

Abstract
The coexistence of low back pain (LBP) and temporomandibular disorder (TMD) has often been noted clinically. However, studies of the association between these two conditions involving a large population with longitudinal evidences are lacking. Therefore, the study aimed to investigate the association between LBP and TMD in a nationwide-matched cohort population with a 15-year follow-up.
Data of 65,121 patients newly diagnosed with LBP were analyzed, along with those of 195,363 (1:3) sex- and age-matched controls. Multivariate Cox regression analysis was used to determine TMD risk between the LBP and non-LBP groups. Kaplan-Meier method was used for determining the cumulative risk of first-onset TMD between groups, with a 15-year follow-up.
The LBP group was more likely to develop first-onset TMD (adjusted hazards ratio (HR) = 1.561, P < .001), after adjusting for demographic variables and comorbidities. The risk factors for TMD were LBP, young age, higher insured premium, and osteoporosis. In the subgroup analysis, the LBP group had a higher risk of TMD than the non-LBP group in all stratifications.
LBP is the risk factor contributing to the development of first-onset TMD. Therefore, clinicians should be reminded to manage LBP disorders concurrently when treating TMD.
Keywords: first-onset temporomandibular disorder, low back pain, National Health Insurance Research Database
1. Introduction
Temporomandibular disorders (TMD) are complex and multifactorial diseases. The common signs and symptoms of TMD are orofacial pain, clicking or crepitus of the temporomandibular joints (TMJ), limited mandible movement, and deviation from the midline during movement.[1,2] Besides local TMJ pain, TMD is often associated with simultaneous pain in the head, neck, and back areas. The evidence from clinical and epidemiologic studies shows that TMD coexists with numerous systemic disorders including fibromyalgia, low back pain (LBP), spinal pain, chronic fatigue syndrome, irritable bowel syndrome, sleep disorders, tension-type and migraine headaches, and allergic conditions.[3,4,5] TMD seems to be of multifactorial etiology, including parafunctional habits, bruxism, deleterious body posture, occlusal features, trauma, overload, and stress[6,7,8]; hence, TMD is not easy to cure. Owing to the complexity of the symptoms and etiology, many patients with TMD cannot be appropriately treated according to the cause of the disease.
In fact, LBP and TMD often coexist in clinical practice. If we treat patients focusing on the TMJ only, the symptoms will easily recur. This reminds us that we should determine the cause of the condition in advance or manage comorbidities simultaneously. Previous studies have documented a significant association between LBP and TMD.[4,5,9,10] In 2000–2005 US National Health Interview Survey, 64% of 189,977 patients with TMD reported LBP.[4] Wiesinger et al.[9] reported significant associations between back pain and musculoskeletal disorders in the jaw or face and indicated the comorbidity between these two conditions. However, these investigations were only cross-sectional studies; studies involving a large population with longitudinal evidences are limited. Moreover, data on the possible mechanism linking LBP to TMD are lacking.
LBP is the most common musculoskeletal condition affecting the adult population, and >70% of the population has experienced acute episode of LBP at some point in their lives.[11] The common causes of LBP include muscle strain, herniated intervertebral disc, degenerative joint, sacroiliitis, spinal stenosis, sciatica, and other unspecified back disorders.[12,13,14] If LBP and TMD occur concurrently, functional activities would be mostly affected. Therefore, early prevention of TMD occurrence as comorbidity in patients with LBP is important, to avoid the profound functional limitation. To achieve that, this study aimed to investigate the association between LBP and first-onset TMD and to determine the possible mechanism linking these two diseases, using the Taiwan's National Health Insurance Research Database (NHIRD) with a 15-year follow up.
2. Methods
2.1. Data sources and ethics
Data retrieved from the 2000–2015 Longitudinal Health Insurance Database, a subset of Taiwan's NHIRD, were used in this study to investigate the association between LBP and TMD over a 15-year period. The NHIRD comprises comprehensive data on disease diagnoses coded by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)[15]; treatments and procedures; service dates; patients’ demographic characteristics; and drug prescriptions. The NHIRD is strictly used for research purposes, and all personally identifiable information is encrypted before being released to researchers to maintain patients’ confidentiality. The National Health Insurance program was launched in Taiwan in 1995 and, as at June 2009, included contracts with 97% of healthcare providers, with approximately 23 million beneficiaries or >99% of the entire population. Several studies have shown the accuracy and validity of diagnoses in the NHIRD.[16,17] This study received approval from the Tri-Service General Hospital (IRB No.2-103-05-043). Since the patient identifiers were encrypted to protect patient confidentiality before the data were used for research purposes, the requirement for patient written or verbal consent was waived.
2.2. Study design and sample population
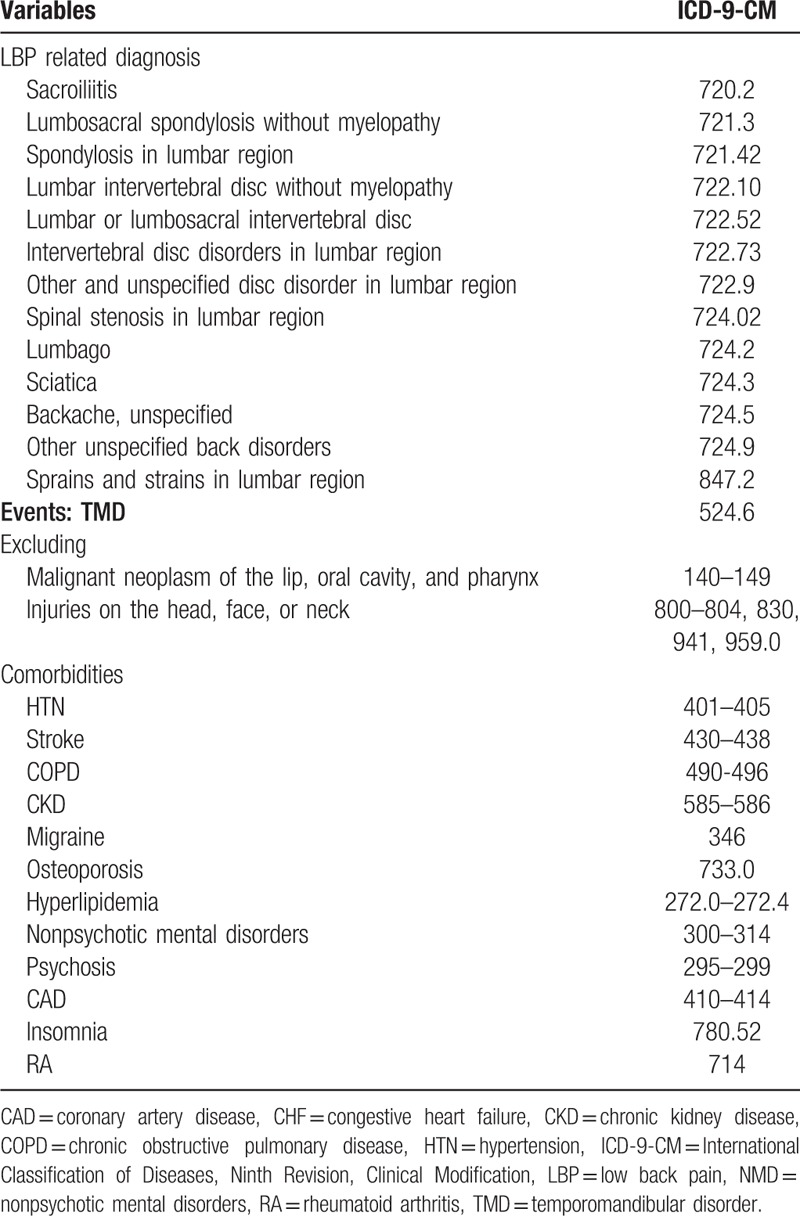
This retrospective matched-cohort study analyzed patients with LBP-related diagnosis from January 1, 2000 to December 31, 2004 according to the following ICD-9-CM codes: 720.2, 721.3, 721.42, 722.10, 722.52, 722.73, 722.9, 724.02, 724.2, 724.3, 724.5, 724.9, and 847.2 (Table 1).[18,19] Each enrolled LBP patient was required to have made at least six outpatient visits or one inpatient visit. All diagnoses of LBP were made by a board-certified rehabilitation, orthopedics, neurology, neurosurgery, and orthopedic doctor. For each patient with LBP, three patients without LBP, who were matched for sex, age, medical visits, and index year, were allocated to the comparison group. A total of 260,484 patients (study group, n = 65,121; comparison group, n = 195,363) were enrolled in this study. Both groups were followed-up from the index date until the onset of TMD, withdrawal from the NHI program, or the end of 2015. The diagnosis of TMD was based on the ICD-9-CM code 524.6, which was adapted from previous studies,[6,20,21] and has been used widely in population studies. All diagnoses of TMD were included at least 1 year after the LBP diagnosis and confirmed by board-certified rehabilitation physicians or dentists according to the physical examination or imaging findings, including three groups of the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD).[22]
Table 1.
Diagnosis groups with corresponding ICD-9-CM codes.
The flowchart of the study sample selection process is presented in Figure 1.
Figure 1.
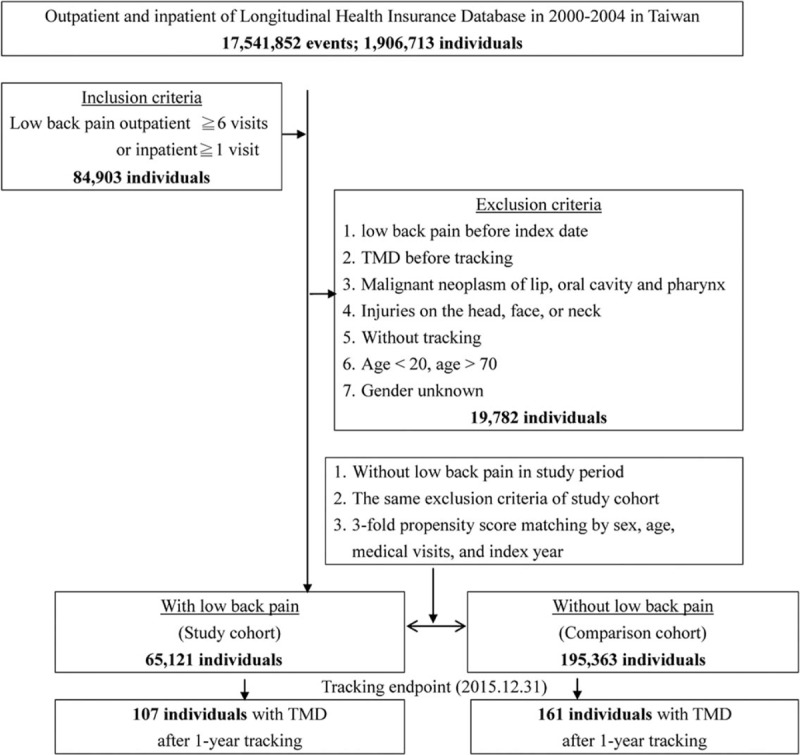
Flowchart of study sample selection from the National Health Insurance Research Database in Taiwan.
2.3. Exclusion criteria and comorbidities
Patients diagnosed with
-
(1)
LBP and TMD before 2000 (or LBP prior to the first visit for TMD);
-
(2)
those with diseases and injuries that may involve the temporomandibular joint (details provided in Table 1);
-
(3)
those aged <20 years or >70 years; and
-
(4)
those with unknown sex were all excluded from the study.
Associated systemic diseases and risk factors for TMD were analyzed to compare the effect of these confounding factors between the two groups.[6,23,21] Comorbidities were identified using the ICD-9-CM diagnosis codes, and detailed information was shown in the Table 1.
2.4. Statistical analysis
All analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY). The chi-square test and t test were used to statistically examine the differences between the two cohorts. Multivariate Cox regression analysis was performed to determine the risk of TMD, with the results of the analysis presented as hazards ratio (HR) with 95% confidence interval (CI). The difference in the risk of TMD between the study and comparison groups was estimated using Kaplan-Meier analysis with the log-rank test. A two-tailed P value <.05 was considered statistically significant.
3. Results
3.1. Sample characteristics
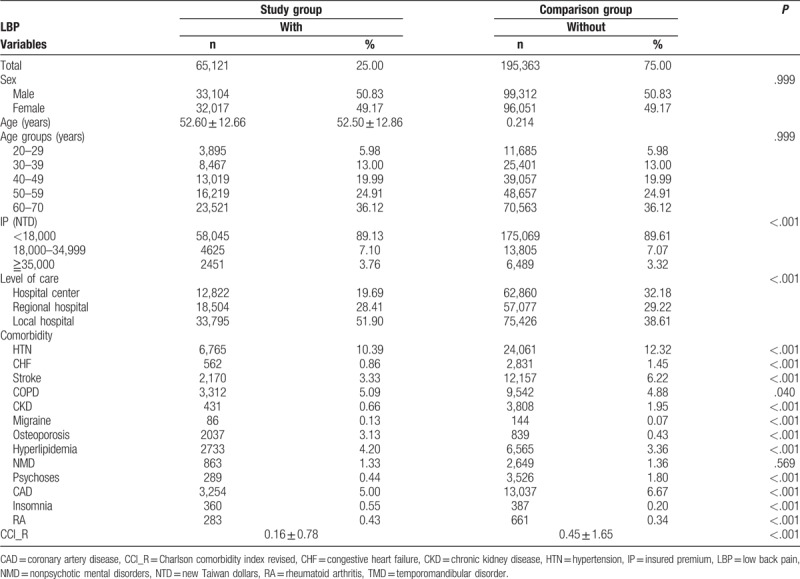
The characteristics of the study participants are presented in Table 2. There were no significant differences between the study and comparison groups in terms of sex, age, and comorbidity such as nonpsychotic mental disorders. There were significant differences in the insured premium (IP), level of care, and most of the comorbidities, such as hypertension, diabetes mellitus, congestive heart failure, stroke, chronic obstructive pulmonary disease, chronic kidney disease, migraine, osteoporosis, hyperlipidemia, nonpsychotic mental disorders, psychoses, coronary artery disease, insomnia, rheumatoid arthritis, and Charlson comorbidity index revised (CCI_R) between the study and control groups.
Table 2.
Characteristics of the study and comparison group at baseline.
3.2. Kaplan–Meier analysis of the cumulative risk for TMD
The LBP group showed a significantly higher cumulative risk of TMD than the non-LBP group (log-rank P < .001). The cumulative risk of TMD became significantly different between the 2 groups since the tenth year of tracking (Fig. 2). We divided the follow-up duration into 3 periods and found that the difference became significant since the 6 to 10-year period and became more significant as the LBP became more chronic (Table 3).
Figure 2.
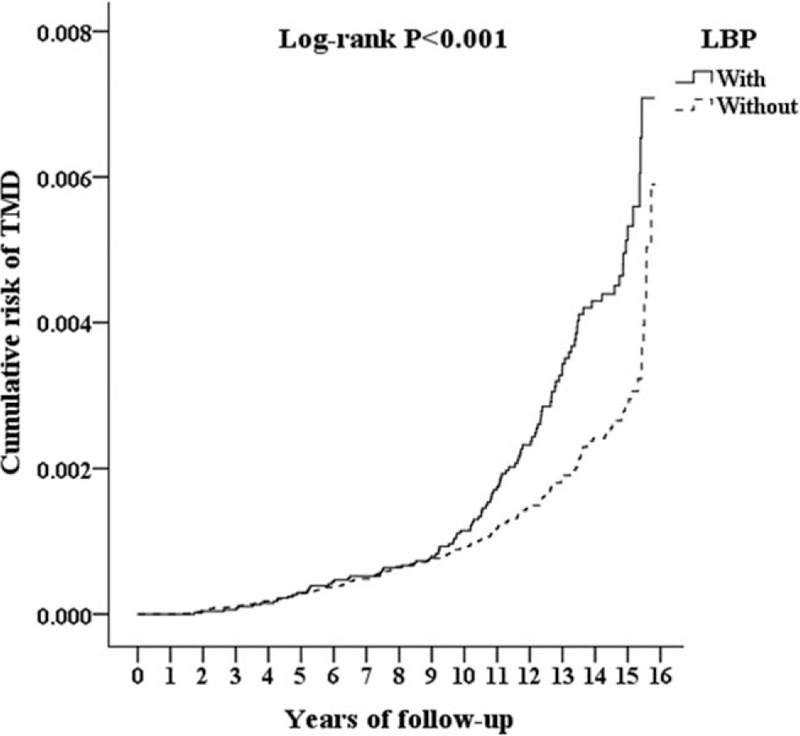
Kaplan-Meier for cumulative risk of first-onset TMD in patients aged 20 to 70 years stratified by low back pain with log-rank test. LBP = low back pain, TMD = temporomandibular disorder.
Table 3.
Risk of temporomandibular disorder among different tracking year.

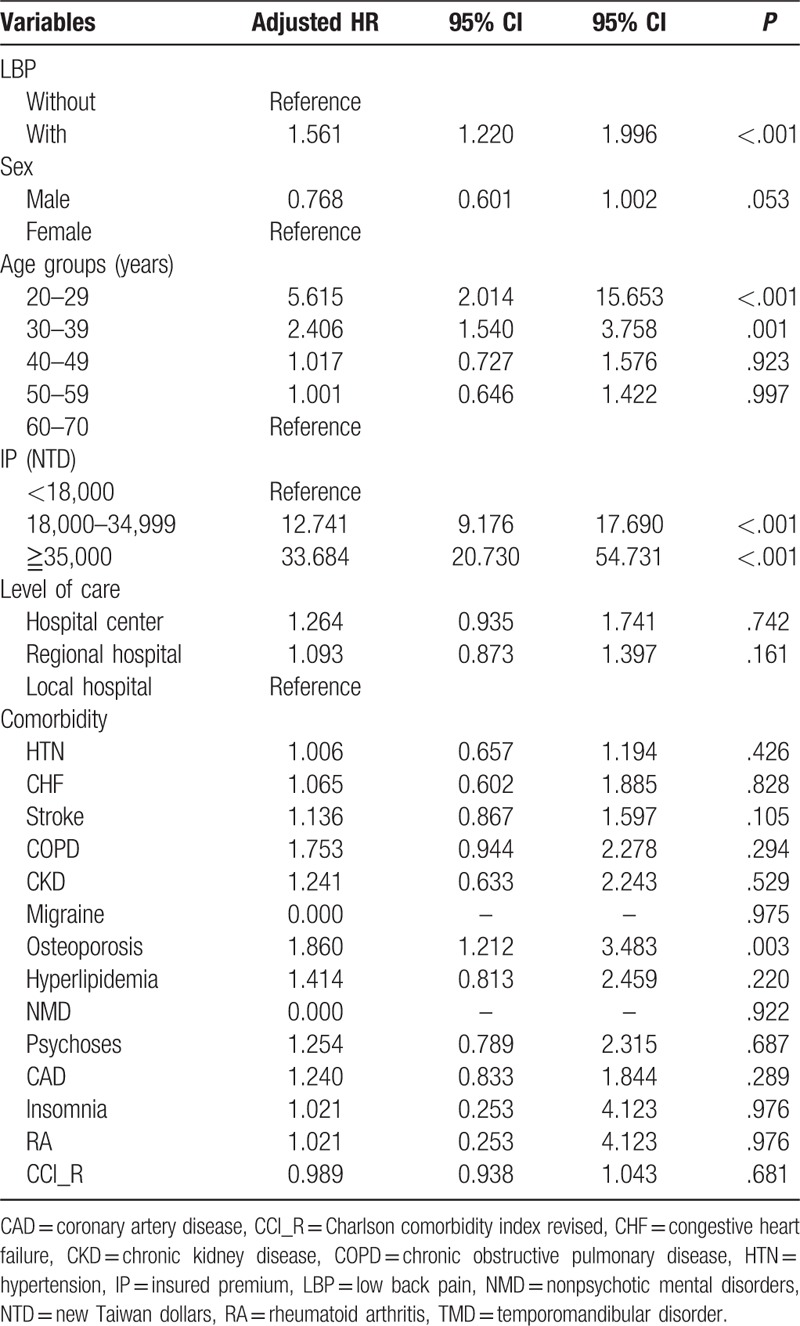
3.3. Factors for the incidence of TMD in the Cox regression analysis
The Cox regression analysis showed that the adjusted HR for the development of TMD was 1.561 times greater in the LBP group than in the non-LBP group (95% CI: 1.220–1.996, P < .001), after adjusting for demographic variables and comorbidities.
There was a higher risk of TMD in younger patients than in older patients (60–70 years) [adjusted HR for 20–29 years = 5.615, P < .001; for 30–39 years = 2.406, P = .001]. Moreover, those with higher IP showed a higher incidence of TMD than those with lower IP [adjusted HR for 18,000–34,999 NT = 12.741 (P < .001), for ≧35,000 NT = 33.684 (P < .001)]. Moreover, osteoporosis was also a risk factor contributing to TMD occurrence (adjusted HR = 1.860, P = .003) (Table 4).
Table 4.
Risk Factors for the incidence of TMD in the Cox regression analysis.
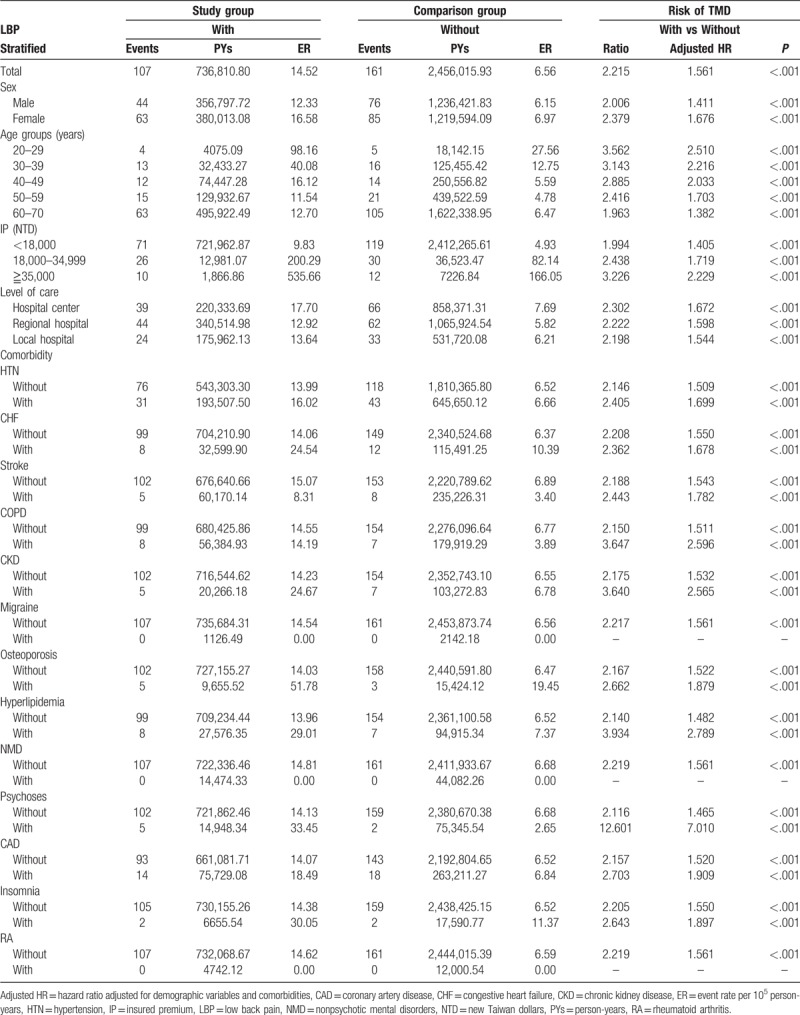
3.4. Risk of TMD between the study and comparison groups stratified by variables and comorbidities
The LBP group had a higher risk of TMD occurrence than the non-LBP group in all stratifications (Table 5).
Table 5.
Risk of temporomandibular disorder between study group and comparison group stratified by variables and comorbidities.
4. Discussion
Based on the results, the overall adjusted HR of TMD occurrence in the LBP group was 1.561 (95% CI: 1.220–1.996, P < .001) after adjusting for demographic variables and comorbidities. In other words, the patients with LBP had a 1.561-fold increased risk of developing first-onset TMD than the patients without LBP. The subgroup analysis stratified by demographic variables and comorbidities also revealed a higher risk of TMD in the LBP group than in the non-LBP group in all stratifications. It indicated LBP as a strong risk factor contributing to the occurrence of first-onset TMD. To the best of our knowledge, this is the first report that investigated the association between LBP and the risk of developing first-onset TMD through a nationwide population-based cohort study, with 15 years of follow-up. The study results support previous cross-sectional observations of comorbidity relationship between LBP and TMD.[4,5,9,10] However, their results only demonstrate the coexistence of LBP and TMD, but not that LBP may contribute to the development of first-onset TMD, as reported in the present study with 15-year follow-up. In the cumulative risk of TMD, we found that the difference between LBP and non-LBP groups became significant since the 6–10-year follow-up (Table 3), indicating that when LBP became more chronic, the occurrence of TMD would be more obvious.
Patients with LBP usually reveal problems in the lumbar spine and in the pelvic and hip joints.[24] A recent electromyography study demonstrated that cervical postural muscles (deep neck flexors) were more difficult to recruit in non-neutral spinal lumbopelvic alignment than in a neutral posture.[25] Therefore, problems in the lumbar-pelvis-hip (LPH) complex will affect the normal coordination of the neck muscle. Fink et al[26] proposed the functional relationships between the craniomandibular system, cervical spine, and the sacroiliac joint. Another study also documented that LBP might be associated with an increased incidence of neck pain.[27] Moreover, TMD was already confirmed to be related to cervical pain or upper quarter dysfuntion.[28,29] El-Hamalawy[30] reported that the forward head movement correction can improve myogenic temporomandibular joint dysfunction. Seagreen reported that tensed muscles around the head and neck would induce TMD symptoms.[31] Therefore, problems in the LPH complex can affect the head and neck, subsequently causing temporomandibular joint dysfunction. This may explain why patients with LBP would develop first-onset TMD, and the trend became obvious with chronic LBP of >6 years. However, the real mechanism of LBP triggering TMD still needs further investigation.
Regarding the factors affecting the incidence of first-onset TMD, patients with younger age, higher IP, and osteoporosis have an increased risk of first-onset TMD. There was a higher risk of TMD in the 20–29- and 30–39-year-old groups than in the other age groups. The age prevalence was similar to those reported in other studies.[2,32] Gonçalves et al[2] reported that the age groups with the largest proportion of first-onset TMD were the 31–40-year-old and 21–30-year old age groups (21.3% and 20.2%, respectively). In Aggarwal et al's study, patients aged 18 to 35 years were significantly more likely to report new oral facial pain at the 2-year follow-up than those aged 64 to 75 years.[32] Stress factors and low adaptive capacity might explain why young people were most affected.[33] The finding could be supported by other data from our results in the present study, indicating that those with middle (18,000–34,999 NT) and high (≥35,000 NT) IP showed a high risk of TMD occurrence. In the Taiwan NHI Program, a higher IP may indicate a higher socioeconomic status, which may be associated with higher stress. Stress is usually related to the presence of TMD pain that may be due to increased activity of the masticatory muscles, which is a compensatory reaction to stress.[8,34] Contrarily, a Brazilian study reported that poor economic class was significantly associated with the diagnosis of TMD.[35] However, another US study showed that the socioeconomic measures were not significantly associated with TMD incidence in their participants.[36]
Our data showed that osteoporosis is a risk factor contributing to TMD development in patients with LBP. Previous studies proposed that subchondral bone loss or osteoporotic changes in the temporomandibular joint may account for the high risk of TMD occurrence in LBP patients when combined with osteoporosis.[37–40] With regard to the association between osteoporosis and the occurrence of TMD, osteoporosis may induce bone loss in both the condyle and temporal components of the TMJ and impede the functional harmony of the masticatory system, increasing the occurrence of TMD.[39,40] In addition, our results indicate that migraine is not a risk factor for TMD development. Although some previous studies[41–43] reported that migraine is a common symptom in TMD individuals, they only proposed a comorbidity relationship between migraine and TMD according to cross-sectional evidence, using TMD questionnaires or physical examination. However, our cohort study demonstrated that there was no cause–effect relationship between migraine and TMD with 15 years of follow-up. This may be because the prevalence of migraine was significantly higher in individuals with myofascial TMD than in those with non-myofascial TMD.[44,45] However, myofascial TMD only involves group I of RDC/TMD, and our study enrolled three groups of RDC/TMD. Therefore, the cause–effect relationship between myofascial TMD and migraine needs to be further investigated with a longitudinal follow-up.
The event rate of TMD in the present study is lower than that in other studies,[3,10] which may be due to the following reasons. First, this study had stricter inclusion criteria such as TMD patients with identification ICD-9 code of 524.6 confirmed by doctors during outpatient or inpatient visits. Many previous studies only included patients who responded to a questionnaire or telephone interview.[3,4,10,36] The real incidence of TMD in the Taiwan population was much higher than that found in medical records, because many patients with TMD did not seek medical treatment. Moreover, the difference in ethnicity should also be taken into consideration.[4,10]
4.1. Limitations and strengths
There are several limitations in this study. First, there are many etiologies of LBP, but our study only analyzed the most common related diagnosis. Otherwise, data on pain severity, laboratory parameters, and radiologic images were not available in the NHIRD; thus, we could not classify the severity of LBP among the enrolled participants. Second, the actual prevalence of TMD might have been underestimated in the NHIRD, because some symptoms associated with TMD are often observed in other diseases, resulting in confusion or misdiagnosis.
Moreover, the major strength of our study is that we used data based on clinical diagnosis, which enabled a reliable cohort assessment. Furthermore, our longitudinal cohort study could overcome the major limitation of cross-sectional and case-control study designs by only providing information on disease incidence.
5. Conclusion
LBP is a risk factor contributing to the development of first-onset TMD. Therefore, for appropriate TMD management, clinicians should be reminded to manage both LBP disorders and TMD concurrently, especially among individuals presenting with associated risk factors, such as age 20 to 39 years, high IP, and osteoporosis.
Author contributions
Data curation: Wu-Chien Chien, Chi-Hsiang Chung, and Kuei-Chen Lee.
Funding acquisition: Wu-Chien Chien, Yi-Shing Shieh, and Kuei-Chen Lee.
Methodology: Wu-Chien Chien, Kuei-Chen Lee, and Yi-Shing Shieh.
Project administration: Yung-Tsan Wu and Liang-Cheng Chen.
Software: Chi-Hsiang Chung.
Supervision: Yung-Tsan Wu and Liang-Cheng Chen.
Writing – original draft: Kuei-Chen Lee and Yung-Tsan Wu.
Writing – review & editing: Yung-Tsan Wu, Wu-Chien Chien, and Yi-Shing Shieh.
Footnotes
Abbreviations: CCI_R = Charlson comorbidity index revised, CI = Confidence interval, HR = Hazard ratio, ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification, IP = Insured premium, LBP = Low back pain, LPH = Lumbar pelvis hip, NHIRD = National Health Insurance Research Database, RDC = Research Diagnostic Criteria, TMD = Temporomandibular disorder, TMJ = Temporomandibular joint.
How to cite this article: Lee KC, Wu YT, Chien WC, Chung CH, Chen LC, Shieh YS. The prevalence of first-onset temporomandibular disorder in low back pain and associated risk factors: A nationwide population-based cohort study with a 15-year follow-up. Medicine. 2020;99:3(e18686).
This work was supported by the Tri-Service General Hospital Research Foundation (Grant Reference Numbers TSGH-C105-012, TSGH-C106-010, TSGH-C107-183, TSGH-C108-003, and TSGH-C108-005-006-006-S03).
The authors have no conflicts of interest to disclose.
References
- [1].Inglehart MR, Patel HM, Widmalm SE, et al. Self-reported TMJD symptoms, oral health and quality of life of children in kindergarten through grade 5: does gender, race, and socio-economic background matter? J Am Dent Assoc 2016;147:131–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Gonçalves DA, Dal Fabbro AL, Campos JA, et al. Symptoms of temporomandibular disorders in the population: an epidemiological study. J Orofac Pain 2010;24:270–8. [PubMed] [Google Scholar]
- [3].Sanders AE, Slade GD, Bair E, et al. General health status and incidence of first-onset temporomandibular disorder: the OPPERA prospective cohort study. J Pain 2013;14:T51–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Plesh O, Adams SH, Gansky SA. Temporomandibular joint and muscle disorder (TMJMD) – type pain and co-morbid pains in a national US sample. J Orofac Pain 2011;25:190–8. [PMC free article] [PubMed] [Google Scholar]
- [5].Wiesinger B, Malker H, Englund E, et al. Does a dose-response relation exist between spinal pain and temporomandibular disorders? BMC Musculoskelet Disord 2009;10:28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Liao CH, Chang CS, Chang SN, et al. The risk of temporomandibular disorder in patients with depression: a population-based cohort study. Community Dent Oral Epidemiol 2011;39:525–31. [DOI] [PubMed] [Google Scholar]
- [7].Furquim BD, Flamengui LM, Conti PC. TMD and chronic pain: A current view. Dental Press J Orthod 2015;20:127–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Reissmann DR, John MT, Schierz O, et al. Stress-Related adaptive versus maladaptive coping and temporomandibular disorder pain. J Orofac Pain 2012;26:181–90. [PubMed] [Google Scholar]
- [9].Wiesinger B, Malker H, Englund E, et al. Back pain in relation to musculoskeletal disorders in the jaw-face: a matched case–control study. Pain 2007;131:311–9. [DOI] [PubMed] [Google Scholar]
- [10].Sipilä K, Suominen AL, Alanen P, et al. Association of clinical findings of temporomandibular disorders (TMD) with self-reported musculoskeletal pains. Eur J Pain 2011;15:1061–7. [DOI] [PubMed] [Google Scholar]
- [11].Allegri M, Montella S, Salici F, et al. Mechanisms of low back pain: a guide for diagnosis and therapy. F1000Res 2016;5:F1000.Faculty Rev-1530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].De Palma MJ, Ketchum JM, Saullo T. What is the source of chronic low back pain and does age play a role? Pain Med 2011;12:224–33. [DOI] [PubMed] [Google Scholar]
- [13].Jhun HJ, Park JY. Estimated number of Korean adults with back pain and population-based associated factors of back pain: data from the Fourth Korea National Health and Nutrition Examination Survey. J Korean Neurosurg Soc 2009;46:443–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Hestbaek L, Leboeuf-Yde C, Manniche C. Is low back pain part of a general health pattern or is it a separate and distinctive entity? A critical literature review of comorbidity with low back pain. J Manip Physiol Ther 2003;26:243–52. [DOI] [PubMed] [Google Scholar]
- [15].Chinese Hospital Association. ICD-9-CM English-Chinese Dictionary. Taipei: Chinese Hospital Association Press; 2000. [Google Scholar]
- [16].Ho Chan WS. Taiwan's healthcare report 2010. EPMA J 2010;1:563–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Cheng CL, Kao YH, Lin SJ, et al. Validation of the National Health Insurance Research Database with ischemic stroke ases in Taiwan. Pharmacoepidemiol Drug Saf 2011;20:236–42. [DOI] [PubMed] [Google Scholar]
- [18].Chia YY, Lo Y, Chen YB, et al. Risk of chronic low back pain among parturients who undergo cesarean delivery with neuraxial anesthesia: a nationwide population-based retrospective cohort study. Medicine (Baltimore) 2016;95:e3468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Chung YC, Hung CT, Li SF, et al. Risk of musculoskeletal disorder among Taiwanese nurses cohort: a nationwide population-based study. BMC Musculoskelet Disord 2013;14:144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Lin CY, Chung CH, Chu HY, et al. Prevalence of temporomandibular disorders in rheumatoid arthritis and associated risk factors: a nationwide study in Taiwan. J Oral Facial Pain Headache 2017;31:e29–36. [DOI] [PubMed] [Google Scholar]
- [21].Lee CF, Lin MC, Lin HT, et al. Increased risk of tinnitus in patients with temporomandibular disorder: A retrospective population-based cohort study. Eur Arch Otorhinolaryngol 2016;273:203–8. [DOI] [PubMed] [Google Scholar]
- [22].Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord 1992;6:301–55. [PubMed] [Google Scholar]
- [23].Huang GJ, LeResche L, Critchlow CW, et al. Risk factors for diagnostic subgroups of painful temporomandibular disorders (TMD). J Dent Res 2002;81:284–8. [DOI] [PubMed] [Google Scholar]
- [24].Shum GL, Crosbie J, Lee RY. Effect of low back pain on the kinematics and joint coordination of the lumbar spine and hip during sit-to-stand and stand-to-sit. Spine 2005;30:1998–2004. [DOI] [PubMed] [Google Scholar]
- [25].Falla D, O’Leary S, Fagan A, et al. Recruitment of the deep cervical flexor muscles during a postural-correction exercise performed in sitting. Man Ther 2007;12:139–43. [DOI] [PubMed] [Google Scholar]
- [26].Fink M, Wähling K, Stiesch-Scholz M, et al. The functional relationship between the craniomandibular system, cervical spine, and the sacroiliac joint: a preliminary investigation. Cranio 2003;21:202–8. [DOI] [PubMed] [Google Scholar]
- [27].Lee HY, Wang JD, Chang HL, et al. The association between asymmetric hip mobility and neck pain in young adults. J Manipulative Physiol Ther 2013;36:364–8. [DOI] [PubMed] [Google Scholar]
- [28].Walczyńska-Dragon K, Baron S. The biomechanical and functional relationship between temporomandibular dysfunction and cervical spine pain. Acta Bioeng Biomech 2011;13:93–8. [PubMed] [Google Scholar]
- [29].Chang TH, Duh DY, Lee MS, et al. Therapeutic effect of combining muscle relaxant and posture correction in patients with myofascial pain dysfunction syndrome of temporomandibular disorder. J Med Sci 2013;33:183–9. [Google Scholar]
- [30].El-Hamalawy FA. Forward head correction exercises for management of myogenic temporomandibular joint dysfunction. J Am Sci 2011;7:71–7. [Google Scholar]
- [31].Seagreen ME. An investigation into the relationship of myofascial trigger points in the head and neck region in association with temporomandibular joint dysfunction. [masters in technology: chiropractic dissertation]. Durban, South Africa: Durban University of Technology; 2009. in press. [Google Scholar]
- [32].Aggarwal VR, Macfarlane GJ, Farragher TM, et al. Risk factors for onset of chronic oro-facial pain--results of the North Cheshire oro-facial pain prospective population study. Pain 2010;149:354–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Mazzetto MO, Rodrigues CA, Magri LV, et al. Severity of TMD related to age, sex and electromyographic analysis. Braz Dent J 2014;25:54–8. [DOI] [PubMed] [Google Scholar]
- [34].Ohrbach R, Blascovich J, Gale EN, et al. Psychophysiological assessment of stress in chronic pain: Comparisons of stressful stimuli and of response systems. J Dent Res 1998;77:1840–50. [DOI] [PubMed] [Google Scholar]
- [35].Magalhães BG, de-Sousa ST, de Mello VV, et al. Risk factors for temporomandibular disorder: Binary logistic regression analysis. Med Oral Patol Oral Cir Bucal 2014;19:e232–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Slade GD, Bair E, Greenspan JD, et al. Signs and symptoms of first-onset TMD and sociodemographic predictors of its development: the OPPERA prospective Cohort Study. J Pain 2013;14:T20–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Dervis E. Oral implications of osteoporosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100:349–56. [DOI] [PubMed] [Google Scholar]
- [38].Chen K, Zhang N, Ding L, et al. Early intra-articular injection of alendronate reduces cartilage changes and subchondral bone loss in rat temporomandibular joints after ovariectomy. Int J Oral Maxillofac Surg 2014;43:996–1004. [DOI] [PubMed] [Google Scholar]
- [39].Gruber HE, Gregg J. Subchondral bone resorption in temporomandibular joint disorders. Cells Tissues Organs 2003;174:17–25. [DOI] [PubMed] [Google Scholar]
- [40].Klemetti E, Vainio P, Kroger H. Craniomandibular disorders and skeletal mineral status. Cranio 1995;13:89–92. [DOI] [PubMed] [Google Scholar]
- [41].Stuginski-Barbosa J, Macedo HR, Bigal ME, et al. Signs of temporomandibular disorders in migraine patients: a prospective, controlled study. Clin J Pain 2010;26:418–21. [DOI] [PubMed] [Google Scholar]
- [42].Goncalves DA, Camparis CM, Speciali JG, et al. Treatment of comorbid migraine and temporomandibular disorders: a factorial, double-blind, randomized, placebo-controlled study. J Orofac Pain 2013;27:325–35. [DOI] [PubMed] [Google Scholar]
- [43].Lopes SL, Costa AL, Gamba Tde O, et al. Lateral pterygoid muscle volume and migraine in patients with temporomandibular disorders. Imaging Sci Dent 2015;45:1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Dahan H, Shir Y, Nicolau B, et al. Self-reported migraine and chronic fatigue syndrome are more prevalent in people with myofascial vs nonmyofascial temporomandibular disorders. J Oral Facial Pain Headache 2016;30:7–13. [DOI] [PubMed] [Google Scholar]
- [45].Goncalves DA, Camparis CM, Speciali JG, et al. Temporomandibular disorders are differentially associated with headache diagnoses: a controlled study. Clin J Pain 2011;27:611–5. [DOI] [PubMed] [Google Scholar]