslan H. Effect of acupressure on nausea and vomiting during pregnancy. Complementary Therapies in Clinical Practice 2008;14(1):46‐52. [DOI] [PubMed] [Google Scholar]
Cartwright 1951 {published data only}
- Cartwright EW. Dramamine in nausea and vomiting of pregnancy. Western Journal of Surgery 1951;59:216‐34. [PubMed] [Google Scholar]
Conklin 1958 {published data only}
- Conklin FJ, Nesbitt REL. Buclizine hydrochloride for nausea and vomiting of pregnancy. Obstetrics & Gynecology 1958;11:214‐9. [PubMed] [Google Scholar]
De Aloysio 1992 {published data only}
- Aloysio D, Penacchioni P. Morning sickness control in early pregnancy by Neiguan point acupressure. Obstetrics & Gynecology 1992;80:852‐4. [PubMed] [Google Scholar]
Diggory 1962 {published data only}
- Diggory PLC, Tomkinson JS. Nausea and vomiting in pregnancy. A trial of meclozine dihydrochloride with and without pyridoxine. Lancet 1962;2:370‐2. [DOI] [PubMed] [Google Scholar]
Dundee 1988 {published data only}
- Dundee JW, Sourial FBR, Ghaly RG, Bell PF. P6 acupressure reduces morning sickness. Journal of the Royal Society of Medicine 1988;81:456‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Evans 1993 {published data only}
- Evans AT, Samuels SN, Marshall C, Bertolucci LE. Suppression of pregnancy‐induced nausea and vomiting with sensory afferent stimulation. Journal of Reproductive Medicine 1993;38(8):603‐6. [PubMed] [Google Scholar]
Ferruti 1982 {published data only}
- Ferruti MM, Speranza R. Use of the combination of adrenal cortex extract, pyridoxal‐5‐phosphate, cyanocobalamin and ascorbic acid in the treatment of hypocorticism in pregnancy [Italian] [Sulla utilita dell'associazione di estratto corticosurrenale, piridossal‐5‐fosfato, cianocobalamina e acido ascorbico nel trattamento degli stati di ipocorticalismo in gravidanza.]. Minerva Ginecologica 1982;34:619‐23. [PubMed] [Google Scholar]
Fitzgerald 1955 {published data only}
- Fitzgerald JPB. The effect of promethazine in nausea and vomiting of pregnancy. New Zealand Medical Journal 1955;54:215‐8. [PubMed] [Google Scholar]
Heazell 2006 {published data only}
- Heazell A, Thorneycroft J, Walton V, Etherington I. Acupressure for the in‐patient treatment of nausea and vomiting in early pregnancy: a randomized control trial. American Journal of Obstetrics and Gynecology 2006;194(3):815‐20. [DOI] [PubMed] [Google Scholar]
Hyde 1989 {published data only}
- Hyde E. Acupressure therapy for morning sickness. A controlled clinical trial. Journal of Nurse Midwifery 1989;34:171‐8. [DOI] [PubMed] [Google Scholar]
Kadan 2009 {published data only}
- Kadan Y. Does thiamine help vomiting and nausea in pregnancy?. ClinicalTrials.gov (http://clinicaltrials.gov) (accessed 15 July 2013) 2013.
King 1955 {published data only}
- King AG. The treatment of pregnancy nausea with a pill. Obstetrics & Gynecology 1955;6:332‐8. [PubMed] [Google Scholar]
Koren 2004 {published data only}
- Koren G, Maltepe C. Pre‐emptive therapy for severe nausea and vomiting of pregnancy and hyperemesis gravidarum. Journal of Obstetrics and Gynaecology. 2004;24(5):530‐3. [DOI] [PubMed] [Google Scholar]
Koren 2006 {published data only}
- Koren G. Pre‐emptive treatment of severe nausea and vomiting of pregnancy (ongoing trial, February 2015). ClinicalTrials.gov (http://clinicaltrials.gov/) [accessed 21 March 2006] 2006.
- Maltepe C, Koren G. Pre‐emptive treatment of nausea and vomiting of pregnancy: results of a randomised controlled trial. Obstetrics and Gynaecology International 2013;2013:Article no: 809787. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lask 1953 {published data only}
- Lask S. Treatment of nausea and vomiting of pregnancy with antihistamines. British Medical Journal 1953;1:652‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Liu 2014 {published data only}
- Liu MC, Kuo SH, Lin CP, Yang YM, Chou FH, Yang YH. Effects of professional support on nausea, vomiting, and quality of life during early pregnancy. Biological Research for Nursing 2014;16(4):378‐86. [DOI] [PubMed] [Google Scholar]
Luz 1987 {published data only}
- Luz NP, Gonzales MAG. Effect of bromopride on nausea and vomiting during pregnancy. Personal communication 1987.
McCarthy 2014 {published data only}
- Higgins JR. Day care versus inpatient management of nausea and vomiting of pregnancy ‐ D.I.M. trial. Current Controlled Trials (http://controlled‐trials.com/) [accessed 5 January 2009].
- Higgins JR. Randomized controlled trial of day care versus inpatient management of nausea and vomiting of pregnancy. ClinicalTrials.gov (http://clinicaltrials.gov) [accessed 21 May 2013] 2008.
- McCarthy FP, Murphy A, Khashan AS, McElroy B, Spillane N, Marchocki Z, et al. Day care compared with inpatient management of nausea and vomiting of pregnancy: a randomized controlled trial. Obstetrics and Gynecology 2014;124(4):743‐8. [DOI] [PubMed] [Google Scholar]
Mehrolhasani 2012 {published data only}
- Mehrolhasani Y. Comparison of Demitron and promethazine in treatment of hyperemesis gravidarum. IRCT: Iranian Registry of Clinical Trials (www.irct.ir) (accessed 22 July 2013) 2012.
Pasha 2010 {published data only}
- Pasha NG. A comparison of ondansetron vs. metoclopramide for treatment of nausea and vomiting in pregnancy. IRCT Iranian Registry of Clinical Trials (www.irct.ir) (accessed 6 December 2010) 2010.
Reyhani 2013 {published data only}
- Reyhani M, Eskandari M. Evaluation of the Achillea millefolum effect in nausea and vomiting of early pregnancy. Iranian Journal of Pharmaceutical Research 2013;12(Suppl 2):232. [Google Scholar]
Shahbazzadegan 2006 {published data only}
- Ozgoli G, Shahbazzadegan S, Rasaeian N, Alavimajd H. Effect of acupressure with wristband on nausea and vomiting of pregnancy. Journal of Ardabil University of Medical Science 2007;7(3):247‐53. [Google Scholar]
- Shahbazzadegan S. Investigation the trend of pregnancy nausea and vomiting treatment using acupressure wristband. IRCT: Iranian Register of Clinical Trials (http://www.irct.ir) (accessed 30 April 2013) 2006.
Steele 2001 {published data only}
- Steele NM, French J, Gatherer‐Boyles J, Newman S, Leclaire S. Effect of acupressure by sea‐bands on nausea and vomiting of pregnancy. Journal of Obstetric, Gynecologic and Neonatal Nursing 2001;30(1):61‐70. [PubMed] [Google Scholar]
Wheatley 1977 {published data only}
- Wheatley D. Treatment of pregnancy sickness. British Journal of Obstetrics and Gynaecology 1977;84:444‐7. [DOI] [PubMed] [Google Scholar]
Winters 1961 {published data only}
- Winters HS. Antiemetics in nausea and vomiting of pregnancy. Obstetrics & Gynecology 1961;18:753‐6. [PubMed] [Google Scholar]
References to studies awaiting assessment
Abedian 2014 {published data only}
- Abedian Z. The effect of telephone support on health‐related quality of life in women with nausea and vomiting of pregnancy. IRCT: Iranian Register of Clinical Trials (www.irct.ir/) [accessed 19 January 2015] 2014.
Adamczak 2007 {published data only}
- Adamczak J, Kasdaglis J, Rinehart B, Antebi Y, Wolf E, Terrone D. A prospective randomized trial of solumedrol dose pack vs. phenergan for the treatment of symptomatic nausea and vomiting in pregnancy. American Journal of Obstetrics and Gynecology 2007;197(6 Suppl 1):S88, Abstract no: 277. [Google Scholar]
Babaee 2010 {published data only}
- Babaee PAG. Determining the effect of pyridoxine on nausea and vomiting in pregnancy. Journal of Maternal‐Fetal and Neonatal Medicine 2010;23(S1):129. [Google Scholar]
Hsu 2003 {published data only}
- Hsu E, Pei V, Shofer FS, Abbuhl SB. A prospective randomized controlled trial of acupressure vs sham for pregnancy‐related nausea and vomiting in the emergency department. Academic Emergency Medicine 2003;10(5):437. [Google Scholar]
Mamo 1995 {published data only}
- Mamo J, Mamo D, Pace M, Felice D. Evaluation of sea‐band acupressure device for early pregnancy nausea and vomiting. 27th British Congress of Obstetrics And Gynaecology; 1995 July 4‐7; Dublin, Ireland. 1995:283.
Narenji 2014 {published data only}
- Narenji F. Comparison the effects of ginger powder and fresh root of ginger and Vit B6 on nausea and vomiting in pregnancy. IRCT: Iranian Register of Clinical Trials (www.irct.ir/) [accessed 19 January 2015] 2014.
- Narenji F, Delaver M, Rafiei M. Comparison the effects of the ginger fresh root and vitamin B6 on the nausea and vomiting in pregnancy. Iranian Journal of Obstetrics, Gynaecology and Infertility 2012;15(2):39‐43. [Google Scholar]
Paridokht 2010 {published data only}
- Paridokht A, Gholamreza B. Determine effect VB6 on nausea and vomiting of pregnancy. Journal of Maternal‐Fetal and Neonatal Medicine 2010;23(S1):127‐8. [Google Scholar]
Smith 1991 {published data only}
- Smith EA, Smith GL. Acupressure to control nausea and vomiting during pregnancy. Masters Abstracts International 1991; Vol. 29, issue 4:651.
References to ongoing studies
Dehkordi 2013 {published data only}
- Dehkordi EJ. Comparison of "Cydonia Oblonga" fruit product with B6 on nausea and vomiting in pregnancy. IRCT: Iranian Register of Clinical Trials (www.irct.ir) [accessed 30 April 2013] 2013.
Faramarzi 2013 {published data only}
- Faramarzi M. The comparison of effectiveness of supportive psychotherapy and pharmacotherapy with ondansetron to improvement of nausea and vomiting of pregnancy. IRCT: Iranian Register of Clinical Trials (www.irct.ir) [accessed 1 May 2013] 2013.
Farhadifar 2011 {published data only}
Keshavarz 2014 {published data only}
- Keshavarz M. Comparison the effect of Lavender and mint oil on nausea, vomiting and anxiety in pregnant women. IRCT: Iranian Register of Clinical Trials (www.irct.ir/) [accessed 19 January 2015] 2014.
Koren 2014 {published data only}
- Koren G. A multicenter trial of the efficacy and safety of Diclegis for nausea and vomiting of pregnancy in pregnant adolescents. ClinicalTrials.gov (http://clinicaltrials.gov/) [accessed 5 February 2014] 2014.
Ozgoli 2011 {published data only}
- Ozgoli G. Study of Cardamom powder effect on the severity of nausea and vomiting in pregnant women referred to health centers in Chalus city 1389‐90. IRCT: Iranian Register of Clinical Trials (http://www.irct.ir) [accessed 30 April 2013] 2011.
Ozgoli 2014 {published data only}
- Ozgoli G. Determination the effect of inhaled peppermint aroma on the severity of nausea and vomiting of pregnancy in women. IRCT: Iranian Register of Clinical Trials (http://www.irct.ir/) [accessed 19 January 2015] 2014.
Safajou 2014 {published data only}
- Safajou F. The effect of combined inhaler aromatherapy on nausea and vomiting of pregnancy: a randomised controlled trial. IRCT: Iranian Register of Clinical Trials (http://www.irct.ir/) [accessed 19 January 2015].
Additional references
ACOG 2004
- American College of Obstetricians and Gynecologists (ACOG). Nausea and vomiting of pregnancy. ACOG Practice Bulletin 2004; Vol. 52.
Aikins Murphy 1998
- Aikins Murphy P. Alternative therapies for nausea and vomiting of pregnancy. Obstetrics & Gynecology 1998;91(1):149‐55. [DOI] [PubMed] [Google Scholar]
Anderka 2012
- Anderka M, Mitchell AA, Louik C, Werler MM, Hernandez‐Diaz S, Rasmussen SA, et al. Medications used to treat nausea and vomiting of pregnancy and the risk of selected birth defects. Birth defects Research (Part A) 2012;94:22‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
Arsenault 2002
- Arsenault MY, Lane CA. The management of nausea and vomiting in pregnancy (Society of Obstetricians and Gynaecologists Canada: Clinical Practice Guidelines, no. 120). Journal of Obststrics and Gynaecology Canada 2002;24(10):817‐31. [PubMed] [Google Scholar]
Atanackovic 2001
- Atanackovic G, Wolpin J, Koren G. Determinants of the need for hospital care among women with nausea and vomiting of pregnancy. Clinical & Investigative Medicine 2001;24(2):90. [PubMed] [Google Scholar]
Attard 2002
- Attard CL, Kohli MA, Coleman S, Bradley C, Hux M, Atanackovic G, et al. The burden of illness of severe nausea and vomiting of pregnancy in the United States. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S220‐S227. [DOI] [PubMed] [Google Scholar]
Bayles 2007
- Bayles BP. Herbal and other complementary medicine use by Texas midwives. Journal of Midwifery and Women's Health 2007;52(5):473‐8. [DOI] [PubMed] [Google Scholar]
Boelig 2013
- Boelig RC, Berghella V, Kelly AJ, Barton SJ, Edwards SJ. Interventions for treating hyperemesis gravidarum. Cochrane Database of Systematic Reviews 2013, Issue 6. [DOI: 10.1002/14651858.CD010607] [DOI] [PMC free article] [PubMed] [Google Scholar]
Borrelli 2005
- Borrelli F, Capasso R, Aviello G, Pittler MH, Izzo AA. Effectiveness and safety of ginger in the treatment of pregnancy‐induced nausea and vomiting. Obstetrics & Gynecology 2005;105(4):849‐56. [DOI] [PubMed] [Google Scholar]
Brent 2002
- Brent R. Medical, social, and legal implications of treating nausea and vomiting of pregnancy. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S262‐S266. [DOI] [PubMed] [Google Scholar]
Bryer 2005
- Bryer E. A literature review of the effectiveness of ginger in alleviating mild‐to‐moderate nausea and vomiting of pregnancy. Journal of Midwifery and Women's Health 2005;50(1):e1‐e3. [DOI] [PubMed] [Google Scholar]
Bsat 2003b
- Bsat FA, Hoffman DE, Seubert DE. Comparison of three outpatient regimens in the management of nausea and vomiting in pregnancy. Journal of Perinatology 2003;23(7):531‐5. [DOI] [PubMed] [Google Scholar]
Buckwalter 2002
- Buckwalter JG, Simpson SW. Psychological factors in the etiology and treatment of severe nausea and vomiting in pregnancy. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S210‐S214. [DOI] [PubMed] [Google Scholar]
Chan 2011
- Chan RL, Olshan AF, Savitz DA, Herring AH, Daniels JL, Peterson HB, et al. Maternal Influences on nausea and vomiting in early pregnancy. Maternal and Child Health Journal 2011;15(1):122‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chin 2014
- Chin JWS, Gregor S, Persaud N. Re‐analysis of safety data supporting doxylamine use for nausea and vomiting of pregnancy. American Journal of Perinatology 2014;31(8):701‐10. [DOI: 10.1055/s-0033-1358772] [DOI] [PubMed] [Google Scholar]
Chou 2003
- Chou FH, Lin LL, Cooney AT, Walker LO, Riggs MW. Psychosocial factors related to nausea, vomiting, and fatigue in early pregnancy. Journal of Nursing Scholarship 2003;35(2):119‐25. [DOI] [PubMed] [Google Scholar]
Chou 2008
- Chou FH, Avant KC, Kuo SH, Fetzer SJ. Relationships between nausea and vomiting, perceived stress, social support, pregnancy planning, and psychosocial adaptation in a sample of mothers: a questionnaire survey. International Journal of Nursing Studies 2008;45(8):1185‐91. [DOI] [PubMed] [Google Scholar]
Cunningham 2015
- Cunningham K. Ondansetron compared with doxylamine and pyridoxine for treatment of nausea and vomiting in pregnancy: a randomised controlled trial [Letter]. Obstetrics & Gynecology 2015;125(2):490. [DOI] [PubMed] [Google Scholar]
Czeizel 2004
- Czeizel AE, Puho E. Association between severe nausea and vomiting in pregnancy and lower rate of preterm births. Paediatric and Perinatal Epidemiology 2004;18(4):253‐9. [DOI] [PubMed] [Google Scholar]
Dante 2013
- Dante G, Pedrielli G, Annessi E, Facchinetti F. Herb remedies during pregnancy: a systematic review of controlled clinical trials. Journal of Maternal Fetal and Neonatal medicine 2013;26(3):306‐12. [DOI] [PubMed] [Google Scholar]
Davis 2004
- Davis M. Nausea and vomiting of pregnancy: an evidence‐based review. Journal of Perinatal & Neonatal Nursing 2004;18(4):312‐28. [DOI] [PubMed] [Google Scholar]
De Veciana 2001
- Veciana M, Stewart L, Miller H, Slotnick R, Rebarber A, Rosen T. Multicenter randomized controlled trial of nerve stimulation therapy for the relief of nausea and vomiting in pregnancy. American Journal of Obstetrics and Gynecology 2001;185(6 Suppl):S182. [DOI] [PubMed] [Google Scholar]
Ding 2013
- Ding M, Leach M, Bradley H. The effectiveness of ginger in the treatment of pregnancy‐indiced nausea and vomiting: a systematic review. Women and Birth 2013;26(1):e26‐30. [DOI] [PubMed] [Google Scholar]
Einarson 2007
- Einarson TR, Navioz Y, Maltepe C, Einarson A, Koren G. Existence and severity of nausea and vomiting in pregnancy (NVP) with different partners. Journal of Obstetrics and Gynaecology 2007;27(4):360‐2. [DOI] [PubMed] [Google Scholar]
Einarson 2013
- Einarson TR, Piwko C, Koren G. Quantifying the global rates of nausea and vomiting of pregnancy: a meta analysis. Journal of the Population Therapeutics and Clinical Pharmacology [Journal de la Therapeutique des Populations et de la Pharmacologie Clinique] 2012;20(2):e171‐e183. [PubMed] [Google Scholar]
Eliakim 2000
- Eliakim R, Abulafia O, Sherer DM. Hyperemesis gravidarum: a current review. American Journal of Perinatology 2000;17(4):207‐18. [DOI] [PubMed] [Google Scholar]
Ernst 2000
- Ernst E, Pittler MH. Efficacy of ginger for nausea and vomiting: a systematic review of randomized clinical trials. British Journal of Anaesthesia 2000;84(3):367‐71. [DOI] [PubMed] [Google Scholar]
Ernst 2002a
- Ernst E, Schmidt K. Health risks over the Internet: advice offered by "medical herbalists" to a pregnant woman. Wiener Medizinische Wochenschrift 2002;152(7‐8):190‐2. [DOI] [PubMed] [Google Scholar]
Ernst 2002b
- Ernst E. Herbal medicinal products during pregnancy: are they safe?. BJOG: an international journal of obstetrics and gynaecology 2002;109:227‐35. [DOI] [PubMed] [Google Scholar]
Goodwin 2002
- Goodwin TM. Nausea and vomiting of pregnancy: an obstetric syndrome. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S184‐S189. [DOI] [PubMed] [Google Scholar]
GRADEpro 2014 [Computer program]
- McMaster University. GRADEpro. [Computer program on www.gradepro.org]. Version [2014]. McMaster University, 2014.
Hall 2011
- Hall HG, Griffiths DL, McKenna LG. The use of complementary and alternative medicine by pregnant women: a literature review. Midwifery 2011;27(6):817‐24. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jewell 2003b
- Jewell D. Nausea and vomiting in early pregnancy. American Family Physician 2003;68(1):143‐4. [PubMed] [Google Scholar]
King 2009
- King TL, Aikins Murphy P. Evidence‐based approaches to managing nausea and vomiting in early pregnancy. Journal of Midwifery & Women's Health 2009;54(6):430‐44. [DOI] [PubMed] [Google Scholar]
Koch 2002
- Koch KL. Gastrointestinal factors in nausea and vomiting of pregnancy. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S198‐S203. [DOI] [PubMed] [Google Scholar]
Koren 2002a
- Koren G, Levichek Z. The teratogenicity of drugs for nausea and vomiting of pregnancy: perceived versus true risk. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S248‐S252. [DOI] [PubMed] [Google Scholar]
Koren 2002b
- Koren G, Boskovic R, Hard M, Maltepe C, Navioz Y, Einarson A. Motherisk ‐ PUQE (pregnancy‐unique quantification of emesis and nausea) scoring system for nausea and vomiting of pregnancy. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S228‐S231. [DOI] [PubMed] [Google Scholar]
Koren 2005
- Koren G, Piwko C, Ahn E, Boskovic R, Maltepe C, Einarson A. Validation studies of the Pregnancy Unique‐Quantification of Emesis (PUQE) scores. Journal of Obstetrics and Gynaecology 2005;25(3):241‐4. [DOI] [PubMed] [Google Scholar]
Koren 2011
- Koren G, Maltepe C, Gow R. Therapeutic choices for nausea and vomiting of pregnancy: a critical review of a systematic review. Journal of Obstetrics and Gynaecology 2011;33:733–5. [DOI] [PubMed] [Google Scholar]
Koren 2015
- Koren G, Maltepe C, Madjunkova S. Ondansetron compared with doxlamine and pyridoxine for treatment of nausea and vomiting in pregnancy: a randomized controlled trial [Letter]. Obstetrics & Gynecology 2015;125(2):490. [DOI] [PubMed] [Google Scholar]
Kousen 1993
- Kousen M. Treatment of nausea and vomiting in pregnancy. American Family Physician 1993;48(7):1279. [PubMed] [Google Scholar]
Lacasse 2008
- Lacasse A, Rey E, Ferreira E, Morin C, Berard A. Validity of a modified Pregnancy‐Unique Quantification of Emesis and Nausea (PUQE) scoring index to assess severity of nausea and vomiting of pregnancy. American Journal of Obstetrics and Gynecology 2008;198(1):71.e1‐71.e7. [DOI] [PubMed] [Google Scholar]
Lacroix 2000
- Lacroix R, Eason E, Melzack R. Nausea and vomiting during pregnancy: a prospective study of its frequency, intensity, and patterns of change. American Journal of Obstetrics and Gynecology 2000;182(4):931‐7. [DOI] [PubMed] [Google Scholar]
Locock 2008
- Locock L, Alexander J, Rozmovits L. Women's responses to nausea and vomiting in pregnancy. Midwifery 2008;24:143‐52. [DOI] [PubMed] [Google Scholar]
Louik 2006
- Louik C, Hernandez‐Diaz S, Werler MM, Mitchell AA. Nausea and vomiting in pregnancy: maternal characteristics and risk factors. Paediatric and Perinatal Epidemiology 2006;20(4):270‐8. [DOI] [PubMed] [Google Scholar]
Magee 2002a
- Magee LA, Mazzotta P, Koren G. Evidence‐based view of safety and effectiveness of pharmacologic therapy for nausea and vomiting of pregnancy (NVP). American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S256‐S261. [DOI] [PubMed] [Google Scholar]
Magee 2002b
- Magee LA, Chandra K, Mazzotta P, Stewart D, Koren G, Guyatt GH. Development of a health‐related quality of life instrument for nausea and vomiting of pregnancy. American Journal of Obstetrics and Gynecology 2002;186(5):S232‐S238. [DOI] [PubMed] [Google Scholar]
Magee 2006
- Magee L, Shrim A, Koren G. Diagnosis and management of nausea and vomiting in pregnancy. Fetal and Maternal Medicine Review 2006;17(1):45‐67. [Google Scholar]
Mazzotta 2000
- Mazzotta P, Magee LA. A risk‐benefit assessment of pharmacological and nonpharmacological treatment for nausea and vomiting of pregnancy. Drugs 2000;59:781‐800. [DOI] [PubMed] [Google Scholar]
McParlin 2008
- McParlin C, Graham RH, Robson SC. Caring for women with nausea and vomiting in pregnancy: new approaches. British Journal of Midwifery 2008;16(5):280‐5. [Google Scholar]
Melzack 1985
- Melzack R, Rosberger Z, Hollingsworth ML, Thirlwell M. New approaches to measuring nausea. Canadian Medical Association Journal 1985;133(8):755‐8. [PMC free article] [PubMed] [Google Scholar]
Miller 2001
- Miller H, Veciana M, Stewart L, Rebarber A, Rosen T, Slotnick R. A multicenter randomized controlled trial of nerve stimulation therapy: subanalysis of severe nausea and vomiting symptoms [abstract]. American Journal of Obstetrics and Gynecology 2001;185(6 Suppl):S188. [Google Scholar]
Miller 2002
- Miller F. Nausea and vomiting in pregnancy: the problem of perception‐‐is it really a disease?. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S182‐S183. [DOI] [PubMed] [Google Scholar]
Munch 2011
- Munch S, Korst LM, Hernandez GD, Romero R, Goodwin TM. Health‐related quality of life in women with nausea and vomiting of pregnancy: the importance of psycho‐social context. Journal of Perinatology 2011;31(1):10‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
NICE 2008
- National Collaborating Centre for Women's and Children's Health. Antenatal care: routine care for the healthy pregnant woman. Clinical guideline 62. London: National Institute for Clinical Excellence (NICE), March 2008. [Google Scholar]
NICE 2013
- National Collaborating Centre for Women's and Children's Health. Antenatal Care: Routine Care for the Healthy Pregnant Woman. Clinical Guideline 62 (Revised 2013). London: National Institute for Clinical Excellence (NICE), June 2013. [Google Scholar]
Niebyl 2002
- Niebyl JR, Goodwin TM. Overview of nausea and vomiting of pregnancy with an emphasis on vitamins and ginger. American Journal of Obstetrics and Gynecology 2002;186(5 Suppl):S253‐S255. [DOI] [PubMed] [Google Scholar]
O'Brien 1992
- O'Brien B, Naber S. Nausea and vomiting during pregnancy: effects on the quality of women's lives. Birth 1992;19:138‐43. [DOI] [PubMed] [Google Scholar]
O'Brien 1997
- O'Brien B, Relyea J. Diary reports of nausea and vomiting during pregnancy. Clinical Nursing Research 1997;6(3):239. [DOI] [PubMed] [Google Scholar]
O'Brien 1999
- O'Brien B, Relyea MJ. Use of Indigenous explanations and remedies to further understand nausea and vomiting during pregnancy. Health Care for Women International 1999;20(1):49‐61. [DOI] [PubMed] [Google Scholar]
Ornstein 1995
- Ornstein M, Einarson A, Koren G. Bendectin/Diclectin for morning sickness: a Canadian follow‐up of an American tragedy. Reproductive Toxicology 1995;9(1):1‐6. [DOI] [PubMed] [Google Scholar]
Persaud 2014
- Persaud N, Chin J, Walker M. Should doxylamine‐pyridoxine be used for nausea and vomiting of pregnancy. Journal of Obstetrics and Gynaecology of Canada 2014;36(4):343‐8. [DOI] [PubMed] [Google Scholar]
Piwko 2007
- Piwko C, Ungar WJ, Einarson TR, Wolpin J, Koren G. The weekly cost of nausea and vomiting of pregnancy for women calling the Toronto Motherisk Program. Current Medical Research and Opinion 2007;23(4):833‐40. [DOI] [PubMed] [Google Scholar]
Piwko 2013
- Piwko C, Koren G, Babashov V, Vicente C, Einarson TR. Economic burden of nausea and vomiting of pregnancy in the USA. Journal of Population Therapeutics and Clinical Pharmacology [Journal de la Therapeutique des Populations et de la Pharmacologie Clinique] 2013;20(2):e149‐e160. [PubMed] [Google Scholar]
Pongrojpaw 2007b
- Pongrojpaw D, Somprasit C, Chanthasenanont A. A randomized comparison of ginger and dimenhydrinate in the treatment of nausea and vomiting in pregnancy. Journal of the Medical Association of Thailand 2007;90(9):1703‐9. [PubMed] [Google Scholar]
Quinlan 2003
- Quinlan JD, Hill DA. Nausea and vomiting of pregnancy. American Family Physician 2003;68(1):121‐8. [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rhodes 1984
- Rhodes V, Watson P, Johnson M. Development of reliable and valid measures of nausea and vomiting. Cancer Nursing 1984;7:33‐41. [PubMed] [Google Scholar]
Schunemann 2009
- Schunemann HJ. GRADE: from grading the evidence to developing recommendations. A description of the system and a proposal regarding the transferability of the results of clinical research to clinical practice [GRADE: Von der Evidenz zur Empfehlung. Beschreibung des Systems und Losungsbeitrag zur Ubertragbarkeit von Studienergebnissen]. Zeitschrift fur Evidenz, Fortbildung und Qualitat im Gesundheitswesen 2009;103(6):391‐400. [PUBMED: 19839216] [DOI] [PubMed] [Google Scholar]
Seto 1997
- Seto A, Einarson T, Koren G. Pregnancy outcome following first trimester exposure to antihistamines: meta‐analysis. American Journal of Perinatology 1997;14(3):119‐24. [DOI] [PubMed] [Google Scholar]
Slaughter 2014
- Slaughter SR, Hearns‐Stokes R, Vlugt T, Joffe HV. FDA approval of doxylamine‐pyridoxine therapy for use in pregnancy. New England Journal of Medicine 2014;370:1081‐3. [DOI] [PubMed] [Google Scholar]
South Australian Health Commission 1999
- South Australian Health Commission. South Australian Health Commission (Pregnancy Outcome Statistics) Regulations. South Australian Health Commission, 1999. [Google Scholar]
Swallow 2002
- Swallow BL, Lindow SW, Masson EA, Hay DM. Development of an instrument to measure nausea and vomiting in pregnancy. Journal of Obstetrics and Gynaecology 2002;22(5):481‐5. [DOI] [PubMed] [Google Scholar]
Swallow 2004
- Swallow BL, Lindow SW, Masson EA, Hay DM. Psychological health in early pregnancy: relationship with nausea and vomiting. Journal of Obstetrics and Gynaecology 2004;24(1):28‐32. [DOI] [PubMed] [Google Scholar]
Swallow 2005
- Swallow BL, Lindow SW, Masson EA, Hay DM. Women with nausea and vomiting in pregnancy demonstrate worse health and are adversely affected by odours. Journal of Obstetrics and Gynaecology 2005;25(6):544‐9. [DOI] [PubMed] [Google Scholar]
Tiran 2002
- Tiran D. Nausea and vomiting in pregnancy: safety and efficacy of self‐administered complementary therapies. Complementary Therapies in Nursing and Midwifery 2002;8(4):191‐6. [DOI] [PubMed] [Google Scholar]
Tiran 2003
- Tiran D. The use of herbs by pregnant and childbearing women: a risk‐benefit assessment. Complementary Therapies in Nursing & Midwifery 2003;9(4):176‐81. [DOI] [PubMed] [Google Scholar]
Tiran 2012
- Tiran D. Ginger to reduce nausea and vomiting during pregnancy: evidence of effectiveness is not the same as proof of safety. Complementary Therapies in Clinical Practice 2012;18:22‐5. [DOI] [PubMed] [Google Scholar]
UKTIS 2012
- UKTIS. Treatment of nausea and vomiting in pregnancy. TOXBASE. UK Teratology Information Service (www.toxbase.org) 2012.
Viljoen 2014
- Viljoen E, Visser J, Koen N, Musekiwa A. A systematic review and meta‐analysis of the effect and safety of ginger in the treatment of pregnancy‐associated nausea and vomiting. Nutrition Journal 2014;13:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
Weigel 1989
- Weigel MM, Weigel RM. Nausea and vomiting of early pregnancy and pregnancy outcomes. An epidemiological study. British Journal of Obstetrics and Gynaecology 1989;96:1304‐11. [DOI] [PubMed] [Google Scholar]
Westfall 2004
- Westfall RE. Use of anti‐emetic herbs in pregnancy: women's choices, and the question of safety and efficacy. Complementary Therapies in Nursing & Midwifery 2004;10(1):30‐6. [DOI] [PubMed] [Google Scholar]
Wilkinson 2000
- Wilkinson JM. What do we know about herbal morning sickness treatments? A literature survey. Midwifery 2000;16(3):224‐8. [DOI] [PubMed] [Google Scholar]
Wood 2013
- Wood H, McKellar LV, Lightbody M. Nausea and vomiting in pregnancy: blooming or bloomin' awful?. Women and Birth 2013;26(2):100‐4. [DOI] [PubMed] [Google Scholar]
Woolhouse 2006
- Woolhouse M. Complementary medicine for pregnancy complications. Australian Family Physician 2007;35(9):695. [PubMed] [Google Scholar]
Zhou 1999
- Zhou Q, O'Brien B, Relyea J. Severity of nausea and vomiting during pregnancy: what does it predict?. Birth 1999;26(2):108‐14. [DOI] [PubMed] [Google Scholar]
Zhou 2001
- Zhou Q, O'Brien B, Soeken K. Rhodes Index of Nausea and Vomiting‐‐Form 2 in pregnant women. A confirmatory factor analysis. Nursing Research 2001;50(4):251‐7. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Jewell 2003a
- Jewell D, Young G. Interventions for nausea and vomiting in early pregnancy. Cochrane Database of Systematic Reviews 2003, Issue 4. [DOI: 10.1002/14651858.CD000145] [DOI] [PubMed] [Google Scholar]
Matthews 2010
- Matthews A, Dowswell T, Haas DM, Doyle M, O'Mathúna DP. Interventions for nausea and vomiting in early pregnancy. Cochrane Database of Systematic Reviews 2010, Issue 9. [DOI: 10.1002/14651858.CD007575.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Matthews 2014
- Matthews A, Haas DM, O'Mathúna DP, Dowswell T, Doyle M. Interventions for nausea and vomiting in early pregnancy. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD007575.pub3] [DOI] [PubMed] [Google Scholar]