
FIGURE 1.
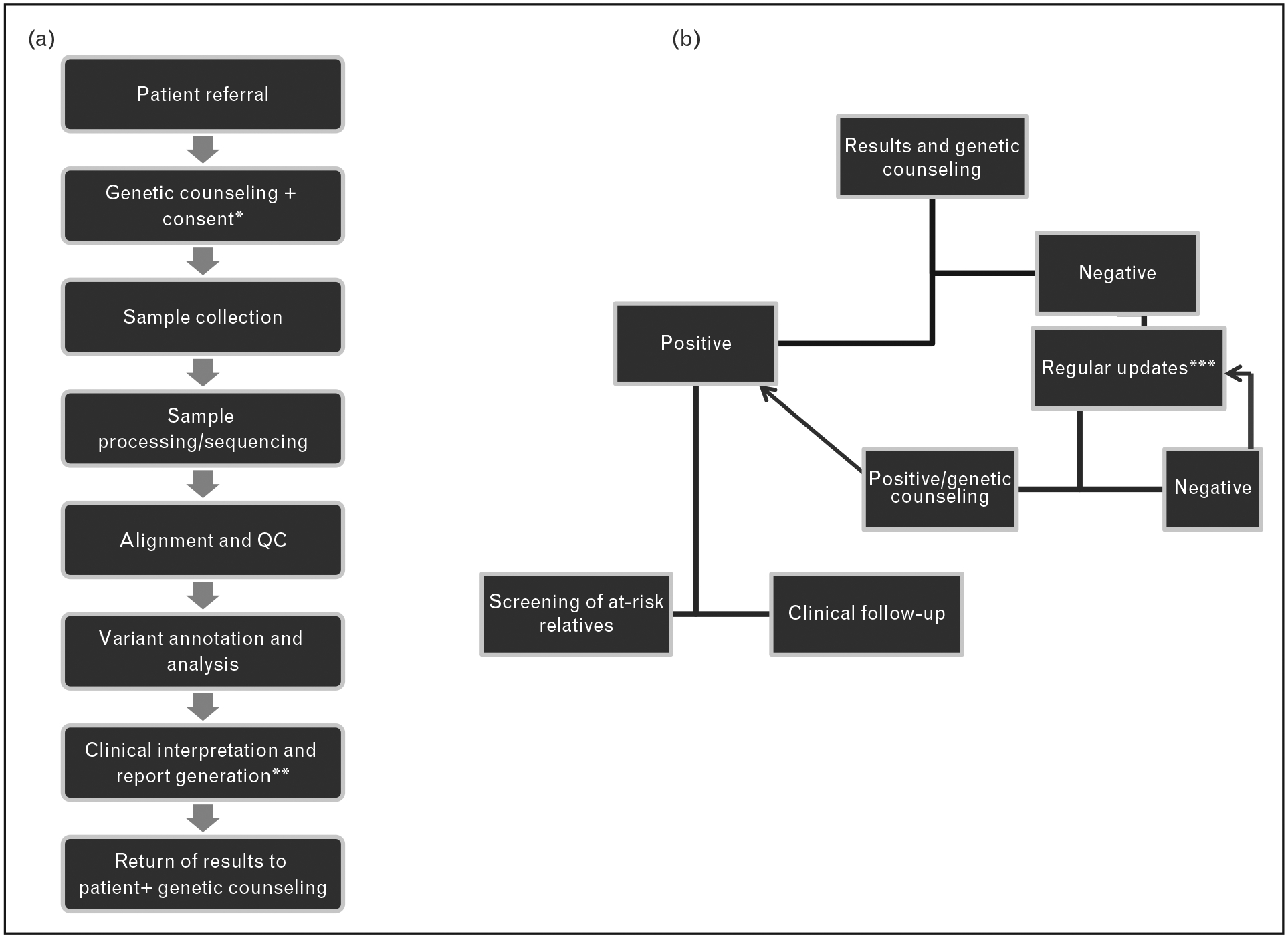
Proposed workflow of a genome-wide next-generation sequencing-based screen of patients with pheochromocytoma or paraganglioma. (a) Initial steps of the screening process involve genetic counseling and informed consent (apatient must opt in or out of ‘incidental finding’ reporting and decisions of future evaluation of the collected sequence data for future updates – see text for additional details). bIt is suggested that the final report be the consensus interpretation of physicians, researchers and clinical geneticists. (b) Results are returned to the patient at a genetic counseling session. Unquestionably, positive results follow the current route of clinical follow-up for index patient and screening of at-risk relatives. Negative results may include lack of a clearly pathogenic mutation in a known susceptibility gene or detection of variants of unknown significance (VUS). Regular updates on the status of VUS or evaluation of novel susceptibility genes from collected data are performed. If a new pathogenic variant is detected or pathogenic status of VUS is established, based on new research data, the patient will be offered genetic counseling and follow procedures for a ‘positive’ mutation carrier. If there are no changes in the genetic screening status, the process of regular updates may continue.