

Abstract
Social support (SS) is typically associated with lower emotional distress (e.g., stress and depression) in individuals. However, SS is a multifaceted construct that can vary by quality, quantity (amount), and type (i.e., it can be emotional or instrumental in nature).
Objectives:
The current study examined the relationships between characteristics of SS, stress, and depression in aging African-Americans.
Participants:
Analyses focused on data from 705 participants aged 22–92 years from the Carolina African American Twin Study of Aging.
Measurements:
Measures included the quality and quantity of emotional and instrumental support received, as well as stress and depression.
Design:
A series of univariate and increasingly complex multivariate regression models were conducted in MPlus (using the cluster option to control for family structure) to examine the relationships between SS and emotional distress variables.
Results:
Overall, better quality of emotional SS predicted fewer depression symptoms and less perceived stress, after controlling for age, gender, socioeconomic status variables, and the other subtypes of SS. However, more instances of emotional SS were associated with higher levels of perceived stress, depression symptoms, and more stressful life events within the past year. Likewise, more instrumental SS predicted more perceived stress, while holding the other variables constant.
Conclusions:
African Americans who experience more emotional distress report more SS, but the quality of emotional support appears to play an important role in the association between reduced levels of stress and depression. These findings suggest that interventions should include approaches to reduce emotional distress as well as enhance the quality SS.
Keywords: Depression, Stress, Social Support, African American
Objective
Social support (SS), the perception that a person is cared for, has access to help from other individuals, and is part of a supportive social network, enhances multiple aspects of physical health (1) and plays an important role in reducing stress and depression (2, 3). For instance, social isolation and low levels of SS have been associated with higher levels of depression (4) and stress (5) and poorer physical health outcomes (6, 7), whereas high levels of SS have been associated with improved outcomes following a variety of stressors (3). However, despite prior evidence of SS as a protective factor in psychological distress, the exact nature of their interplay remains unclear.
Heterogeneity in Social Support as a Construct
A notable challenge to understanding the effects of SS is that SS is often oversimplified by the aggregation of indices (e.g., appraisal, belonging, and tangible support or emotional and functional support into a total SS score). Clumping together these indices can obscure the relationships between components of SS and psychological distress and create heterogeneity across empirical studies. When SS is given or received, it can be in a variety of forms (e.g., emotional or material/instrumental). Consequently, the type of support received is another factor to consider when examining the effects of SS. Cutrona and Suhr (8) have suggested that there are five general social support categories: (a) informational, (b) emotional, (c) esteem, (d) social network support, and (e) tangible support. The current study focuses on emotional, informational, and tangible support. Emotional support reflects whether an individual has someone to confide in and receive sympathy from, while informational support deals with the ability to get advice and feedback from another person. Tangible/instrumental support focuses on whether an individual has someone to help with tasks he/she cannot do alone, such as moving furniture, transportation, or loans. Additionally, SS can be gauged by the amount received (i.e., quantity; number of interactions, number of supportive relationships, time) or perceived satisfaction (i.e., whether one felt their needs were met OR felt “better” after receiving support) with support received (9).
Heterogeneity in Social Support Across Racial/Ethnic Groups
Prior research suggests that the protective effects of SS can vary within the population, where groups with adverse health outcomes show the greatest benefits of SS. In a meta-analysis of studies on SS and diabetes, Strom and Egede (7) determined that the majority of adult populations that received SS experienced improved clinical outcomes, decreased mortality, and increased mental stability, regardless of race/ethnicity. However, differences were observed in the method of delivery and the source of SS among minority groups compared with non-Hispanic Whites (7). African-Americans engaged in more variable modes of SS (e.g. phone, group, and internet) and relied more on support from family and friends than from the media or healthcare professionals (7). Though disparities in stress, whether contextual (10), cultural, or race-related (11), may explain a greater need for SS to combat emotional distress and poorer health in African Americans (2, 4, 12, 13).
Previous research has primarily focused on how SS mediates the relationship between stressful life events and depression (14–16). Studies have found that increased SS reduces levels of depression after a stressful life event, but rarely address which properties of SS mediate this reduction. One study by Lincoln, Chatters and Taylor (17) suggests that SS from relatives was associated with lower psychological distress in African Americans but not in their White counterparts when controlling for personality, financials, and other factors. Compared to their White counterparts, African Americans may utilize social support somewhat differently, experience unique and additional stressors, have worse health outcomes because of emotional distress, and may benefit more from social support. Altogether, this underscores the need to develop a clearer understanding of the ameliorative components of SS in order to develop effective interventions to prevent and alleviate emotional distress in African Americans.
Current Study
The current study examines how different aspects of SS relate to phenotypes that indicate forms of emotional distress, as measured by perceived stress, depression symptoms, and number of stressful life events in a sample of African-Americans. While stressful life events are often conceptualized as external events that happen to an individual, a number of stressful life events can be considered dependent (i.e., brought about by the person’s actions and personality, such as divorce or an illness related to smoking habits) (18). While it would theoretically be possible to select out the “dependent” life events for analysis, our construct was not designed to do so. Additionally, external stressful life events are still by definition stressful, and SS could still vary in relation to the number of both dependent and external life events, therefore we kept all event types in our analysis.
Social support was decomposed into four components: quality of SS (e.g., how satisfied one is with their SS), quantity of SS (amount of SS), emotional SS (e.g., someone to talk to about worries) and instrumental SS (e.g., someone to provide help around the house). This more nuanced characterization of SS can help elucidate what qualities of SS help to reduce stress and depression. Quality and quantity are looked at separately because someone might receive a lot of poor-quality SS or very little high-quality SS and not receive the protective benefits one might expect. It is possible that instrumental SS might be more effective than emotional SS if an individual is under high financial strain. We hypothesized that better quality emotional and instrumental SS would predict lower levels of depression symptoms, perceived stress, and fewer stressful life events among African Americans. Additionally, we hypothesized that higher amounts of emotional and instrumental SS would be associated with reduced emotional distress.
Methods
Sample
The study consisted of 705 individuals from the Carolina African American Twin Study of Aging (CAATSA), which was approved by the Institutional Review Boards of the University of North Carolina Chapel Hill and Pennsylvania State University (19). Participants read and signed an informed consent prior to completing a 2.5-hour interview in their home. Information was read to the participant to reduce the possible effects of low education. Participants included members of twin pairs and siblings of twins. The sample was roughly 59% female (33% monozygotic twins, 22% opposite-sex twins, and 7% from twin-sibling pairs), ranging in age from 22–92 years (M = 49.86, SD =14.49). The mean level of education level was 12.76 (SD = 4.15) years, 61.5% reporting over $1500 in monthly income, and 67.8% employed at study inception. Other details about the sample, including identification, recruitment of the twins, and sample ascertainment are described previously (20).
Measures
Depression.
Depression symptom severity was measured using an abridged 11-item version of the Center for Epidemiologic Studies Depression scale (CES-D) which assessed depressed mood over the past week (20, 21) (Cronbach’s alpha of 0.79) (22).
Perceived Stress Scale.
The 14-item Perceived Stress Scale (23) was used to assess feelings of stress in the past month. Analyses were limited to 9 out of the 14 items, which had good reliability (Cronbach’s alpha of 0.78).
Stressful Life Events.
Stressful life events were measured with a checklist of 26 events that may have occurred in the past year. Participants indicated whether or not an event happened, and if it did happen, was it “of little importance,” “somewhat important,” or “very important.” Conflated importance of any particular event was minimized by using a simple count of the number of events for each participant (24).
Social Support (SS).
Past year social support was assessed using a set of questions adapted from Taylor (25) that included how frequently friends and family had helped with certain activities, such as household chores, given rides or money (i.e., instrumental), provided advice and/or discussed personal problems (emotional). Participants could indicate “never,” “rarely,” “sometimes,” “often,” or “no need.” Emotional and instrumental frequency items were separately averaged to get an overall quantity score for each form of SS. The second question asked participants to rate (on a 1 to 5 Likert scale) how satisfied (“not at all satisfied” to “extremely satisfied”) they were with received emotional and instrumental support, specifically “in terms of how they make you feel and how much it helps.” These latter items comprised the emotional quality and instrumental quality scores.
Covariates.
Covariates (see Table 1) included age at the time of the assessment (mean-centered), gender (male/female), and several indicators of socioeconomic status (SES; current work status, education level (mean-centered), and income). Participants who worked part time were considered currently working. Education level was defined as the highest grade completed in school. Income was current total gross family income per month and was binned into 16 categories ranging from under $100 to over $1500.
Table 1.
Descriptive Statistics of Participants in the CAATSA study
| Measure | Mean / Percentage | SD | Min | Max |
|---|---|---|---|---|
| Age | 49.86 | 14.59 | 22 | 92 |
| Gender (Female = 1) | 59% | - | 0 | 1 |
| Work Status (currently working = 1) | 68% | - | 0 | 1 |
| Education Level | 12.76 | 4.15 | 0 | 77 |
| Monthly Income | 12.54 | 3.88 | 0 | 15 |
| Depression Symptoms | 6.12 | 5.54 | 0 | 30 |
| Perceived Stress | 11.75 | 6.07 | 0 | 35 |
| Life Events | 2.01 | 2.14 | 0 | 18 |
| Emotional Quality | 2.92 | 1.03 | 0 | 4 |
| Emotional Quantity | 1.69 | 0.95 | 0 | 3 |
| Instrumental Quality | 2.95 | 0.99 | 0 | 4 |
| Instrumental Quantity | 1.16 | 0.80 | 0 | 3 |
Note. CAATSA=Carolina African American Twin Study of Aging, SD = Standard Deviation, Min = Minimum, Max = Maximum.
Statistical Analyses
Analyses comprised of correlations between variables and then a series of increasingly complex linear regressions executed in MPlus (version 8). Robust standard errors were computed using the sandwich estimator to account for non-independence (i.e., family structure) using the cluster option. For the first set of regression analyses, each of the four SS variables was used to predict each indicator of psychological distress ignoring covariates. Next, we assessed the joint effects of all SS variables on each outcome (i.e., we fit a model where all forms of SS simultaneously predicted a given outcome). Third, we examined the effect of SS while controlling age and gender as covariates. We then expanded the model further by adding the set of SES measures as covariates for each outcome. Lastly, when there were main effects of SS on an outcome, it was followed up with a model testing for an interaction between the quality and quantity of that type of social support (emotional or instrumental; Interaction Model). Only tabled results for the models including covariates (i.e., full model) and interaction variables are presented. Results for the models using fewer or no covariates are available upon request.
Results
Table 2 shows the zero-order correlations among the indicators of emotional distress (i.e., depression, perceived stress, and stressful life events) variables and among the social support (SS) variables. Correlations (not adjusted for multiple testing) revealed that individuals with higher amounts of depression symptoms also reported elevated perceived stress. Severity of depression was also positively correlated with the number of stressful life events, but the effect was more limited in comparison to depression’s association with perceived stress. Stressful life events and perceived stress were uncorrelated in the current sample.
Table 2.
Pearson Correlations and between Emotional Distress and Social Support
| Measure | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Depression Symptoms | - | ||||||
| 2. Perceived Stress | .59** | - | |||||
| 3. Life Events | .12* | .05 | - | ||||
| 4. Emotional Quality | −.22** | − 24** | .02 | ||||
| 5. Emotional Quantity | .12** | .20** | .10** | .23** | - | ||
| 6. Instrumental Quality | −.14** | −.16** | .00 | .59** | .15** | - | |
| 7. Instrumental Quantity | .10* | .17** | .10* | .11** | .35** | .15** | - |
Note. N’s ranged from 697 to 705.
p <.05;
p <.01.
Among the predictor variables, quality of emotional and instrumental SS were strongly correlated, while quantity of emotional and instrumental SS were moderately correlated. Quality of SS and quantity of SS had small but significant relationships for emotional and instrumental types respectively, suggesting that if both were associated with emotional distress, it could be via separate and largely distinct mechanisms.
Effects of Social Support on Emotional Distress
As seen in previous studies, SS was related to emotional distress (Table 2). When not accounting for other subtypes of social support, generally, better quality social support was associated with lower emotional distress, while more social support (i.e., higher quantity) was associated with more emotional distress. This held true for both emotional and instrumental SS. It is important to note that the stated relationship was not observed for quantity of SS and stressful life events. When controlling for other types of SS and additional covariates (see Table 3), there was a clear pattern suggesting that emotional SS, but not instrumental SS, was associated with emotional distress. Notably, no relationship was observed between quality of emotional SS and stressful life events. Additionally, there was a small, positive relationship between the amount of instrumental support received and perceived stress. As seen with the correlations, higher satisfaction with emotional SS (i.e., quality of emotional SS) predicted fewer perceived stress and depression symptoms, but more emotional SS predicted more depression symptoms, perceived stress, and stressful life events; having received more instrumental SS only predicted more perceived stress.
Table 3.
Standardized Regression Results Showing Association between Social Support, Depression, Perceived Stress and Stress Life Events with Covariates
| Scale | Depression Symptoms | Perceived Stress | Life Events | |
|---|---|---|---|---|
| (n = 662) | (n = 661) | (n = 662) | ||
| β (SE) | β (SE) | β (SE) | ||
| Emotional | Quality | −0.25 (0.05)** | −0.28 (0.04)** | −0.02 (0.05) |
| Quantity | 0.15 (0.04)** | 0.22 (0.04)** | 0.13 (0.04)** | |
| Instrumental | Quality | −0.02 (0.05) | −0.05 (0.05) | −0.01 (0.05) |
| Quantity | 0.05 (0.04) | 0.08 (0.04)* | 0.03 (0.05) | |
| Age | −0.15(0.05)** | −0.14 (0.05)** | 0.02 (0.05) | |
| Gender | 0.04 (0.04) | 0.10 (0.04)** | −0.09 (0.04)* | |
| Income | −0.10 (0.05)* | −0.11 (0.05)* | 0.05 (0.05) | |
| Work Status | −0.04 (0.05) | −0.06 (0.05) | −0.09 (0.05) | |
| Education | −0.11 (0.05)* | −0.05 (0.06) | −0.01 (0.03) |
Note. Results shown for each predictor include the following covariates in the regression model: age, gender, socioeconomic status variables, and other types of social support; Standardized betas from z-tests are reported. SE = Standard Error.
p <.05.
p <.01.
Given the unique contributions of each form of SS to emotional distress, we fitted interaction models that provided deeper insight into the codependences that may be present, such that how much support a person received could be a function of the quality of the support being given. While most of our interaction models showed null results, our analysis of the effect of emotional SS on stressful life events revealed a significant quality-by-quantity interaction effect (see Table 4 for standardized effects). Specifically, individuals reporting having experienced more stressful life events, and average quality emotional SS, received more than average amounts of emotional SS. However, if a person received higher quality SS, they generally received it relatively less frequently (B = −.18, SE = .07, z =−2.60, p =.009; β= −.31, SE = .12, z = −2.66, p = .008; see Figure 1).
Table 4.
Multiple Regression Models of Social Support Predicting Emotional Distress Including Interaction Terms for Quality by Quantity of Social Support
| Model 1 | Life Events (n=551) | Perceived Stress (n=571) | Depression Symptoms (n = 662) | Model 2 | Life Events (n=551) | Perceived Stress (n = 571) | Depression Symptoms (n = 662) | ||
|---|---|---|---|---|---|---|---|---|---|
| β(SE) | β(SE) | β(SE) | β(SE) | β(SE) | β(SE) | ||||
| Emo | Quality | 0.11 (0.07) | −0.18 (0.06) | −0.26 (0.08) | Emo | Quality | 0.00 (0.06) | −0.24 (0.05) | −0.25 (0.05) |
| Quantity | 0.37 (0.10) | 0.34 (0.10) | 0.13 (0.11) | Quantity | −0.12 (0.10) | −0.02 (0.07) | −0.08 (0.09) | ||
| Inst | Quality | −0.01 (0.05) | −0.08 (0.05) | −0.02 (0.05) | Inst | Quality | 0.09 (0.05) | 0.09 (0.04) | 0.09 (0.04) |
| Quantity | 0.03 (0.05) | 0.06 (0.04) | 0.05 (0.04) | Quality | −0.15 (0.18) | 0.21 (0.12) | −0.11 (0.16) | ||
| Emo Interaction | −0.31 (0.12)* | −0.15 (0.12) | 0.03 (0.13) | Inst Interaction | 0.23 (0.19) | -0.17 (0.13) | 0.18 (0.17) | ||
Note. SE = Standard Error; Emo = Emotional; Inst = Instrumental; Age, gender, socioeconomic status variables, and other types of social support included as covariates. Standardized betas from z-tests are reported.
p <.05
Figure 1.
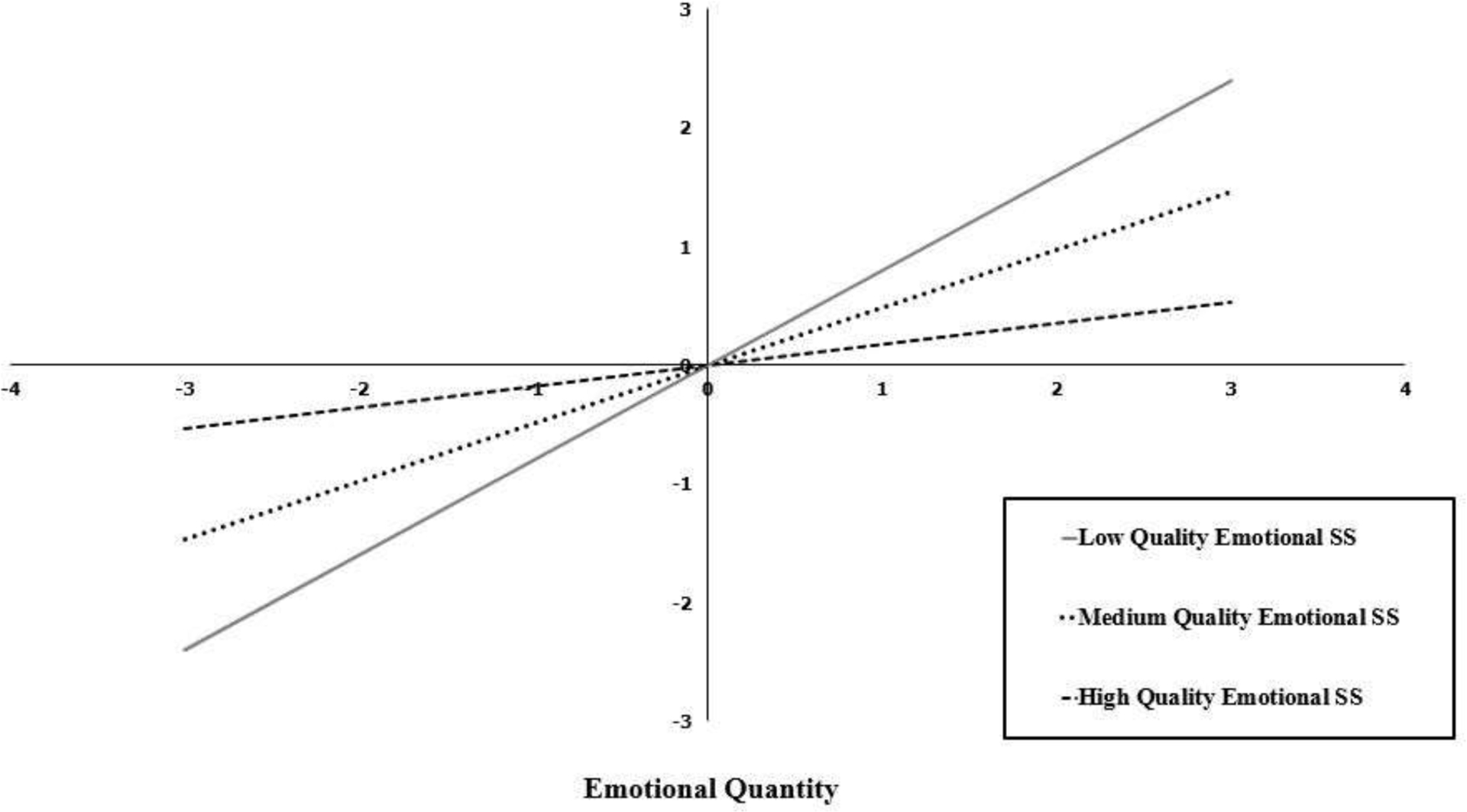
Interaction between emotional quality and emotional quantity social support on number of past year stressful life events.
Conclusions
The current study adds to our understanding of how different forms of SS are associated with emotional distress in African Americans. The study builds upon the previously discussed literature that examined SS as a unitary construct. This study distinguishes itself by deconstructing SS into four components to better understand how different aspects of SS relate to stress and depression in African-Americans. First, a distinction was made between the quantity and quality characteristics of SS to assess whether the frequency at which a person receives SS or whether the perceived satisfaction of SS plays a role in emotional distress. Furthermore, the added distinction between emotional and instrumental characteristics of SS allowed for us to ask whether having someone to talk to or whether receiving assistance with daily activities helps to alleviate emotional distress.
The four aspects of SS showed differential relationships with depression and stress. With respect to the multivariate model, participants reported receiving higher amounts of emotional SS when they had higher stress levels and more depression symptoms; often translating to roughly one-half to two symptoms being endorsed by each participant. This was somewhat surprising given the previous body of literature, which demonstrated SS (broadly defined) was associated with lower levels of stress and depression (1, 12, 26). We hypothesize that this may be due to individuals seeking out or evoking more SS, regardless of the type, when the need is greater, as suggested by the relationship between a high number of stressful life events with stress and depression. However, further research must be done in order to disentangle this relationship and to determine if this relationship is specific to this African American sample or if it would replicate in other populations as well. Unfortunately, due to the cross-sectional design of this study, which is based on between-person-differences, we cannot distinguish between whether social support led to changes in perceived distress or whether the experienced distress led to different experiences of support and the actual amount of support people received.
Quantity of emotional SS was also positively associated with stressful life events. However, the relationship between the amount of SS and stressful life events varied depending upon the quality of the SS. Such that, among individuals reporting relatively more occurrences of stressful life events, those who reported higher satisfaction with the level of emotional support given, received less frequent emotional SS, compared to those who only reported moderate satisfaction with the emotional support given, who seemed to need emotional SS more often. This could indicate that, in the presence of more stressful life events, individuals who are more satisfied with their emotional SS need less support.
We also found that high satisfaction with emotional support received in the past year was inversely related to recent depression and perceived stress, regardless of the amount of SS an individual received and the perceived quality of instrumental support; this roughly translated to at least one fewer symptoms endorsed. It is plausible that better quality social support reduces emotional distress, leading to better outcomes. This is supported by similar findings that perceived quality of relationships is a better predictor of well-being than quantity of relationships (3). Likewise, Wethington and Kessler (27) found the effect of SS on psychological distress to be more strongly linked to the perception of support (quality) than to the actual support behaviors (frequency). This study expands upon these previous results by controlling for other types of SS, revealing that an overall feeling of satisfaction with emotionally-supportive interactions has a lasting positive impact on emotional distress.
The potential clinical importance of these findings is particularly relevant to middle-aged and older individuals. Social support can often decrease with age given the increases in social isolation that can occur due to a variety of factors, such as health-related loss of mobility, loss of partners and friends due to death and relocation. Individual or group therapy would be ideal interventions for working on social skills and improving an individual’s ability to give and receive emotional social support, however, this is not always possible or appealing to an individual. Another strategy is to circulate tips, such as those provided by the American Psychological Association, on how to improve emotional connections (e.g., by reaching out first, or teaching individuals how to use technology to stay in touch (28). If older individuals maintain or foster a few relationships that have good quality social support, having fewer sources of social support may not have as large of an impact.
Limitations
There are several limitations when interpreting this body of work. First, we operationalized SS as individuals’ perceptions of the support received, potentially conflating his or her improved well-being and outlook, as suggested by less stress and depression, with feelings of satisfaction. Likewise, studies have suggested a relationship between depression symptoms and subsequent reductions in perceived SS may be attributable to depression symptoms themselves (29), as well as depression symptoms resulting from poor social relationships (30). Second, personality characteristics associated with depression, such as neuroticism, could negatively affect the evaluation of support availability. However, perceived support availability is not as strongly linked to emotional distress as perceived support (31).
Another limitation is the potential generalizability of the sample. For example, with age, intact pairs of twins are healthier in general. This comes from ascertaining participants who enter a sample by the nature that they have a living relative. The sample also includes younger adults who may have different reasons for SS than older adults. Their sources of stress and depression might also arise from sources different from older adults. Future examinations should collect enough participants across the lifespan to be sufficiently powered to stratify by age in order to see if there are systematic differences by age. Additionally, while there was a wide age range included in this sample, the majority of the sample was middle aged or older in the early 2000s, which might not generalize to a sample who can utilize the internet and social media more effectively. Similarly, additional forms of social support (such as from online social networks and informational support) were not adequately assessed; it is unclear if the results would generalize to forms for social support from those types of sources. Lastly, this sample did not include individuals from other racial groups, making comparisons to other racial groups difficult.
Future Directions
Satisfaction with SS seems to be a key component for reducing emotional distress, therefore we recommend that outreach and therapy practices teach individuals how to provide better quality SS themselves, as well as how to elicit better quality SS from friends and family. When possible, therapists could work directly with friends and family members to train them to provide higher quality emotional SS. Whenever possible, any intervention strategy should be tailored to the situation at hand, however, our findings suggest that engendering a broad sense of care and concern may reduce levels of emotional distress over and above other types of social support.
Thus far, interventions involving SS have targeted the provision of support, where adding or increasing the quantity of support has been met with mixed results (see (32) for a review). It appears that it is not primarily quantity of SS, but the recipients’ perception of, and satisfaction with, available support that is most strongly linked to emotional distress, which is consistent with our findings. Therefore, incorporating strategies to train an individual to strengthen his or her existing social support systems in multiple settings (e.g., primary health care, educational, and spiritual settings) may prove useful. Additionally, reframing the SS a person currently receives to be perceived more positively could reduce emotional distress. As mentioned previously, this could be particularly important for individuals at risk of socially isolation, such as the elderly. Future studies could collect a measure of social isolation and see if higher quality emotional social support still buffers against stress and depression in individuals who are more socially isolated.
Final Conclusions
The present results suggest that emotional distress is associated with both the quality and quantity of social support provided by friends and family. Notably, quality and not quantity of support is associated with less emotional distress, but quantity of support is associated with more distress. Taken together, these findings highlight the need for future research to parse these opposing processes of social support that may distinguish between the benefit of social support and the need for support, respectively.
Highlights.
The present study examined how the quality and quantity of emotional and instrumental social support relate to stress and depression among older African Americans.
Better quality emotional social support was associated with less stress and depression, while higher levels of stress and depression were associated with receiving more social support.
Improving quality of emotional social support may help to further reduce emotional distress.
Author Note:
This work was supported by the National Institute of Health’s National Institute on Aging grant (R01AG013662 [Whitfield] and K02AG059140 [Thorpe]), the National Institute on Minority Health and Health Disparities (NIMHD U54MD000214 [Thorpe]), and the National Institute on Drug Abuse (DP1DA042103; Palmer).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of interest: The authors have no conflicts to declare.
References
- 1.Heard E, Whitfield KE, Edwards CL, et al. : Mediating effects of social support on the relationship among perceived stress, depression, and hypertension in African Americans. J Natl Med Assoc 2011; 103:116–122 [DOI] [PubMed] [Google Scholar]
- 2.Kogan SM, Brody GH, Crawley C, et al. : Correlates of elevated depressive symptoms among rural African American adults with type 2 diabetes. Ethn Dis 2007; 17:106–112 [PubMed] [Google Scholar]
- 3.Southwick SM, Vythilingam M, Charney DS: The psychobiology of depression and resilience to stress: implications for prevention and treatment. Annual review of clinical psychology 2005; 1:255–291 [DOI] [PubMed] [Google Scholar]
- 4.Shim RS, Ye J, Baltrus P, et al. : Racial/Ethnic Disparities, Social Support, and Depression: Examining a Social Determinant of Mental Health. Ethnicity & disease 2012; 22:15–20 [PMC free article] [PubMed] [Google Scholar]
- 5.Mama SK, Li Y, Basen-Engquist K, et al. : Psychosocial Mechanisms Linking the Social Environment to Mental Health in African Americans. PLOS ONE 2016; 11:e0154035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cacioppo JT, Cacioppo S, Capitanio JP, et al. : The Neuroendocrinology of Social Isolation. Annual Review of Psychology 2015; 66:733–767 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Strom JL, Egede LE: The impact of social support on outcomes in adult patients with type 2 diabetes: a systematic review. Curr Diab Rep 2012; 12:769–781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cutrona CE, Suhr JA: Controllability of stressful events and satisfaction with spouse support behaviors. Communication Research 1992; 19:154–174 [Google Scholar]
- 9.Lakey B, Orehek E, Hain KL, et al. : Enacted Support’s Links to Negative Affect and Perceived Support Are More Consistent With Theory When Social Influences Are Isolated From Trait Influences. Personality and Social Psychology Bulletin 2009; 36:132–142 [DOI] [PubMed] [Google Scholar]
- 10.Giurgescu C, Misra DP, Sealy-Jefferson S, et al. : The impact of neighborhood quality, perceived stress, and social support on depressive symptoms during pregnancy in African American women. Social science & medicine (1982) 2015; 130:172–180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Utsey SO, Giesbrecht N, Hook J, et al. : Cultural, sociofamilial, and psychological resources that inhibit psychological distress in African Americans exposed to stressful life events and race-related stress. Journal of Counseling Psychology 2008; 55:49–62 [Google Scholar]
- 12.Dennis JP, Markey MA, Johnston KA, et al. : The Role of Stress and Social Support in Predicting Depression Among a Hypertensive African American Sample. Heart & lung : the journal of critical care 2008; 37:105–112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Strogatz DS, Croft JB, James SA, et al. : Social support, stress, and blood pressure in black adults. Epidemiology (Cambridge, Mass.) 1997; 8:482–487 [DOI] [PubMed] [Google Scholar]
- 14.Calvete E, Connor-Smith JK: Perceived social support, coping, and symptoms of distress in American and Spanish students. Anxiety, Stress & Coping: An International Journal 2006; 19:47–65 [Google Scholar]
- 15.Heard E, Whitfield KE, Edwards CL, et al. : Mediating Effects of Social Support on the Relationship Among Perceived Stress, Depression, and Hypertension In African Americans. Journal of the National Medical Association 2011; 103:116–122 [DOI] [PubMed] [Google Scholar]
- 16.Holahan CJ, Moos RH, Holahan CK, et al. : Social support, coping, and depressive symptoms in a late-middle-aged sample of patients reporting cardiac illness. Health Psychology 1995; 14:152–163 [DOI] [PubMed] [Google Scholar]
- 17.Lincoln KD, Chatters LM, Taylor RJ: Psychological distress among black and white Americans: differential effects of social support, negative interaction and personal control. Journal of health and social behavior 2003; 44:390–407 [PMC free article] [PubMed] [Google Scholar]
- 18.Bemmels HR, Burt SA, Legrand LN, et al. : The Heritability of Life Events: An Adolescent Twin and Adoption Study. Twin Research and Human Genetics 2008; 11:257–265 [DOI] [PubMed] [Google Scholar]
- 19.Whitfield KE, Brandon DT, Wiggins S, et al. : Does Intact Pair Status Matter in the Study of African American Twins? The Carolina African American Twin Study of Aging. Experimental Aging Research 2003; 29:407–423 [DOI] [PubMed] [Google Scholar]
- 20.Whitfield KE: A Registry of Adult African American Twins: The Carolina African American Twin Study of Aging. Twin Research and Human Genetics 2013; 16:476–480 [DOI] [PubMed] [Google Scholar]
- 21.Suthers KM, Gatz M, Fiske A: Screening for depression: A comparative analysis of the 11-item CES-D and the CIDI-SF, 2004
- 22.Cronbach LJ: Coefficient alpha and the internal structure of tests. Psychometrika 1951; 16:297334 [Google Scholar]
- 23.Cohen S, Kamarck T, Mermelstein R: A global measure of perceived stress. J Health Soc Behav 1983; 24:385–396 [PubMed] [Google Scholar]
- 24.Lei H, Skinner HA: A psychometric study of life events and social readjustment. Journal of Psychosomatic Research 1980; 24:57–65 [DOI] [PubMed] [Google Scholar]
- 25.Taylor RJ: The Extended Family as a Source of Support to Elderly Blacks1. The Gerontologist 1985; 25:488–495 [DOI] [PubMed] [Google Scholar]
- 26.Dean A, Kolody B, Wood P: Effects of Social Support from Various Sources on Depression in Elderly Persons. Journal of Health and Social Behavior 1990; 31:148–161 [PubMed] [Google Scholar]
- 27.Wethington E, Kessler RC: Perceived support, received support, and adjustment to stressful life events. J Health Soc Behav 1986; 27:78–89 [PubMed] [Google Scholar]
- 28.American Psychological Association: Stress management: How to strengthen your social support network, 2019
- 29.Stice E, Rohde P, Gau J, et al. : Relation of Depression to Perceived Social Support: Results from a Randomized Adolescent Depression Prevention Trial. Behaviour research and therapy 2011; 49:361–366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hamilton JL, Burke TA, Stange JP, et al. : Trait Affect, Emotion Regulation, and the Generation of Negative and Positive Interpersonal Events. Behavior Therapy 2017; 48:435–447 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Barrera M: Distinctions Between Social Support Concepts, Measures, and Models, 1986
- 32.Hogan BE, Linden W, Najarian B: Social support interventions: Do they work? Clinical Psychology Review 2002; 22:381–440 [DOI] [PubMed] [Google Scholar]