

Abstract
Objective:
To estimate the prevalence of health care transition components among youth with autism spectrum disorder (ASD) aged 12-17 using the 2016 National Survey of Children’s Health (NSCH), compared to youth with other mental, behavioral, or developmental disorders (MBDDs) or youth without MBDDs.
Methods:
The 2016 NSCH is a nationally and state representative survey that explores issues of health and well-being among children ages 0-17. Within the NSCH, parents of a subset of youth, ages 12-17, are asked a series of questions about their youth’s eventual transition into the adult health care system. The current study explores components of this transition, comparing youth diagnosed with ASD, youth with other mental, behavioral, or developmental disorders (MBDDs), and youth without MBDDs.
Results:
Approximately 1-in-4 youth with ASD had actively worked with their doctor to understand future changes to their health care, significantly less than youth with other MBDDs and youth without MBDDs. Fewer than 2-in-5 youth with ASD had met with their doctor privately or had a parent who knew how their youth would be insured when they reached adulthood.
Conclusions:
The current analysis of a nationally representative sample of youth reveals discrepancies in the proportion of youth with ASD receiving appropriate health care transition planning compared to youth with other MBDDs and youth without MBDDs. These findings suggest the potential for barriers among youth with ASD to effectively transitioning into the adult health care system.
Keywords: autism spectrum disorder, transition, NSCH, health care
Health care transition (HCT) planning is the individualized process of addressing the comprehensive healthcare needs of adolescents as they age into adulthood, and was designed to ensure developmentally appropriate health care services are available in an uninterrupted manner (AAP et al., 2011). Although HCT planning is necessary and recommended for all adolescents, researchers and practitioners have made efforts to emphasize the importance of such planning for youth with special health care needs (YSHCN), particularly youth with mental, behavioral, and developmental disorders (AAP et al., 2002). These youth usually have a harder time during this transition period, as it can be challenging to find high-quality developmentally appropriate health care services in adulthood, which may be further complicated by eligibility issues for supportive services (Gore et al., 2007; Hogan & Astone, 1986; Rutter, 1993). In fact, several studies have corroborated an increased need for HCT planning among these youth, underscored by the high number not receiving any services to aid in this transition (Cheak-Zamora et al., 2013; Lotstein et al., 2009; Nageswaran et al., 2011). Recent research has also demonstrated a link between HCT planning and better health outcomes in adulthood among a population of former youth with chronic health conditions (Sharma et al., 2014).
A population of youth who may have an additional need for HCT planning are youth with autism spectrum disorder (ASD), who use more health care services, have more inpatient hospital visits that are longer in mean duration, make more health care claims, and have higher healthcare expenditures when compared to their peers with other special health care needs (Tregnago & Cheak-Zamora, 2012). Youth with ASD additionally have high rates of unmet medical needs, particularly among children with comorbid psychiatric conditions (Zablotsky et al., 2015; Zablotsky, Maenner, & Blumberg, 2019).
Current research shows that youth with ASD less often receive HCT planning than other YSHCN; estimates are that only 15-21% of transition age youth (between 12-17 years of age) with ASD receive HCT planning (Cheak-Zamora et al., 2013; Cheak-Zamora et al., 2014; Rast et al., 2018).
The transition to the adult medical care is difficult because complex needs must be communicated to a new provider, yet a limited number of providers of adult care feel they have adequate knowledge or skills to provide care to adults with ASD (Zerbo et al., 2015). Compounding this challenge is the fact that the transition period spans across many service systems, likely without overlapping providers (Narendorf, Shattuck & Sterzing, 2011; Shattuck et al., 2011).
In addition to the prevalent deficiencies in HCT planning among youth with ASD, recent literature shows this population is both growing in size and changing in health characteristics (Baio et al., 2018; Christensen et al., 2016). The increased size of this population marks it as an important public health concern. The changes of the demographic composition and distribution of impairments, including fewer youth with an intellectual disability and smaller differences in prevalence by race, ethnicity, and sex (Baio et al., 2018; Christensen et al., 2016) should be considered as research is updated. Understanding the experiences and needs of this changing population is integral to providing targeted services and interventions.
The majority of research on HCT planning at the national level comes from a survey of children with special health care needs (SHCN), the most recent estimates accompanying the 2009-2010 National Survey of Children with Special Health Care Needs (NS-CSHCN) (e.g., Lotstein et al. 2009, Cheak-Zamora et al. 2013). The NS-CSHCN was a sample of children (0-17 years of age) with SHCN identified based on a five question screener designed to capture the presence of a chronic health condition and the use of medical services (Bethell et al., 2002). Although an important source of detailed health and health needs information, the NS-CSHCN was not representative of the experiences of all children, but instead was exclusively those experiences of children with special health care needs.
In 2016, the National Survey of Children’s Health (NSCH) was redesigned, combining elements of former NS-CSHCN and NSCH questionnaires and sampling frameworks, resulting in broader topical coverage in an expanded sample of children with and without SHCN. This creates a unique opportunity to explore transition questions in a timely and nationally representative sample of all children. The primary objective of the current study is to describe health care transition components among the population of youth with ASD, youth with other mental, behavioral, or developmental disorders, and youth without any mental, behavioral, or developmental disorders serving as comparisons.
Methods
Source
Data come from the 2016 National Survey of Children’s Health (NSCH), a cross-sectional, nationally representative population-based survey designed to monitor the health and well-being of non-institutionalized children in the United States ages 0-17. The NSCH is sponsored by the Health Resources and Services Administration’s Maternal and Child Health Bureau and is conducted by the United States Census Bureau. As a secondary data analysis of a deidentified data set, this study is exempt from review by the NCHS Ethics Review Board.
Households are randomly selected for inclusion in the NSCH (from the Census Master Address File appended with indicators from the Census Bureau’s Center for Administrative Records Research and Applications), receiving a mailed invitation in the form of a household screener questionnaire. The screener includes questions about the race and ethnicity, age, sex, and English proficiency (for children over 4 years of age) for all children in the household. Additionally, the screener asks about whether any child has a SHCN, as defined through responses to a series of questions focused on functional limitation, prescription medication use, elevated service use or need, use of specialized therapies, and/or ongoing emotional, developmental, or behavioral conditions requiring treatment (Bethell et al., 2002). Eligible households later receive an invitation to complete the NSCH on one randomly selected child either by completing a mailed paper version of the questionnaire or by completing the survey online using a secure confidential website. Three separate questionnaires were developed for different age groups: 0-5, 6-11, and 12-17 years of age.
A total of 50,212 interviews were completed in the 2016 NSCH, with an overall weighted response rate of 40.7%; the survey completion rate among eligible households was 69.7%. Respondents were adults familiar with the health and health care of the sampled child, with the vast majority of respondents being the child’s parent (93% of cases; hereafter referred to as parents). For more information about the NSCH, including survey methods and response rates, see https://mchb.hrsa.gov/data/national-surveys. Data used in the current paper were publicly available.
Sample
Eligibility for the analytic sample included being between the ages of 12-17 years (hereafter referred to as “youth”), with information available on whether the youth had been diagnosed with a current mental, behavioral, or developmental disorder (MBDD) (n=20,121) (less than 3% of the sample was missing on MBDD status). The sample was divided into three subgroups: youth who were currently diagnosed with ASD (n=586); youth currently diagnosed with any other current mental, behavioral, or developmental disorder (other MBDD) (n=4,735); and youth without a current MBDD (n=14,800).
Measures
Health Care Transition Components
The current study focuses on several questions dedicated to a youth’s transition into the adult health care system. Three health care transition components were examined.
Active work:
Parents were asked four questions about whether the youth’s doctor or other health care provider had actively worked with their youth to 1) “think about and plan for his or her future,” 2) “make positive choices about his or her health,” 3) “gain skills to manage his or her health and health care,” and 4) “understand the changes in health care that happen at age 18”. Youth whose parents answered in the affirmative to at least three of the four items were considered to be actively working with their doctor.
Insurance:
Additionally, parents were asked “Do you know how this child will be insured as he or she becomes an adult?” This question is intended to serve as a proxy for whether the child will likely have continued health insurance coverage which facilitates health care and receipt of transition planning.
Independence:
Parents were also asked whether their youth had had “a chance to speak with the doctor or other health care provider privately, without you or another adult in the room?” at their youth’s last preventive check-up. This question evaluates whether the youth is building independent health care skills.
Comparison Groups
We created three comparison groups for this study based on a series of questions about the presence of a diagnosed condition. Parents were asked “Has a doctor or other health care provider [or educator] EVER told you that this child has [specified condition]?”. In instances where the parent answered in the affirmative, the follow-up question was asked, “does the child CURRENTLY have the condition?”. Ten conditions were considered mental, behavioral or developmental disorders (MBDDs) for the purpose of this study, which included: “autism or autism spectrum disorder (including diagnoses of Asperger’s Disorder or Pervasive Developmental Disorder (PDD),” “attentive deficit disorder or attention-deficit/hyperactivity disorder,” “depression,” “anxiety problems,” “behavioral or conduct problems,” “Tourette syndrome,” “learning disability,” “intellectual disability (also known as mental retardation),” “developmental delay,” and “speech or other language disorder”. We created the following groups: 1) youth with current autism spectrum disorder, 2) youth with current other mental, behavioral, or developmental disorders, and 3) youth without current mental, behavioral, or developmental disorders. Youth with both autism spectrum disorder and some other mental, behavioral, or developmental disorder, which was common (n=534, 92%) were placed in the autism spectrum disorder group.
Demographic characteristics
Youth characteristics included age, sex, race and ethnicity, insurance status (any current private; current public only; uninsured), and whether the youth is currently receiving services under a special education or early intervention plan, including through an Individualized Education Plan (IEP). Family characteristics included federal poverty level ratio, family structure, highest education reported among adults in the family, and geographic region.
Statistical analysis
Estimates were calculated using Stata 13.0 to account for the complex survey design of the NSCH, incorporating both the sampling weights and the sample design variables. First, demographic characteristics were described for youth diagnosed with ASD, youth diagnosed with other MBDDs, and youth without current MBDDs (Table 1). A design-based Rao-Scott corrected χ2 test was used to test whether an overall difference existed between these groups for each characteristic. Next, the proportion in each group who had experienced each of the four indicators of active work (see Figure 1) and three health transition components of active work, insurance and independence (see Table 2; Figure 2) was calculated, and χ2 tests were again used to detect whether a difference existed among the three groups’ unadjusted estimates. When the χ2 produced a significant test statistic (p<.05), a series of multivariate logistic regressions (rotating which of the three groups was the reference group) were used as an adjustment follow-up to examine whether the proportion of children in each group differed significantly after controlling for youth (age, race and ethnicity, sex, insurance status, current IEP) and family (federal poverty level, family structure, highest education, region) demographics.
Table 1.
Demographic characteristics of the analytic, by MBDD status
| Current ASD (n=586) % (SE) |
Current Other MBDD (n=4,735) % (SE) |
No current MBDD (n=14,800) % (SE) |
p-value1 | |
|---|---|---|---|---|
| Youth characteristics | ||||
| Sex | <.001 | |||
| Male | 80.7 (3.4) | 53.6x (1.5) | 49.6x (1.0) | |
| Female | 19.3 (3.4) | 46.4 (1.5) | 50.4 (1.0) | |
| Age | .18 | |||
| 12-14 | 57.1 (3.9) | 48.8 (1.5) | 49.8 (1.0) | |
| 15-17 | 42.9 (3.9) | 51.2 (1.5) | 50.2 (1.0) | |
| Race | <.001 | |||
| Non-Hispanic white | 67.6 (3.8) | 59.4 (1.6) | 51.1xy (1.0) | |
| Non-Hispanic black | 15.2 (3.5) | 13.5 (1.1) | 13.7 (0.7) | |
| Non-Hispanic other | 6.4 (1.3) | 7.2 (0.6) | 10.4xy (0.5) | |
| Hispanic | 10.8 (2.2) | 19.9x (1.6) | 24.9xy (1.1) | |
| Insurance status | <.001 | |||
| Private | 52.1 (4.1) | 58.3 (1.6) | 67.9xy (1.0) | |
| Public | 46.2 (4.1) | 36.8x (1.6) | 25.1xy (1.0) | |
| Uninsured | 1.8 (0.7) | 4.9x (0.7) | 7.0xy (0.6) | |
| Current IEP | 70.1 (3.7) | 29.7x (1.4) | 1.9xy (3.2) | <.001 |
| Family characteristics | ||||
| Family structure | <.001 | |||
| Two parent, married | 53.8 (4.2) | 57.2 (1.5) | 67.7xy (0.9) | |
| Two parent, unmarried | 10.6 (2.9) | 7.1 (0.9) | 6.7 (0.5) | |
| Single mother | 24.7 (3.8) | 23.8 (1.3) | 16.9xy (0.7) | |
| Other | 10.9 (3.4) | 11.9 (0.9) | 8.7y (0.6) | |
| Federal poverty level | .09 | |||
| <100% | 26.7 (4.0) | 22.5 (1.3) | 20.0 (1.0) | |
| 100-199% | 20.9 (3.5) | 23.3 (1.4) | 20.9 (0.9) | |
| 200-399% | 23.3 (2.9) | 24.5 (1.2) | 27.1 (0.8) | |
| ≥400% | 29.2 (3.3) | 29.7 (1.3) | 31.9 (0.8) | |
| Highest education family member | .60 | |||
| Less than high school | 9.1 (3.7) | 10.3 (1.5) | 10.2 (0.9) | |
| High school graduate | 23.0 (4.0) | 23.5 (1.4) | 20.6 (0.9) | |
| Some college or more | 68.0 (4.6) | 66.1 (1.7) | 69.2 (1.1) | |
| Region | .001 | |||
| Northeast | 16.8 (2.4) | 16.7 (1.1) | 16.4 (0.6) | |
| Midwest | 21.9 (3.0) | 23.9 (1.1) | 20.5y (0.5) | |
| South | 45.3 (4.1) | 39.4 (1.5) | 37.5 (0.9) | |
| West | 16.1 (2.3) | 20.0 (1.3) | 25.6xy (0.9) | |
Notes: ASD = autism spectrum disorder, MBDD = mental, behavioral, or developmental disorder, IEP = Individualized Education Plan.
Differences in proportions was examined using Rao-Scott corrected χ2 tests.
Significantly different than youth with autism spectrum disorder based on unadjusted odds ratio (p<.05).
Significantly different than youth with other mental, behavioral, or developmental disorders based on unadjusted odds ratio (p<.05).
Figure 1.
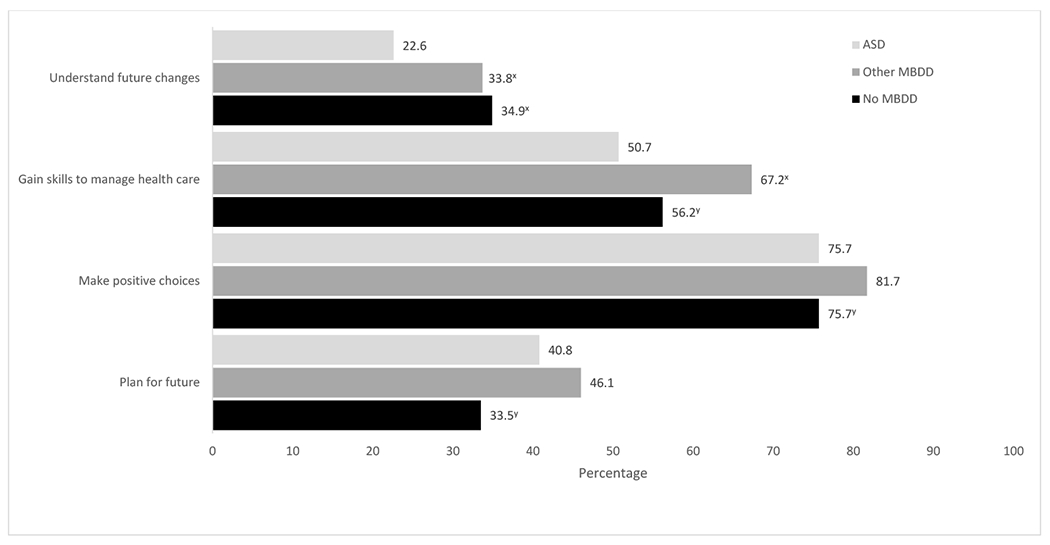
Prevalence of active work indicators, by MBDD status
NOTES: ASD = autism spectrum disorder; MBDD = mental, behavioral, or developmental disorder.
Indicators presented are unadjusted estimates.
x Significantly different than youth with autism spectrum disorder based on adjusted odds ratio (p<.05).
y Significantly different than youth with other mental, behavioral, or developmental disorders based on adjusted odds ratio (p<.05).
Odds ratios are adjusted for youth (age, race and ethnicity, sex, insurance status, current IEP) and family (federal poverty level, family structure, highest education, region) demographics.
Table 2.
Prevalence of health care transition components, by MBDD status
| Unadjusted % (SE) | Adjusted ORs (95% CI) | |||||
|---|---|---|---|---|---|---|
| Current ASD | Current Other MBDD | Current No MBDD | ASD vs. Other MBDD | ASD vs. No MBDD | Other MBDD vs. No MBDD | |
| Actively working with doctor1 | 34.4 (4.1) | 48.6 (1.7) | 39.8 (1.1) | 0.59** (0.41-0.85) | 0.86 (0.59-1.26) | 1.46*** (1.22-1.74) |
| Parent knows how youth will be insured | 39.0 (3.7) | 48.0 (1.5) | 56.8 (1.0) | 0.73 (0.50-1.07) | 0.59** (0.40-0.87) | 0.80* (0.68-0.95) |
| Youth sees doctor privately | 37.8 (4.2) | 52.2 (1.6) | 48.7 (1.1) | 0.62* (0.39-0.98) | 0.76 (0.47-1.23) | 1.22* (1.02-1.46) |
NOTES: ASD is autism spectrum disorder; MBDD is mental, behavioral, or developmental disorder
Youth had a parent who endorsed at least three of the four indicators that make up the active work component.
Odds ratios are adjusted for youth (age, race and ethnicity, sex, insurance status, current IEP) and family (federal poverty level, family structure, highest education, region) demographics.
A Rao-Scott corrected χ2 test was significant for each of the three health transition components and diagnostic group (p’s<.01).
p<.001
p<.01
p<.05
Figure 2.
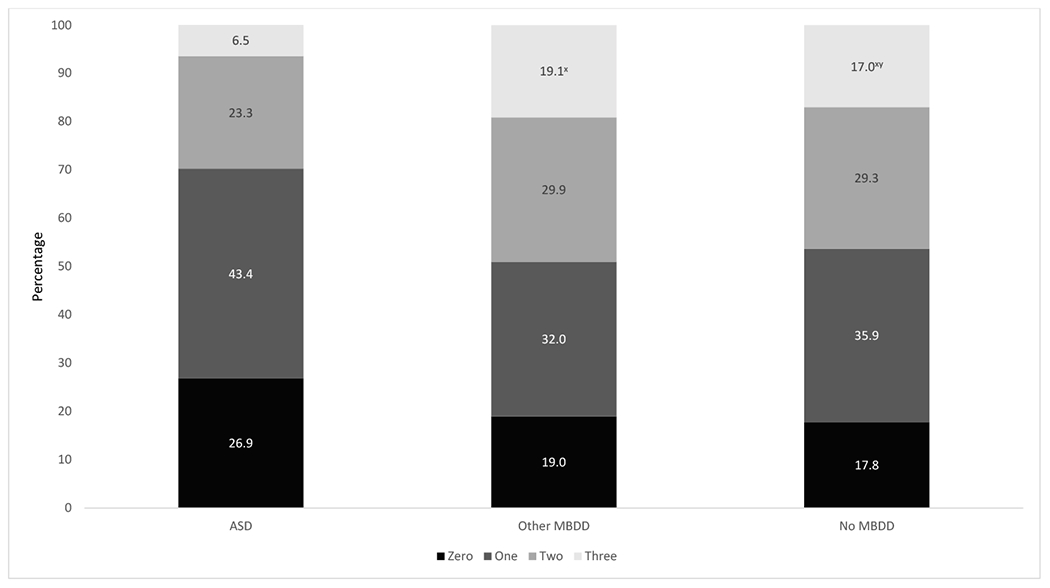
Number of health care transition components, by MBDD status
NOTES: ASD is autism spectrum disorder; MBDD is mental, behavioral, or developmental disorder
The three HCT components presented are unadjusted estimates and include active work, insurance, and independence. Youth had to have a parent who endorsed at least three of the four indicators to be considered to meet the active work HCT component.
x Significantly different than youth with autism spectrum disorder based on adjusted odds ratio (p<.05).
y Significantly different than youth with other mental, behavioral, or developmental disorders based on adjusted odds ratio (p<.05).
Odds ratios are adjusted for youth (age, race and ethnicity, sex, insurance status, current IEP) and family (federal poverty level, family structure, highest education, region) demographics.
Adjusted predicted marginal probabilities and adjusted odds ratios for all models can be found in an online supplemental table. There were no missing data for the youth’s sex, race and ethnicity, or family poverty ratio due to single hot-deck imputations performed by the US Census Bureau (2011). Missing data on family type, youth insurance type, and highest education in the family were limited to less than 3% of the analytic sample.
Results
Table 1 contains demographic information about youth in the analytic sample. Youth with ASD were most likely to be male, have an IEP and be on public health insurance, but were least likely to be Hispanic or uninsured. Youth without MBDDs were most likely to be Hispanic, living in two married parent household and have private health insurance. Youth with other MBDDs were more likely to live in the Midwest, but less likely to live in the West when compared to youth without MBDDs.
Figure 1 presents the prevalence of the four active work indicators. Approximately 1 in 4 youth with ASD (22.6%) had actively worked with their doctor to understand future changes to their health care, a significantly lower proportion compared to youth with other MBDDs (33.8%) (p<.01) and youth without MBDDs (34.9%) (p<.01), after adjustment for youth and family characteristics. After adjustment, youth with ASD (50.7%) were also less likely to have worked with their doctor to gain skills to manage their health and health care than youth with other MBDDs (67.2%) (p<.01). Youth without MBDDs were less likely than youth with other MBDDs to have actively worked with their doctor to gain skills to manage health and health care (56.2% vs. 67.2%) (p<.01), make positive choices (75.7% vs. 81.7%) (p<.001), and plan for the future (33.5% vs. 46.1%) (p<.001), after adjustment. The difference in making positive choices between youth with ASD (75.7%) and youth with other MBDDs (81.7%) was comparable to that between youth with other MBDDs and youth without MBDDs (75.7%), but was not statistically significant, presumably due to the smaller sample size for youth with ASD.
Table 2 presents the composite of whether the youth was considered to be actively working with their provider (defined as having at least three of the four items from Figure 1). About 1 in 3 youth with ASD were actively working with their doctor (34.4%), significantly less than youth with other MBDDs (48.6%) (p<.01), who were significantly more likely to have actively worked with their doctor compared to youth without MBDDs (39.8%) (p<.001). However, youth without MBDDs (56.8%) were significantly more likely to have parents who know how their youth will be insured when they reach adulthood compared to either youth with ASD (39.0%) (p<.01) or other MBDDs (48.0%) (p<.05). Approximately half of youth with other MBDDs have met with their doctor privately (52.2%), which was significantly more likely than youth with ASD (37.8%) (p<.05) and youth without MBDDs (48.7%) (p<.05).
Figure 2 depicts the distribution of the three HCT components (active work (having at least three of the four indicators), insurance, independence) experienced by group. Youth with ASD were the least likely to have all three HCT components (6.5%) with only about 1 in 15 youth having accomplished all three components of actively working with their doctor, meeting with their doctor privately, and having a parent who knows how they will be insured when they reach adulthood when compared to youth with other MBDDs (19.1%) (p<.001) and youth without MBDDs (17.0%) (p<.05). Youth with other MBDDs were the most likely to have all three HCT components.
Discussion
Overall, youth with ASD were less likely to have completed HCT items when compared to youth with other MBDDs and youth without MBDDs. Youth with ASD were less likely than their peers with other MBDDs to be actively working with their doctor or meeting with their doctor privately, and less likely than youth without MBDDs to have a parent who knows how they’ll be insured when they reached adulthood.
We found that the prevalence of HCT components among youth with ASD was lower, with 1 in 3 doctors actively working with these youth or meeting with them privately. Providers possibly have lowered expectations that youth with ASD will be able to take over healthcare decisions and actions when they reach adulthood (Burdo-Hartman & Patel, 2008; Kingsnorth et al., 2011) which may be compounded by a shortage of adult primary care providers who are knowledgeable about the unique needs among youth with mental or developmental disabilities (Cheak-Zamora & Teti, 2015).
Regardless, the needs of youth with ASD are unlikely to decline as they reach adulthood given current projections of service utilization through transition (Nathenson & Zablotsky, 2017). In addition, emerging evidence suggests that adults with ASD are more likely to have major chronic medical conditions than adults without ASD, including hypertension, diabetes, thyroid disease, GI disorders, and seizures (Croen et al., 2015).
Typically coinciding with a transition into the adult health care system is an exit from the education system. Given the reliance on supportive services such as mental health care through special education, many youth with mental, behavioral, and developmental disorders experience what is referred to as a “services cliff” during this transition age. Roughly 50,000 youth with ASD are estimated to turn 18 every year (Shattuck et al., 2012a), a number that has steadily increased with the increasing prevalence of ASD (now 1 in 59 children) (Baio et al., 2018), and many will be particularly vulnerable during this time because of the complexity of their service needs and functional challenges. During secondary school, parents of youth with ASD more often report insufficient services and expending greater effort to receive needed services than other youth in special education (Levine, Marder, & Wagner, 2007). The percentage of families who report some or great effort to access services increases following exit from secondary school (Roux et al., 2015). Postsecondary education is a source of support for some young adults with ASD after leaving special education services in high school (about 1/3 attend within the first several years after leaving high school (Shattuck et al., 2012b)), but services provided through a college setting are less comprehensive than those services received through special education in secondary school, and are often only academically focused, if received at all (Gelbar, Smith, & Reichow, 2014).
Implications
More comprehensive health care in young adulthood and the provision of health care transition have the potential to improve the health outcomes of young adults with these conditions (AAP et al., 2011). HCT services are designed to maximize lifelong functioning and potential by providing patient-centered care during the transition (AAP et al., 2002) and are increasingly recognized as a desirable outcome for all youth, and particularly youth with special health care needs. The American Academy of Pediatrics has emphasized the importance of providing health care transition to youth, particularly youth with special health care needs, in a 2002 consensus statement with American Academy of Family Physicians, and the American College of Physicians-American Society of Internal Medicine (AAP et al., 2002). The Maternal and Child Health Bureau has also named HCT as a Title V Maternal and Child Health Services Block Grant program National Performance Measure (CAMHI, 2018) and Healthy People 2020 has a goal to increase the proportion of YSCHN whose health care provider has discussed transition planning from pediatric to adult health care (Healthy People 2020).
Limitations and strengths
A major strength of using data from a large and nationally representative survey such as the National Survey of Children’s Health is the ability to generalize findings and explore associations and outcomes in various subgroups, including disentangling youth with ASD from other youth with mental, behavioral, or developmental disorders. However, in some instances statistical tests of differences in prevalence between youth with ASD and youth from other groups may have been underpowered due to the smaller sample size for youth with ASD.
Additionally, the cross-sectional nature of the NSCH prevents the determination of directionality or causality in the associations examined. Several questions ask parents to assess whether their youth is actively working with their doctor, and a parent’s perception of their youth’s preparedness for transition may possibly influence their response to various indicators. If some youth are meeting privately with their doctor, parents may not be fully aware of what activities are taking place.
Finally, the reliance on parental report for all current diagnoses is subject to recall biases and diagnoses have not been validated either through clinical evaluation or educational records. Some children who appear in the control group may possibly have been diagnosed with a mental, behavioral, or developmental disorder had they been evaluated.
Conclusions
Findings from the current study of a nationally representative sample of youth with ASD highlight a population where less than half have received key health care transition components. Future iterations of the National Survey of Children Health provide an opportunity to continue monitoring health care transition and better understand the unique needs of youth with ASD.
Supplementary Material
Significance:
This study provides a timely update of HCT planning components in youth with autism spectrum disorder from a national survey, compared to youth with other mental, behavioral, and developmental disorders (MBDDs), and youth without MBDDs.
Footnotes
Publisher's Disclaimer: Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC, HRSA, HHS nor does mention of these department or agency names imply endorsement by the US government.
Financial disclosure: The authors have indicated that they have no financial relationships relative to this article to disclose.
Conflicts of interest: None to disclose.
References
- American Academy of Pediatrics, American Academy of Family Physicians, American College of Physicians, & Transitions Clinical Report Authoring Group. (2011). Clinical report—Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics 128(1):182–200. [DOI] [PubMed] [Google Scholar]
- American Academy of Pediatrics, American Academy of Family Physicians, & American College of Physicians-American Society of Internal Medicine. (2002). A consensus statement on health care transitions for young adults with special health care needs. Pediatrics 110(Supplement 3):1304–1306. [PubMed] [Google Scholar]
- Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J Warren Z & … Dowling NF (2018). Prevalence of autism spectrum disroder among children aged 8 years – autism and developmental disabilities monitoring network, 11 sites, United States, 2014. Morbidity and Mortality Weekly Report, 67(6):1–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bethell CD, Read D, Stein RE, Blumberg SJ, Wells N, & Newacheck PW (2002). Identifying children with special health care needs: development and evaluation of a short screening instrument. Ambulatory Pediatrics, 2(1), 38–48. [DOI] [PubMed] [Google Scholar]
- Burdo-Hartman WA, & Patel DR (2008). Medical home and transition planning for children and youth with special health care needs. Pediatric Clinics of North America, 55(6), 1287–1297. [DOI] [PubMed] [Google Scholar]
- Cheak-Zamora NC, Farmer JE, Mayfield WA, Clark MJ, Marvin AR, Law JK, & Law PA (2014). Health care transition services for youth with autism spectrum disorders. Rehabilitation Psychology, 59(3), 340. [DOI] [PubMed] [Google Scholar]
- Cheak-Zamora NC, & Teti M (2015). “You think it’s hard now… It gets much harder for our children”: Youth with autism and their caregiver’s perspectives of health care transition services. Autism, 19(8), 992–1001. [DOI] [PubMed] [Google Scholar]
- Cheak-Zamora NC, Yang X, Farmer JE, & Clark M (2013). Disparities in transition planning for youth with autism spectrum disorder. Pediatrics 131(3), 447–454. [DOI] [PubMed] [Google Scholar]
- Child and Adolescent Health Measurement Initiative (CAHMI), Data Resource Center for Child and Adolescent Health. (2018). 2016 National Survey of Children’s Health: Child and Family Health Measures and Subgroups, SAS Codebook, Version 1.0. http://www.childhealthdata.org. Accessed 15 February 2018.
- Christensen DL, Baio J, Van Naarden-Braun K, Bilder D, Charles J, Constantino JN & … Yeargin-Allsopp M (2016). Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years--Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2012. Morbidity and Mortality Weekly Report, 65(3), 1–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Croen LA, Zerbo O, Qian Y, Massolo ML, Rich S, Sidney S & … Kripke C (2015). The health status of adults on the autism spectrum. Autism, 19(7), 814–823. [DOI] [PubMed] [Google Scholar]
- Gelbar NW, Smith I, & Reichow B (2014). Systematic review of articles describing experience and supports of individuals with autism enrolled in college and university programs. Journal of autism and developmental disorders, 44(10), 2593–2601. [DOI] [PubMed] [Google Scholar]
- Gore S, Aseltine RH Jr., & Schilling EA (2007). Transition to adulthood, mental health, and inequality Mental Health, Social Mirror: Springer; pps. 219–237. [Google Scholar]
- Healthy People 2020. (2018). Washington, DC: U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion; Available at http://healthypeople2020.gov. Accessed 21 February 2018. [Google Scholar]
- Hogan DP, Astone NM (1986). The transition to adulthood. Annual Review of Sociology. 109–130. [Google Scholar]
- Kingsnorth S, Gall C, Beayni S, & Rigby P (2011). Parents as transition experts? Qualitative findings from a pilot parent-led peer support group. Child Care Health Development, 37(6), 833–840. [DOI] [PubMed] [Google Scholar]
- Levine P, Marder C, & Wagner M (2007). Services and Supports for Secondary School Students with Disabilities: A Special Topic Report of Findings from the National Longitudinal Transition Study-2 (NLTS2). National Center For Special Education Research. [Google Scholar]
- Lotstein DS, Ghandour R, Cash A, McGuire E, Strickland B, & Newacheck P (2009). Planning for health care transitions: results from the 2005–2006 national survey of children with special health care needs. Pediatrics, 123(1), e145–e152. [DOI] [PubMed] [Google Scholar]
- Nageswaran S, Parish SL, Rose RA, & Grady MD (2011). Do children with developmental disabilities and mental health conditions have greater difficulty using health services than children with physical disorders? Maternal and Child Health Journal, 15(5), 634–641. [DOI] [PubMed] [Google Scholar]
- Narendorf SC, Shattuck PT, & Sterzing PR (2011). Mental health service use among adolescents with an autism spectrum disorder. Psychiatric Services, 62(8), 975–978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nathenson RA, & Zablotsky B (2017). The transition to the adult health care system among youths with autism spectrum disorder. Psychiatric Services, 68, 735–738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rast JE, Shattuck PT, Roux AM, Anderson KA, & Kuo A (2018). The medical home and health care transition for youth with autism. Pediatrics, 141(Supplement 4), S328–S334. [DOI] [PubMed] [Google Scholar]
- Roux AM, Shattuck PT, Rast JE, Rava JA, & Anderson KA (2015). National Autism Indicators Report: Transition into Young Adulthood. Philadelphia, PA: Life Course Outcomes Research Program Area, A.J. Drexel Autism Institute, Drexel University. [Google Scholar]
- Rutter M (1993). Resilience: Some conceptual considerations. Journal of Adolescent Health 14(8), 626–631. [DOI] [PubMed] [Google Scholar]
- Sharma N, O’Hare K, Antonelli RC, & Sawicki GS (2014). Transition care: future directions in education, health policy, and outcomes research. Academic Pediatrics, 14(2), 120–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shattuck PT, Roux AM, Hudson LE, Taylor JL, Maenner MJ, & Trani JF (2012a). Services for adults with an autism spectrum disorder. Canadian Journal of Psychiatry, 57(5), 284–291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shattuck PT, Narendorf SC, Cooper B, Sterzing PR, Wagner M, & Taylor JL (2012b). Postsecondary education and employment among youth with an autism spectrum disorder. Pediatrics, 129(6), 1042–1049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shattuck PT, Wagner M, Narendorf S, Sterzing P, & Hensley M (2011). Post–high school service use among young adults with an autism spectrum disorder. Archives of Pediatrics & Adolescent Medicine, 165(2), 141–146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tregnago MK, & Cheak-Zamora NC (2012). Systematic review of disparities in health care for individuals with autism spectrum disorders in the United States. Research in Autism Spectrum Disorders, 6(3), 1023–1031. [Google Scholar]
- United States Census Bureau. (2011). 2010 Census Demographic Profile Summary file: 2010 Census of Population and Housing. Available at https://www2.census.gov/programssurveys/decennial/2010/technicaldocumentation/complete-tech-docs/summary-file/dpsf.pdf. Accessed 7 December 2016.
- Zablotsky B, Maenner MJ, & Blumberg SJ (2019). Geographic disparities in treatment for children with autism spectrum disorder. Academic Pediatrics, 19:740–747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zablotsky B, Pringle BA, Colpe LJ, Kogan MD, Rice C, & Blumberg SJ (2015). Service and treatment use among children diagnosed with autism spectrum disorders. Journal of Developmental and Behavioral Pediatrics, 36:98–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zerbo O, Massolo ML, Qian Y, & Croen LA (2015). A study of physician knowledge and experience with autism in adults in a large integrated healthcare system. Journal of Autism and Developmental Disorders, 45(12), 4002–4014. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.