
Figure 3. Association Between Multiple Sclerosis (MS) and Risk of Macrovascular Disease and Mortality Between January 1987 and September 2018 in England.
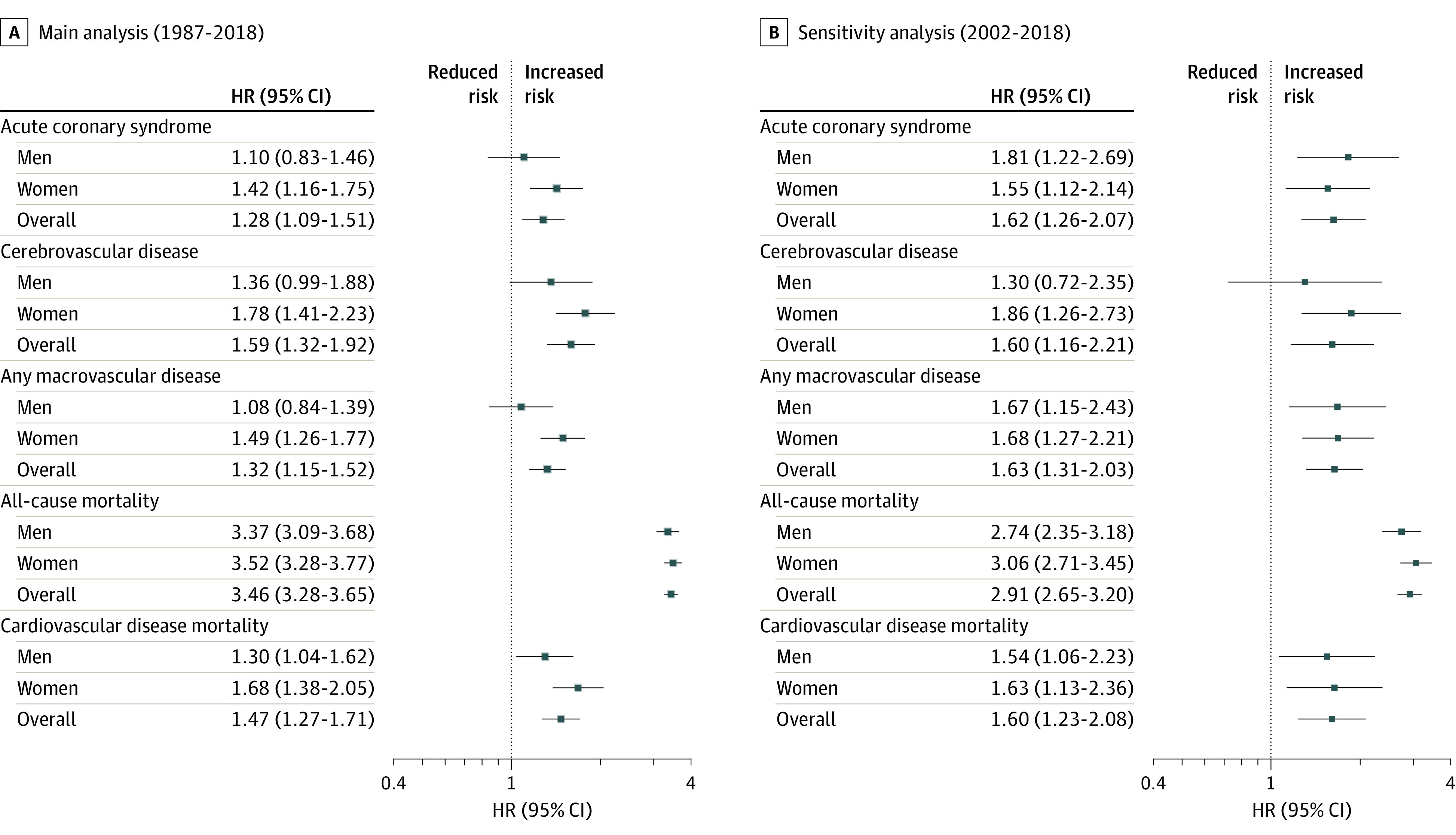
Analyses of mortality outcomes included all individuals with a diagnosis of MS after January 1, 1987, who met case definition criteria for MS and matched controls (see Methods). For analyses of macrovascular diseases, people with a history of the condition at baseline were excluded from the analysis. Date of MS diagnosis was considered as the index date, and a matched index date was assigned to matched controls. Multivariable Cox proportional hazards regression models were used to model the association between MS status and incident rates of acute coronary syndrome, cerebrovascular disease, any macrovascular disease (including acute coronary syndrome, cerebrovascular disease, and peripheral arterial disease), and all-cause mortality. To model differences in rates of cardiovascular disease mortality, competing-risk regressions based on the Fine and Gray proportional subhazard model was used that considered noncardiovascular disease mortality as a competing event, and cumulative incidence functions were computed for subgroups of interest. Regression analyses were adjusted for the following baseline covariates: age; sex; race/ethnicity; index of multideprivation; smoking status; diagnosis of diabetes or depression; use of lipid-lowering, oral antidiabetic, antihypertensive, antiplatelet, and anticoagulation medications; and number of primary care visits in the year before the diagnosis of MS and for the year of diagnosis of MS. For the sensitivity analysis, only patients with MS (and matched controls) who received a diagnosis during the period from 2002 to 2018 were included. HR indicates hazard ratio.